Improving Medication Adherence
in COPD with an Effective Device
Orapan Poachanukoon, MD.
เนื้ อหา
ั ยทีม
ปัจจั
่ ผ
ี ลตอการตกสะสมของยา
่
อุปกรณพ
ดตางๆ
์ นยาชนิ
่
่
วิธก
ี ารเลือกอุปกรณพ
เ่ หมาะสมกับผู้ป่วย
์ นยาที
่
Particle deposition in the respiratory tract
Relationship between aerodynamic chamber and lung deposition
Total
Oropharynx
Bronchial/
Conducting
airways
Alveolar
Laube et al Eur Respir J 2011; 37: 1308–1331.
Factor affecting deposition of aerosols in lung
Physical
Ventilatory
Particle size
Particle shape
Particle density
Humidity
Temperature
Tidal volume
Inspiratory flow
Breath-hold time
Breathing frequency
Nose vs mouth
breathing
Anatomic
Airway
diameter
Age
Disease
Rubin BK, Fink JB. Respir Care Clin N Am 2001;7:175-213.
Patient-related variables impacting correct device use
Pulmonary function and disease stage
Smoking status, age, sex, being overweight
Comorbidities
Manual dexterity
Ability to understand and follow instructions
Eyesight
Psychosocial issues
Fink JB et al. COPD 2013;10: 1-13.
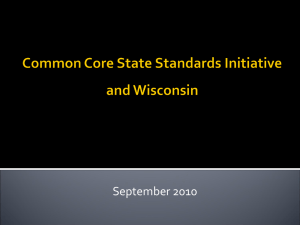
Patient’s inhaler device preference in COPD
Increased patient satisfaction and preference with a device can
help optimize patient adherence to treatment1,2.
Factors affecting patient preferences:
Perceived efficacy of device by patients
Ability to use a given inhaler easily
Psychological or physical issues
o Such as comorbidities (neuromuscular disorders and arthritis) can
impact inhaler technique.
Inhaler features
considered “very
important” by
COPD patients
(Data from Moore and Stone 2004)
1. Anderson et al. ERR 2005
2. Jones et al. PCRJ 2004
Restrepo et al. Int J COPD 2008:3(3) 371-384
Nebulizers
Aerosol
devices
pMDI
DPI
MDI vs MDI with Spacer
Spacer devices
E
Nebuchamber
Aerochamber
Valved holding chamber
Babyhaler
ACE spacer
Volumatric
DIY Spacer
DIY
Petty patent of Thailand No. 5479
AWARDS
• 2013. Gold Prize in International Exhibition of Inventions of
Geneva.Swiss Confederation. 10-14 April 2013
• 2013. Special Award from Taiwan Invention Association.
• 2012. Silver Prize in SII: Korea
• 2012. Excellence Award “Thai-ASEAN”
Thaksin University National Conference.
DIY SPACER on
THAMMASAT DIY SPACER
https://www.youtube.com/watch?v=XeTBTJLnWyg
่ ยพ่นยา TU Asthma Club
อุปกรณ์ชว
https://www.youtube.com/watch?v=kMbXeOo6S3I
www.tuasthmaclub.com
Clinical efficacy of spacer therapy with/without
electrostatic charge
This study showed no negative influence of ESC
on plastic spacers in children with asthma.
Arch. Dis. Child. 2001;84;178-182.
Dry Powder Inhaler (DPI)
DPI
MDI
MDI and DPI:
advantages and disadvantages
Advantages
Disadvantages
Portable and compact
Coordination of actuation and inhalation needed
Short treatment time
Most patients inhale too fast
No contamination risk
Important to prime before first use
High reproducibility between doses
Often difficult to determine remaining doses
Spacers available for some devices
Spacers more expensive and less portable
No coordination required
Forceful inhalation needed to aerosolize particles
Not to be used with spacer
More expensive than MDIs
Portable and compact; multi-dose
Only used with drug that is dispensed with the device
devices available
Single-dose devices with doses kept
Must be kept upright or horizontal during inhalation
separately in sealed packs
Breath actuated
Patients not to exhale into device once prepared
Short treatment time
Single devices require repeat loading
Chrystyn & Price. Prim Care Resp J 2009; Laube et al. Eur Respir J 2011
DPI
MDI
MDI and DPI:
advantages and disadvantages
Advantages
Disadvantages
Portable and compact
Coordination of actuation and inhalation needed
Short treatment time
Most patients inhale too fast
No contamination risk
Important to prime before first use
High reproducibility between doses
Often difficult to determine remaining doses
Spacers available for some devices
Spacers more expensive and less portable
No coordination required
Forceful inhalation needed to aerosolize particles
Not to be used with spacer
More expensive than MDIs
Portable and compact; multi-dose
Only used with drug that is dispensed with the device
devices available
Single-dose devices with doses kept
Must be kept upright or horizontal during inhalation
separately in sealed packs
Breath actuated
Patients not to exhale into device once prepared
Short treatment time
Single devices require repeat loading
Chrystyn & Price. Prim Care Resp J 2009; Laube et al. Eur Respir J 2011
Why dry powder inhalers?
Automatic co-ordination of inhalation and drug release1,2:
– reduces patient errors associated with need to
co-ordinate inhalation and drug release
Dose counting or low warning (multi-dose DPIs)
– also a feature of newer pMDIs
Lack of propellant is environmentally friendly3
– although plastics content, electronics (with some devices) and fewer
doses per device may contribute to a less environmentally friendly
profile
1. Ashurst, et al. Pharm Sci Technol Today 2000; 2. Newman, Busse. Respir Med 2002
3. Byron. PATS 2004
Lung deposition of devices
Respir Care Clin N Am 2001
How to choose right aerosol delivery device
Poor coordination
Good coordination
Inspiratory flow
> 30 L/min
Inspiratory flow
< 30 L/min
Inspiratory flow
> 30 L/min
Inspiratory flow
< 30 L/min
pMDI
pMDI
pMDI+spacer
pMDI+spacer
DPI
Nebulizer
DPI
Nebulizer
Nebulizer
Nebulizer
Laube et al Eur Respir J 2011; 37: 1308–1331.
Evaluating Drug Delivery of DPI
Inspiratory Flow
Device Resistance
Fine Particle Mass
Airflow resistance in DPIs
120
Flow rate (L/min)
100
80
60
40
2.2 10-2 kPa1/2 L-1 min
2.7 10-2 kPa1/2 L-1 min
3.4 10-2 kPa1/2 L-1 min
5.1 10-2 kPa1/2 L-1 min
Breezhaler
Diskus
Turbuhaler
Handihaler
20
0
0
2
4
6
Inspiratory effort (kPa)
8
10
Singh D et al. ATS 2010 (poster)
Peak inspiratory flow rate (PIFR) Breezhaler was not affected
by COPD severity
• Patients with mild to very severe COPD achieved a flow rate of
≥60 L/min (>18.9 cmH2O pressure drop) using Breezhaler®
140
PIFR (L/min)
120
100
80
60
40
20
0
Mild
N=26 COPD patients
Moderate
Moderate/
severe
Severe
Very
severe
COPD severity
Peak inspiratory flow rates via the device were determined in patients with
COPD using an Inhalation Profile Recorder. Each bar represents one patient Pavkov et al. CMRO 2010; 26 (11): 2527-2533
Particle size &
Dose Regional Deposition in Lung
• Delivered dose are usually in range of 75%-90% of metered dose.
• FPD/FPM are very much dependent from formulation and delivery system but never 100% of delivered dose.
Consistent results for fine particle mass
Indacaterol 150 µg
Indacaterol 300 µg
60
120
42
43
45
47
48
38
40
34
30
100
Fine Particle Mass (μg)
Fine Particle Mass (μg)
50
101
27
20
10
85
80
60
90
106 103
93
72
54
40
20
0
0
30
40
50
60
70
80
90
100
Flow Rate (L/min)
** Fine particle mass = drug particles <4.7 μm in diameter
30
40
50
60
70
80
90
100
Flow Rate (L/min)
Pavkov et al. CMRO 2010; 26 (11): 2527-2533
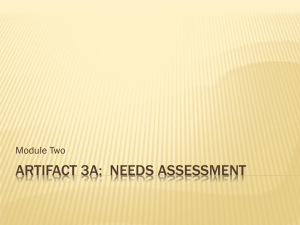
Estimated drug deposition in Breezhaler® and HandiHaler®
35
Intrathoracic deposition
(% of delivered dose)
30
Patient
25
20
15
10
5
0
1
2
3
4
5
Breezhaler
6
7
Mean
±SD
1
2
3
4
5
Handihaler
6
7
Mean
±SD
Particles <5 μm have greatest potential for lung deposition1
FPF (proportion of particles <5 μm) was higher with Breezhaler (27%) vs HandiHaler (10%)2
Mean estimated intrathoracic drug deposition: 31% Breezhaler; 22% HandiHaler2
Mean estimated extrathoracic drug deposition: 57% Breezhaler; 71% HandiHaler2
1. Laube et al. Eur Respir J 2011; 2. Chapman et al. Int J COPD 2011
Breezhaler-new capsule based DPI
Low airflow
resistance
Easy to use,
Feedback on
correct use
Taste,
Transparent
Reasons for Non-adherence
complexity
of treatment, S/E
Possible avoidance
patient education
difficult to access
cost/reimbursement
patients features
chronicity
Pt/HCW partnership
Impact on adherence
Technique to improve adherence to aerosol medications
Written explanation and demonstration
Have patient bring medication to every appointment
and check technique at each visit
Ask the patient specifically about adherence
Follow up on unfilled and refilled
Minimized medications, keep it simple
Parents need to take responsibility
(> 13 years take medicine independently)
Respiratory care 2011.
ขอบคุณคะ่
Please visit us at www.tuasthmaclub.com