Preparing for
Direct Acting Antivirals (DAAs)
in Practice—New Paradigms in
the Management of HCV
Sherilyn C. Brinkley, MSN, CRNP
Nurse Practitioner/Program Manager
Infectious Disease Department
Johns Hopkins University
Baltimore, Maryland
HCV Standard of Care 2011
HCV Genotype 1
Peginterferon,
weekly
Ribavirin,
weight-based, daily
Boceprevir or
telaprevir, thrice
daily
Duration variable based on regimen used
and on-treatment viral kinetics
HCV Genotypes 2 and 31
Peginterferon,
weekly
Ribavirin,
800 mg, daily
Duration 24 weeks
HCV Genotypes 41
Peginterferon,
weekly
Ribavirin,
weight-based, daily
Duration 48 weeks
Ghany MG, et al. Hepatology. 2009;49:1335-1374.
Preparing for Anti-HCV Therapy
Case Study—Carmen
• Carmen is a 59-year-old female from Puerto
Rico diagnosed with chronic HCV in 1999
after moving to the United States and
starting job as medical assistant
– Previously evaluated and treated by a
gastroenterologist but fell out of care in 2004
– Reports taking peginterferon and ribavirin for
48 weeks leading to an undetectable viral load
followed by relapse
• She heard about new anti-HCV drugs with
shorter duration and wants more information
Who Is a Candidate for Anti-HCV
Treatment with DAAs?
• Adults with chronic HCV genotype-1 infection
• Treatment-naive or prior relapsers or
nonresponders
• If cirrhotic, should be compensated
• Ability to adhere to dosing (peginterferon,
ribavirin, and protease inhibitor) and monitoring
schedule
The protease inhibitor is never used
as monotherapy
Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
Who Is NOT a Treatment Candidate?
• Contraindications to peginterferon/ribavirin apply
• Planning for pregnancy or unwilling to use adequate
contraception
• Coadministration of contraindicated drugs
– Highly dependent on CYP3A for clearance
– Strongly induce CYP3A
• Special populations where safety and efficacy not
established
–
–
–
–
Organ transplant
End-stage liver disease
Coinfected with HIV or HBV
Pediatrics
Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
What Are Key Components of
HCV Evaluation?
• Basic lab tests
– HCV RNA by PCR, genotype, complete metabolic
panel, prothrombin time/international normalized
ratio, thyroid stimulating hormone, pregnancy test
• Liver histology assessment (as needed)
– Liver biopsy
– Fibrosis markers
• Comorbid disease status
• Gauge patient motivation to take anti-HCV
therapy
Carmen’s Laboratory Findings
Test
Hemoglobin (g/dL)
Platelets (/mm3)
Result
Reference Range
13.1
12–16.0 g/dL
160,000
150,000–400,000
ALT (U/L)
88
Bilirubin, total (mg/dL)
0.7
<1.0
Albumin (g/dL)
4.2
3.5–5.5
Creatinine (mg/dL)
1.1
0.6–1.2
International Normalized Ratio
1.0
1.0–1.2
HCV RNA
ALT (U/L)
1.8 x 109 IU/mL
HCV genotype
1a
Body mass index
29
Liver biopsy
Metavir grade 2 inflammation
Stage 3 bridging fibrosis
Carmen’s Comorbidities and
Current Medications
• Comorbidities
–
–
–
–
Hypertension
Coronary artery disease
Hyperlipidemia
Insomnia
• Current medications
–
–
–
–
Simvastatin
Aspirin
Trazodone
Atenolol
How Do You Prepare Patients
for Therapy?
• Educate about treatment regimens and potential
side effects
• Discuss adherence to medications,
administration schedule, food requirements,
monitoring schedule
• Explain variable treatment durations and futility
rules
• Review current medications, herbal products,
and supplements for drug interactions
• Counsel regarding pregnancy risk and
contraception
How Do You Prepare Your Practice
Setting for Integration of DAAs?
• Ensure adequate appointment time for patient
counseling
• Limit number of patients starting treatment each
week to avoid clinic volume overload
• Use treatment initiation checklist
• Use pocket guides for drug interactions,
response-guided therapy, and futility rules
• Delegate tasks to others when appropriate
– Prior authorizations
– Medication administration teaching
– Specialty pharmacy services
Carmen’s Follow-Up Appointment
• Carmen presents to clinic to review labs and
biopsy results
• Decision is made to treat with peginterferon,
ribavirin, and a protease inhibitor
• Next steps
– Discuss side effects and lessons learned from prior
therapy
– Review current medication list for drug-drug
interactions and discuss plan for changes
– Consult patient’s cardiologist regarding clearance for
treatment and an alternative lipid-lowering agent
Treatment Goals and
Challenges
Why Treat Chronic HCV?
• Sustained virologic response (SVR) is
achievable
• SVR is associated with gradual
regression of fibrosis
• SVR is associated with lower risk of liver
failure and hepatocellular carcinoma
Pearlman BL, et al. Clin Infect Dis. 2011;52:889-900.
What Are the Benefits of Using DAAs?
• Higher SVR rates observed across all
patient groups1-4
– Previously untreated, relapsers, partial and
null responders
• Response-guided therapy allows for 24or 28-week duration for most treatmentnaive patients with rapid response5,6
1. Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416. 2. Poordad F, et al. N Engl J Med.
2011;364:1195-1206. 3. Zeuzem S, et al. N Engl J Med. 2011;364:2417-2428. 4. Bacon BR, et al. N Engl
J Med. 2011;364:1207-1217. 5. Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation;
2011. 6. Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
Protease Inhibitor
Phase III Clinical Trials
Boceprevir
Telaprevir
SPRINT-21
Naive
ADVANCE3
Naive
RESPOND-22
Nonresponders
ILLUMINATE4
Naive
REALIZE5
Nonresponders
1. Poordad F, et al. N Engl J Med. 2011;364:1195-1206. 2. Bacon BR, et al. N Engl J Med.
2011;364:1207-1217. 3. Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416. 4. Sherman KE, et al.
61st AASLD; October 29-November 2, 2010; Boston, Mass. Abstract LB-2. 5. Zeuzem S, et al. N Engl J
Med. 2011;364:2417-2428.
SPRINT-2—Boceprevir in Treatment-Naive
Genotype-1 Patients
Two cohorts: 1, nonblack; 2, black.
Abbreviations: B, boceprevir 800 mg TID; P, peginterferon -2b 1.5 µg/kg/wk; R, ribavirin 600–1400 mg/d;
RGT, response-guided therapy; TW, treatment week.
Poordad F, et al. N Engl J Med. 2011;364:1195-1206.
SPRINT-2—SVR by Cohort and
Treatment Arm
Poordad F, et al. N Engl J Med. 2011;364:1195-1206.
RESPOND-2—Boceprevir in Genotype-1
Prior Nonresponders
Abbreviations: B, boceprevir 800 mg TID; P, peginterferon -2b 1.5 µg/kg/wk; R, ribavirin 600–1400 mg/d;
RGT, response-guided therapy; TW, treatment week.
Bacon BR, et al. N Engl J Med. 2011;364:1207-1217.
RESPOND-2—SVR by Prior Response
Abbreviations: B, boceprevir 800 mg TID; P, peginterferon -2b 1.5 µg/kg/wk; R, ribavirin 600–1400 mg/d;
RGT, response-guided therapy.
Bacon BR, et al. N Engl J Med. 2011;364:1207-1217.
ADVANCE—Telaprevir in Treatment-Naive
Genotype-1 Patients
Abbreviations: eRVR, extended rapid virologic response (undetectable HCV RNA at weeks 4 and 12);
P, peginterferon -2a 180 µg/wk; R, ribavirin 1000–1200 mg/d; T, telaprevir 750 mg q8h.
Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416.
ADVANCE—SVR Rates
Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416
REALIZE—Telaprevir in Genotype-1
Prior Nonresponders
Abbreviations: P, peginterferon -2a 180 µg/wk; R, ribavirin 1000–1200 mg/d; T, telaprevir 750 mg q8h.
Zeuzem S, et al. N Engl J Med. 2011;364:2417-2428.
REALIZE—SVR by Prior Response
Abbreviations: LI, lead-in; P, peginterferon -2a 180 µg/wk; R, ribavirin 1000–1200 mg/d;
T, telaprevir 750 mg q8h.
Zeuzem S, et al. N Engl J Med. 2011;364:2417-2428.
What Are the Challenges of Triple
Combination Therapy?
• Increased complexity
– Protease inhibitor dosed every 8 hours
– Food requirements
– High pill burden
• More adverse effects
• Frequent lab monitoring and clinic visits
• Emergence of resistance-associated
variants if SVR not achieved
• Increased cost
Using Response-Guided
Therapy
How Does Response-Guided
Therapy Impact Treatment
Duration?
• Both boceprevir and telaprevir use a
response-guided therapy approach
• Allows on-treatment virologic response to
dictate treatment duration among
noncirrhotics
• Early response is the goal and may allow
for a shorter duration of therapy
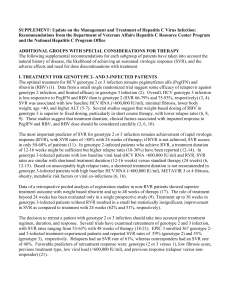
Boceprevir—Response-Guided
Therapy
For all patients: peginterferon/ribavirin only weeks
1 through 4, then add boceprevir
HCV RNA
Results
Undetectable
HCV RNA at
weeks 8 and 24
Detectable
HCV RNA at
week 8
Treatment-Naive
Patients
Previous Partial
Responders and Relapsers
Complete triple therapy at
week 28
Complete triple therapy at
week 36
Continue triple therapy through week 36, then administer
peginterferon/ribavirin only through week 48
Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
Boceprevir—Additional Duration
Instruction
• Response-guided therapy was not studied in patients
who did not achieve early virologic response (<2-log drop
in HCV RNA by week 12) during prior therapy
– These patients should receive 4 weeks of peginterferon/ribavirin
followed by 44 weeks of triple therapy
• For treatment-naive patients who have a poor response
(<1-log drop in HCV RNA) to peginterferon/ribavirin after
the 4-week lead-in phase, consider extending boceprevir
in combination with peginterferon/ribavirin through
week 48
Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
Telaprevir—Response-Guided
Therapy
For all patients: telaprevir, peginterferon, and
ribavirin start on day 1
HCV RNA
Results
Undetectable
HCV RNA at
weeks 4 and 12
Detectable
HCV RNA at
weeks 4 and/or
12
Treatment-Naive Patients
and Prior Relapsers
Continue triple therapy
through week 12, then
administer
peginterferon/ribavirin only
through week 24
Continue triple therapy
through week 12, then
administer
peginterferon/ribavirin only
through week 48
Prior Partial and Null
Responders
Continue triple therapy
through week 12, then
administer
peginterferon/ribavirin only
through week 48
Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
Should Response-Guided Therapy
Be Used in Cirrhotics?
• Boceprevir1
– Patients with compensated cirrhosis should receive
4 weeks of peginterferon alfa and ribavirin followed
by 44 weeks of triple therapy
• Telaprevir2
– Treatment-naive patients with cirrhosis who have
undetectable HCV-RNA at weeks 4 and 12 of
telaprevir combination treatment may benefit from
an additional 36 weeks of peginterferon/ribavirin
(48 weeks total)
1. Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
2. Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
What If a Patient Has a Poor
Virologic Response?
• Futility (stopping) rules are guidelines that
require discontinuation of treatment
medications at specific time points in the
event of inadequate response
• Stopping rules for futility
– Decrease drug exposure
– Minimize emergence of resistance
– Lower cost
Boceprevir—Futility (Stopping)
Rules
Week
12
HCV RNA
Result
≥100 IU/mL
Action
Stop all 3 medications
24
Detectable
Stop all 3 medications
Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
Telaprevir—Futility (Stopping)
Rules
Week
4
HCV RNA
Result
>1000 IU/mL
Action
Stop all 3 medications
12
>1000 IU/mL
Stop all 3 medications
24
Detectable
Stop peginterferon/ribavirin
(telaprevir already stopped
at week 12)
Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
What Are the Implications of
Inadequate Virologic Response?
• HCV has rapid viral dynamics and high mutation rate1
• Baseline resistance mutations exist
– 7% of population in boceprevir trials2
– 5% of population in telaprevir trials3
– Some achieve SVR regardless2,3
• Majority of patients with protease inhibitor treatment failure
are left with resistant variants2,3
• Predominant strain returns to wild type in majority within
2 years4,5
• Cross resistance with other protease inhibitors
anticipated1
• Long-term clinical impact unknown
1. Kieffer TL, et al. J Antimicrob Chemother. 2010;65:202-212. 2. Victrelis [package insert]. Whitehouse
Station, NJ: Schering Corporation; 2011. 3. Incivek [package insert]. Cambridge, MA: Vertex
Pharmaceuticals Incorporated; 2011. 4. Vierling JM, et al. 46th EASL; April 14-18, 2010; Berlin, Germany.
Abstract 2016. 5. Sullivan JC, et al. 47th EASL; March 30-April 3, 2011; Barcelona, Spain. Abstract 8.
Safety Considerations
with DAAs
Are There Drugs to Avoid with
Protease Inhibitors?
• Boceprevir and telaprevir are inhibitors of CYP3A1,2
• Use of boceprevir or telaprevir with drugs/herbs
metabolized by CYP3A may lead to1,2
– Altered drug concentrations
– Loss of therapeutic activity
– Adverse events from toxicity
• Refer to lists of contraindicated drugs and drugs to use
with caution in FDA-approved product package inserts1,2
• Use drug-drug interaction pocket guide and refer to drug
interaction websites
– http://www.hep-druginteractions.org/
• Review patient medication/supplement list at each
patient interaction
1. Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
2. Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
Are There Additional Contraceptive
Requirements with DAAs?
• Ribavirin may cause birth defects and fetal death
• Negative pregnancy test prior to therapy and
monthly
• 2 forms of contraception during therapy and for
6 months posttherapy
– Systemic hormonal contraception should not be relied
upon as effective method during protease inhibitor use
• Decreased ethinyl estradiol concentrations
– Use 2 effective nonhormonal methods of contraception
(barrier methods or nonhormonal IUD)
Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
What Are the Most Common Side
Effects with Protease Inhibitors?
• Boceprevir (≥35% of subjects)1
– Fatigue, anemia, nausea, headache,
dysgeusia
• Telaprevir (≥5% higher than in controls)2
– Rash, pruritus, anemia, nausea,
hemorrhoids, diarrhea, anorectal discomfort,
dysgeusia, fatigue, vomiting, anal pruritus
1. Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
2. Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
Anemia Management Is a Mainstay
of Anti-HCV Therapy
• Increased anemia with boceprevir and telaprevir
• Hematologic parameters at baseline and
treatment weeks 2, 4, 8, 12, and periodically
after–typically every 4 weeks–or more frequently
as clinically indicated
• Utilize anemia management tools employed with
peginterferon and ribavirin
– Ribavirin dose reduction
– Erythropoietin
– Never dose reduce protease inhibitor
Victrelis [package insert]. Whitehouse Station, NJ: Schering Corporation; 2011.
Incivek [package insert]. Cambridge, MA: Vertex Pharmaceuticals Incorporated; 2011.
Adherence Equals Safety
Adherence with medication regimen is
critical but only part of the story
Medication regimen
Lab schedule
Adherence
with…
Clinic appointment
schedule
Drug interactions schedule
Contraception
Carmen’s Pretreatment
Counseling
• Select medication dosing schedule every 7−9 hours for
protease inhibitor
• Customize written daily schedule for taking ribavirin and
protease inhibitor with detailed food requirements
• Reinforce adherence with doses, labs, and clinic visits
• Instruct to not take new medications, supplements, or
herbals without provider clearance
• Emphasize to never discontinue or dose reduce the
protease inhibitor
• Review side effects of protease inhibitor, peginterferon,
and ribavirin
Carmen’s Pretreatment
Counseling
• Discuss and document contraceptive plan
– Postmenopausal
– Vasectomy
• Review response-guided therapy and potential
treatment durations
• Explain rationale for futility rules
• Review clinic/provider contact information
• Provide lab requisitions, lab schedule, next
appointment reminder
• Demonstrate peginterferon injection
Carmen Begins Triple Therapy
• She leaves with lab orders for end of treatment
weeks 2 and 4
• She has a follow-up visit scheduled in 2 weeks
• She will begin treatment the next day after
breakfast
– 1st telaprevir and ribavirin doses at 7:00 am
– 1st peginterferon dose planned for 6:00 pm
• She remembers the flu-like symptoms with
peginterferon from prior therapy and plans to
premedicate with ibuprofen
• She will enlist the support of her family
Summary
• DAAs improve SVR rates among all genotype-1
patient groups
• Triple therapy utilizes response-guided therapy
and potential for shortened treatment duration
• Anti-HCV treatment is increasingly complex
with drug-drug interactions, increased pill
burden and dosing frequency, risk of protease
inhibitor resistance, and more side effects
• Pretreatment education requires adequate time
and detail to prepare patients for treatment
success
Thank you for your participation.
To earn CME/CE credit, please complete the posttest
and evaluation. (Click link in the navigation bar above
or to the left of the slide presentation.)
Your feedback is appreciated and will help us
continue to provide you with clinically relevant
educational activities that meet your specific needs.