2012NationalConferenceMoss
advertisement

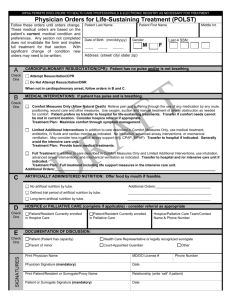
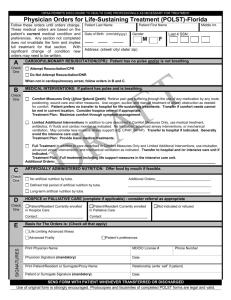
FINE TUNING THE POLST SYSTEM: THE CASE OF AN INVALID, CONTRADICTORY POLST FORM Alvin (Woody) Moss MD, WVU Center for Health Ethics and Law* Margaret Carley JD, RN OHSU Center for Ethics in Health Care* Terri Schmidt MD, MS, Oregon Health & Science University (EMS)* Paul Schneider MD, VA Medical Center, Los Angeles, CA Kenneth Zeri RN, MS, Hospice Hawaii* 1 *National POLST Paradigm Task Force members Current as of January 3, 2012 2 www.polst.org A 78 year-old woman was admitted from a nursing home with chest pain. She had a past history of coronary artery disease status post stent placement, congestive heart failure, hypertension, lipid disorder, and mild dementia. A POLST form accompanied the patient and indicated CPR in Section A and limited additional interventions in Section B. The attending physician wondered what he should do with the POLST form because Section A and Section B seemed to be contradictory. The POLST form had been prepared by a social worker who had signed it, but there was no physician signature on it. 3 In transporting the patient, EMS worried, “What do I do if she codes and I do CPR and get her back, but she is not breathing normally? Do I intubate her?” The ED physician wondered the same thing, but fortunately she did not suffer a cardiac arrest. When interviewed by the palliative care team who was consulted to address the POLST form inconsistency, the patient indicated that she would not want to be kept alive on machines and when it was explained to her that if she had CPR and lived through it, it was very likely that she would end up being on a breathing machine. She said, “Well then, I don’t want CPR.” 4 The patient was questioned, and she clearly understood that without CPR in the event of a cardiorespiratory arrest she would die. She was felt to have decision-making capacity for her decision. A daughter who lived out of state was the patient’s Medical Power of Attorney representative and wanted her mother to have CPR. What should be done with regard to the seemingly contradictory POLST form and the conflict between the patient and her daughter? How could these situations be prevented in the future? 5 Where Was the Problem in This Case? Can we expect POLST preparation to be any more accurate/functional than the rest of our somewhat inaccurate/dysfunctional system? If so, how? Who should “own” POLST and what control should they exert? In code discussions, when will providers demonstrate the moral courage to use the word “die”? “If God forbid you were to die during this hospitalization, would you want us to try to bring you back from death?” 6 Where Was the Problem in This Case? What was the role of the physician in this case? The SCBCC struggled mightily over this question and concluded physicians must at least personally confirm the discussion when initially prepared by a non-physician. My hospital mandates an MD POLST discussion. VA does not allow resident, licensed physicians to sign DNR orders > 24 hrs. Therefore, they should not sign most POLSTs. 7 Does the patient have capacity ? Does the patient have capacity How, when and who would make this determination this in your state? When can the appointed health care representatives begin to make health care decisions? What happens if the patient does not have capacity and there is no one available to make health care decisions? 8 Can a family member override the existing POLST Orders? State by state variations attributable to different advance directives and surrogate decision maker statutes May depend on if your POLST program is statutory, regulatory or voluntary Outside the hospital it may depend on your out-of- hospital DNR statute or rules May depend upon statutory or regulatory limitations based on the client’s medical conditions 9 May Be Multiple Family Member Roles Informal roles of family members Primary Caregiver Primary Decision Maker Spokesperson Out-of-Towner Patient Wishes Expert Protector/Vulnerable Member Health Care Expert End-of-Life Decision Making in Adult ICUs: Roles & Relationships of Key Players Judith Gedney Baggs, PhD, RN, FAAN 10 Minimizing or avoiding conflicts by a better goals of care conversation Advance Care planning Goals of Care Communication What do patients and families want? Better communication by clinicians Timely, on-going, clear, complete, compassionate Address condition, prognosis, treatments Patient-focused health care decision making Aligned with patient values, care goals, preferences Nelson, Puntillo, et al. (2010), In their own words. Critical Care Medicine 11 .Was this a burdensome transition of care from nursing home to hospital? “Health care transitions, such as the hospitalization of nursing home residents, have the potential for fragmentation of care, changes in the management of chronic diseases, duplication of diagnostic workups, and medical errors.” NEJM Study Results Among 474,829 nursing home decedents, 19.0% had at least one burdensome transition(range, 2.1% in Alaska to 37.5% in Louisiana). In adjusted analyses, blacks, Hispanics, and those without an advance directive were at increased risk. Nursing home residents in regions in the highest quintile of burdensome transitions (as compared with those in the lowest quintile) were significantly more likely to have a feeding tube, have spent time in an ICU in the last month of life have a stage IV decubitus ulcer , or have had a late enrollment in hospice. Gozalo P, Teno JM, Mitchell SL, et al. End-of-Life Transitions among Nursing Home Residents with Cognitive Issues. N Engl J Med 2011;365:1212-21. 12 EMS Conflicting Section A and B orders Section A DNR Section A Resus Section A Resus Section B Full Treatment Section B Comfort Measures Section B Limited Interventions What should EMS do? 13 What is the trump card? POLST form Patient choice Family/surrogate choice (Does it matter if it is a legal guardian? Power of attorney for health care?) 14 Hospice Care Staff must know basic laws governing POLST in state Hospice care across most settings Home, SNF, Hospital, Care Home, Hospice Facility, Homeless POLST “Form” may be voluntary for healthcare institutions to use, but POLST “Orders” may be mandatory to follow Legal requirements for correct document 15 Hospice Care Home based care Clarifying goals for care Including family Policies regarding completing forms Nursing Facility / Hospice Collaboration Support Facility staff in review & clarification of POLST Hospice team (MD, RN, MSW) support resolution of conflict Policies governing use of form POLST is voluntary 16 REGIONAL LUNCH DISCUSSIONS 17 Regions California – Aviary Ballroom Midwest – Beach South IL, IA, MN, NE, MO, MI, OH, WI Northeast – Beach South DE, ME, NH, NJ, NY, PA, RI, DC South – Beach South FL, GA, KY, LA, NC, TN, TX, VA, WV West – Beach South CO, HI, ID, MT, NM, OR, UT, WA 18