Part One: Insulin Initiation
advertisement

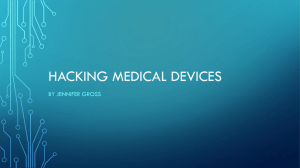
Does the patient need insulin? • Not achieving target HbA1c 50-55 mmol/mol • 1. Doing as much as possible re diet and exercise • • • • Gym membership deals Advice on food: types and amount Bariatric Surgery; Optifast Willingness to change? • 2. Taking maximum doses of oral medication • • • • • Metformin can be continued until eGFR<30ml/min Gliclazide 320mg/day; Glipizide 30mg/day Pioglitazone for young, obese Don’t forget Acarbose Drug adherence? Checking with patient and with dispensing • 3. Is the patient actually primarily insulin deficient (rather than insulin resistant): – Suboptimal HbA1c and slim with weight loss • BMI <= 25; – Overweight patient with duration of diabetes > 10 years; previously good glycaemic control on oral agents • 4. Is the target HbA1c realistic for the patient: – Frail, elderly, mentally ill: trigger HbA1c for commencement of insulin may be higher (e.g. HbA1c> 65 mmol/mol) Type 2 diabetes is a progressive disease that requires progressive treatment ß-cell function and insulin secretion progressively decline in type 2 diabetes Diagnosis of type 2 diabetes Is insulin going to be effective? • 1. How much is the patient prepared to do? – Testing regularly: need to know the blood glucose (BG) profile to work out the best insulin regime – Learning how to self-inject – Learning how to adjust the doses • 2. How much are you and your nurse prepared to do? – Teaching how to inject – Supervising titration of dose in a timely manner – Giving advice on dose adjustment for meal content, exercise if on multidose regime Education Required • • • • • • • Lifestyle advice; BG monitoring Use of insulin pens Injection technique Insulin action, timing of injections, storage Disposal of sharps Hypo management, prevention Sick day management How many injections per day? • How many is the patient prepared to do? • How high is the HbA1c? Are the oral agents providing any benefit? – Likely if HbA1c is between 55 and 75 mmol/mol: • Once daily insulin added on to oral agents indicated – HbA1c > 75: oral agents failing and full switch to insulin may be best. Insulin therapy. Once daily basal insulin • Glargine (Lantus) vs. Isophane (Protophane/Humulin NPH) – NZ Guideline Group (NZGG): Isophane – Commonly used: Glargine • Isophane: cheaper, long and safe track record, 12-18 hours of action – Protophane: Novo pen; Humulin NPH: Luxura pen • i.e. no real difference between the two brands but specific pen needs to be given Basal Insulin: provides background insulin but does not cover meals Isophane Glargine •Schematic action profiles, theoretical representation of insulin injected once a day - results may vary from patient to patient. Once daily Isophane insulin (Protophane or Humulin NPH): Indications • Night dose: Good for patients whose blood sugars climb overnight but have even control during the day due to oral agents: – Continue oral agents and prescribe Isophane insulin at 8-9pm • Morning dose: Elderly patients often do not need much diabetes treatment overnight (reduced hepatic gluconeogenesis) and also useful for those on Prednisone mane – Fasting BG 4-6 but climb during the day – Continue oral agents and prescribe Isophane insulin at 8-9am What are the pros and cons of the Novopen vs. the Luxura? • Novopen – slightly bigger numbers – its mechanism makes counting the clicks (for the sight impaired ) a little easier. – need to pull the end out first before dialing up • Luxura (Huma Pen) – heavier – mechanism feels a little looser - possibly easier to make mistakes – you just dial. Isophane insulin: Starting Dose • NZGG suggest 10 units starting dose – Insulin requirement relates to body weight – If patient > 50kg, expect the dose will need to climb • If patient overweight (BMI > 30) or HbA1c > 65 mmol/mol, suggest start at a higher dose, e.g. 0.2 units/kg body weight/day – e.g. 100kg patient will likely need at least 20 units Glargine (Lantus) insulin • Only funded long-acting insulin analogue (Levemir not funded) • Concerns about potential cancer risk have been disputed • 24 hour action for approximately 70-80% patients • Constant insulin profile with no peak action – can be given at any time of the day so long as the same time each day • More sensitive to heat than other insulins Glargine (Lantus) Insulin • Given either with disposable pen (Solostar Pen) or in penfill used in ClikSTAR Pen – If prescribe Solostar, no need to provide pen and no need for patient to refill pen, but more waste • Solostar Pen ready filled and dispensed at pharmacy – ClikSTAR pen: satisfactory but not as robust as NovoPen/Luxura pen: • Large numbers, easy to see Once daily Glargine (Lantus): Indications • 24 hour basal insulin needed: BG high in the morning and climb over the day • HbA1c > 65 despite maximum oral agents • An introduction to insulin for those who really need full insulin cover but reluctant/unwilling; more coverage than Isophane – No need to time Glargine insulin injection with meals – Still need to cover postprandial hyperglycaemia with something (oral agents or insulin) The problem with type 2 diabetes The mealtime insulin secretory response is blunted… ...resulting in undesired mealtime glucose excursions Both fasting & mealtime glucose contribute to HbA1c • Clinical evidence suggests that reducing PPG excursions is as important, or perhaps more important than fasting blood glucose (FBG), for achieving HbA1c goals Oral hpoglycaemic agents (OHA) and basal insulin – Tempting to stop all OHA and just have one injection per day • Will achieve better control than no treatment • Can result in worse control if patient was taking oral medication as prescribed – Metformin useful agent to continue in most patients • • • • Reduces insulin resistance Treats post-prandial hyperglycaemia No hypoglycaemia due to Metformin itself Continue at same dose Suphonylureas and basal insulin • NZGG: – Once daily Isophane: continue Sulphonylurea – Twice daily Isophane: discontinue Sulphonylurea – If control just above target HbA1c, then this may work – But Isophane will not cover post-prandial hyperglycaemia: » If HbA1c > 65, continue Sulphonylurea • Once daily Glargine: similar to twice daily Isophane Some typical treatment regimens: OHA and basal insulin • Metformin 850mg tds, Gliclazide 160mg bd, Protophane 15 units nocte • Metformin 1gm tds, Humulin N 12 units bd • Gliclazide 80mg tds, Glargine 30 units daily (renal pt) Other OHA • Pioglitazone: usually discontinued at insulin commencement – Increased risk of fluid retention – But…. In young overweight patient maybe continued to help minimise the insulin dose • Acarbose: can be continued if useful Are OHA adding anything? • If HbA1c > 75 mmol/mol and pt taking the OHA at maximum doses, then probably not • If 2-hour post-prandial BG > 10, then probably not – Will depend on pre-prandial BG • Will need insulin to cover meals……unless patient can reduce carbohydrates / meal size Insulin Mealtime Cover Rapid-acting insulin Onset approx 10 minutes after injection. Duration of action around 1–3 hours. Rapid-acting insulin should be given immediately before a meal (or can be given soon after meals) Brand names: Humalog, NovoRapid, Apidra Short-acting insulin Onset approx 30 minutes after injection. Duration of action around 3-6 hours. Short-acting insulin should be given 20-30 minutes before a meal Brand names: Humulin R, Actrapid Short acting insulin – Actrapid and Humulin R not routinely used • Can be useful to try and cover both breakfast and lunch or extended evening food intake – E.g. children who do not want to inject at school – Adults who eat most of their food in the evening but over an extended period (probably better in a pre-mixed formulation) Rapid acting Insulins • Novorapid vs Humalog vs Apidra – No significant difference between them – Novorapid: Novo pen; slightly longer tail of action, up to 4-5 hours – Humalog: Luxura pen; action 3-4 hours – Apidra: disposable solostar pen; action 3-4 hrs Basal bolus insulin regimes • Basal insulin (Isophane or Glargine) taken once or twice daily • Bolus insulin (Novorapid, Humalog or Apidra) with meals • Standard regimen for type 1 diabetes • Becoming popular with insulin requiring type 2 pts – Most flexible insulin regimen • But… does require multiple insulin injections per day – Plus education about adjusting bolus insulin doses for variable meals Basal bolus regimens • Usual: Rapid acting insulin tds + Glargine mane or nocte • Examples of variations: – Glargine once daily + Apidra with main evening meal+ Metformin tds (can give Glargine and Apidra at same time) • Good for pt who eats large evening meal, snacks during day – Humulin N mane + Humalog with breakfast and lunch + Metformin tds • Pt on Prednisone 10mg mane for PMR • Can become somewhat complicated! Pre-mixed Insulins • Avoid complicated regimens in patients who need more than basal insulin + OHA • Cover background insulin requirements + meal cover • Two injections per day timed with breakfast and evening meals – Have to eat at these times – Good opportunity to stress importance of regular meals • Usually continue Metformin but discontinue sulphonylurea, other OHA Pre-mixed Insulins: Covering meals and giving basal cover • • A mixture of either rapid or shortacting and intermediate-acting insulin which act just like two injections of the separate components taken at the same time • Useful for many type 2 patients with tablet failure requiring insulin Pre-mixed Insulins: Short acting insulin + isophane – Penmix 30: 30% Actrapid, 70% Protophane – Penmix 50: 50% Actrapid, 70% Protophane – Humulin 30/70: 30% Humulin R, 70% Humulin N • Ideally injected 20 mins before meal • Actrapid/Humulin R longer duration of action – cover breakfast and lunch – but can linger and potentiate hypoglycaemia overnight • Most patients use Penmix 30 or Humulin 30 – Penmix 50 useful for big eaters Pre-mixed Insulins: Rapid acting insulin + isophane – Humalog Mix 25: 25% Humalog, 75% Humulin N – Novomix 30: 30% Novorapid, 70% Protophane – Humalog Mix 50: 50% Humalog, 50% Humulin N • Cover breakfast and dinner well, but not lunch – Inject when meal served or just after • Most patients use Humalog Mix 25 or Novomix 30: – Not much difference – Novomix 30: disposable pen • Humalog Mix 50 can be useful to cover large evening meal Pre-mixed Insulins • Pros – cover overnight hyperglycaemia and address postprandial excursions • • • – Humalog Mix/ Novomix: • Inject at meal-time • • Less likelihood pre-prandial hypoglycaemia Penmix/Humulin Mix • Improved cover lunch and late night snack • • Cons injections must be given at meal times; work best if regular time for breakfast and evening meal difficult to adjust dose if: – large variation in carbohdrate component of meal – sudden increase in physical activity Humalog/Novo Mix – Not good lunch cover Penmix/Humulin Mix – Inject 20 mins before meal Insulin prescription • Need to also prescribe insulin pen needles – We recommend 5mm needle length to ensure subcutaneous administration (rather than intramuscular) for most people • How to get around expected increase of dose? – Prescribe higher dose but instruct patient to start with lower dose? May cause confusion – Write on script that dose may be increased and repeats needed early – Write another script if supplies run out early Adjusting insulin doses • The patient should be instructed in adjusting their own insulin – checking with the practice weekly. • 2-4 unit adjustment every 3-4 days until target blood glucose is reached. Targets: Pre breakfast target <7.0mmol/L • 2 hour post meal target <10.0mmol/L • Pre-dinner target 6.0–7.0mmol/L Insulin Dosage Adjustments – Pre-mixed insulin Regime (on HealthPoint) Insulin Dosage Adjustments – Basal Bolus Regime (on HealthPoint) Blood Glucose Levels (mmols/litre) Less than 4 or hypo 4-8 8-15 15 or higher Reduce cloudy night time insulin by 2 units Good Control Increase cloudy night time insulin by 2 units Increase cloudy night time insulin by 4 units. Reduce breakfast insulin by 2 units Good Control Increase breakfast insulin by 2 units Increase breakfast insulin by 4 units Before evening meal Reduce lunch insulin by 2 units Good Control Increase Lunch insulin by 2 units Increase lunch insulin by 4 units Before bed Reduce evening insulin by 2 units Good Control Increase evening insulin by 2 units Increase evening insulin by 4 units Blood testing times Before breakfast Before lunch Increasing Insulin Doses: Isophane nocte • Pre breakfast (fasting) BG – Usually >8 mmol/L and never less than 4: • Increase dose by 4–6 units – Usually 6–8 mmol/L and never less than 4: • Increase dose by 2–4 units • Once receiving >20 units daily + 3 consecutive pre breakfast (fasting) BG results higher than agreed BG target AND BG never less than 4 mmol/L – Insulin dose can be increased by 10–20% of total daily dose Twice daily Isophane (= Glargine) • Pre evening meal BG – Usually >8 mmol/L and never less than 4 • Increase pre breakfast insulin dose by 4–5 units • Usually 7–8 mmol/L and never less than 4 – Increase pre breakfast insulin dose by 2–4 units • Once receiving >20 units daily – 3 consecutive BG results (either pre breakfast or pre evening meal) higher than agreed BG target AND BG never less than 4 mmol/L – Appropriate insulin dose can be increased by 10– 20% of total daily dose Post-prandial testing • Check 2 hours after meal: target BG < 10 – If on OHA, maximise – If still not meeting target, make sure basal insulin dose is correct (pre-meal BG < 7) • If basal insulin correct then need to add rapid acting insulin or • Change to Premixed insulin regime Not testing (or not very much)! • Difficult to manage accurately – Most patients will check fasting BG • At least can adjust basal insulin (unless pt eats overnight) – Alternate times of testing so once or twice daily test can give maximum information; certain days of the week • Sometimes pre-prandial, sometimes post-prandial – Evening meal usually largest so 2 hours after dinner • Regular HbA1c (2-3 monthly) HbA1c remains suboptimal • Is basal insulin enough? – Is the dose correct: fasting BG < 7 – Some obese patients require large doses of insulin • Basal insulin 0.5 units/kg body weight/day • What about post-prandial hyperglycaemia? – It always comes back to the food! – If basal dose correct and on maximum OHA • Change to Pre-mixed insulin / basal bolus Changing Insulin Regimens • Options if HbA1c suboptimal on basal insulin: – If not on sulphonylurea: add it on and maximise – If on once daily Isophane, change to bd or Glargine – If on maximum orals: change to Pre-mixed bd insulin • Stop sulphonylurea, give same insulin dose as basal – Isophane 24 units bd: Penmix 30 24 units bd – Or, continue with basal insulin, stop sulphonylurea and add rapid acting insulin • Usually need same total daily dose as basal insulin • Glargine 30 units daily: Novorapid 10 units tds When to refer to Secondary services • This will depend on your teams’ experience: – Current situation (from my viewpoint): • Some practices independently start patients on insulin – Refer when issues with hypoglycaemia impact on improved control. – Or not achieving any improvement in HbA1c » Sometimes patients will self-refer • Other practices refer everyone who is on OHAs with suboptimal HbA1c – Appropriate if skill base and time not there Secondary Services • Expectation for the future (from Ministry of Health): – Insulin for type 2 diabetes patients will be initiated by all GPs • Mostly basal insulin + OHA, or pre-mixed insulin bd – May mean more patients are started on insulin early (appropriately) – Remember basal insulin only will not be sufficient for a number of patients and long-term adjustment is required • We are interested to see young type 2 pts < 25 yrs to provide intensive input Summary • Checklist for commencement of insulin – Maximised lifestyle changes, OHA – Patient willing; skill base in practice • Decision on insulin regime depends on – – – – BG profile ideally HbA1c Patient preference Familiarity of your team with regimen and follow-up required