301.
advertisement

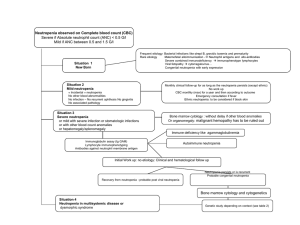
Lab Tests—what to do with a patient with neutropenia, thrombocytopenia, and/or erythropenia Barb Bancroft RN, MSN, PNPenia Oh, GROW UP!! • The process of maturation and differentiation • Everything starts with a pleuripotential stem cell—to 2 cell lines 1) Myeloid stem cells—erythrocytes (RBCs), eosinophils*, neutrophils*, basophils*, monocyte/macrophages, megakaryocytes/thrombocytes/platelets *collectively called the “granulocytes” because they have granules in their cytoplasm—for staining purposes (red/eosin/acid; white/neutral; blue/basic 1) Lymphoid stem cell—T lymphocytes, NK cells, plasma cells/B lymphocytes Some normal numbers Platelets (thrombocytes)—150,000-450,000— less than 100,000 is considered thrombocytopenia Erythrocytes (RBCs)--4.5 million to 6 million • Gender differences • Women with less blood volume and more fat tissue than men with more muscle mass • Women closer to the 4.5 million; men up around the 6 million Some normal numbers… • Neutrophils /segs (57-63%) of the total white count; acute inflammation, bacteria, acute necrosis (1.51-7.07) • NOTE: the precursor to the neutrophil is the band neutrophil; Bands (0-4%) (0.00-.51)—it’s almost mature and can perform many of the functions of the mature neutrophil ; In fact, when a band is released from the bone marrow it only takes 2 hours to mature into a neutrophil • Eosinophils? 3% of total WBC • Basophils? <1% of total WBC Cell growth—Too much? Too little? • Too much? Thrombocytosis • Too little? Thrombocytopenia • Too much? Neutrophillia, eosinophillia, basophillia (CML, PV) • Too little? Life-threatening neutropenia (There is no such thing as life-threatening eosinopenia or basopenia) • • • • OUR FOCUS TODAY? What happens when you don’t have enough? Too little? Thrombocytopenia Too little? Life-threatening neutropenia Too little? Erythropenia? Anemia First question in the work-up of a patient with a “penia”… • Is this an isolated “penia”? • Normal platelets, RBCs, but just neutropenia? • Thrombocytopenia, but with normal # of platelets, and normal # of neutrophils? • OR more importantly, is this pancytopenia? EVERYTHING is “penic”—more ominous but even isolated “penias” require diagnostic acumen The neutrophil • Neutrophils—(phagocytic)—only job in the world is to EAT until it dies • Cell of acute inflammation • First responder to bacterial invasion • Loves acute necrotic tissue Drugs and neutropenia • • • • • • • • Chemotherapy (all patients) Cimetidine (Tagamet), ranitidine (Zantac) Captopril (Capoten), enalapril (Vasotec), amiodarone, quinidine Zidovudine (Retrovir), vidarabine (Vira-A), Flucytosine (Ancoban) ASA, acetaminophen Anti-convulsants-- Carbamazepine (Tegretol); Phenytoin (Dilantin) Antibiotics including metronidazole (Flagyl),gentamicin, clindamycin, vancomycin, imipenem, PCNs, tetracyclines, TMP-SMX • Azothiaprine (Imuran) • PTU and methimazole Other causes of neutropenia • Bone marrow replacement—tumor infiltration, leukemia, myelofibrosis • Immunologic—autoimmune (antineutrophil antibodies—SLE, newborns from maternal IgG) • Metabolic—hyperglycemia (other rare causes of metabolic disorders) • Nutritional—anorexia nervosa, B12/folate deficiency, copper deficiency • Sequestration—hypersplenism Transient neutropenia • The most common cause is viral infection— influenza, adenovirus, coxsackie virus, RSV, hepatitis A and B, measles, rubella, EBV, CMV, and varicella. • The neutropenia usually develops in the first 2 days of the illness and may persist for up to one week • Redistribution of neutrophils (margination pool), sequestration in lymph nodes and BM, marrow suppression) • low risk for serious infectious complications The neutrophil in the world of ONCOLOGY • Fastest dividing cell in the body as an adult • Chemotherapy and radiation therapy kill cells that are rapidly dividing causing life-threatening neutropenia • ANC—absolute neutrophil count • Neutrophils (60%) + bands (4%) = ANC = 64% of the total WBC • If the total WBC is 10,000/ml³, the ANC is 64% or 6,400 The Absolute Neutrophil Count (ANC) • Neutropenia is defined as an absolute neutrophil count (ANC) <500/mm3 or an ANC of <1,000/mm3 with an expected decline. • Serious bacterial infection risk increases directly with the following: (1) severity of neutropenia (ANC < 100 cells/mm3 imposes a greater risk than ANC < 500 cells/mm3), (2) rate of ANC decline (rapidly falling rate imposes a greater risk than chronic neutropenia or aplastic anemia), and (3) duration of neutropenia The Absolute Neutrophil Count • When the ANC falls below 500, control of endogenous microbial flora (mouth, gut) is impaired • When the ANC falls below 200, the inflammatory process is absent. The oncology patient with neutropenia • Patient with a total WBC of 2,000/ml³ is LEUKOPENIC. But, is she NEUTROPENIC? Her neutrophils are 30%, bands are 2%; what’s 32% of 2,000? 640/ml³ • Patient with a total WBC of 2,000/ml³ is LEUKOPENIC. But, is she NEUTROPENIC? Her neutrophils are 50%, bands are 4%; what’s 54% of 2,000? 1080/ml³ • [Neupogen (1991) (filgrastim) and Neulasta (2002)(pegfilgrastim) Febrile neutropenia • The most serious immediate consequence of chemotherapy is febrile neutropenia—defined as an absolute neutrophil count of less than 500 cells per cubic millimeter and a temperature of more than 38.5° C. • Most standard dose chemotherapy regimens are associated with 6 to 8 days of neutropenia • Neutropenia blunts the inflammatory response to infections, allowing bacterial multiplication and invasion • Predisposes patients to serious infections and death if severe neutropenia persists for longer than 10-14 days • (N Engl J Med 2013 Mar 21;368:12) Neutropenia • Acute neutropenia, such as that caused by cancer chemotherapy, is more likely to be associated with increased risk of infection than neutropenia of long duration (months to years) • Rare—usually may manifest in early childhood as a profound constant neutropenia or agranulocytosis Approach to the patient with thrombocytopenia • Is this a healthy young adult with thrombocytopenia or an elderly hospitalized ill patient receiving multiple medications? • Limited differential in the young patient Approach to the patient with thrombocytopenia • Myelodysplasia can present in patients presenting with isolated thrombocytopenia who are greater than 60 years of age • FH (inherited thrombocytopenia is rare) • PE: spleen (mild to moderate splenomegaly is easier to pick up with abdominal ultrasound); enlarged liver, extremities (a platelet count of 5,000 to 10,000 is required to maintain vascular integrity in the microcirculation. With markedly decreased platelets, petechiae first appear in areas of increased venous pressure, the ankles and feet in an ambulatory patient Clinical signs of thrombocytopenia • Petechiae are pinpoint, non-blanching hemorrhages and are usually a sign of decreased platelet number and not platelet dysfunction • Wet purpura, blood blisters that form on the oral mucosa, are thought to denote an increased risk of life-threatening hemorrhage in the thrombocytopenic patient • Excessive bruising is seen in disorders of both platelet number and function Manifestations of platelet deficiency or platelet dysfunction • Superficial bleeding is the rule with platelet dysfunction or deficiency • Mucous membrane bleeding—easy bruising, nose bleeds (most common cause?), gum bleeds, blood in the urine (hematuria), blood in the stool (occult blood) – Causes of thrombocytopenia • Decreased production—bone marrow depression, marrow infiltration, congenital • Excessive pooling—hypersplenism • Infection: HIV, EBV, HCV • Coagulopathies—HELLP syndrome, DIC (meningococcal septicemia) • Increased destruction—Immunologic destruction with autoimmune disease, Henoch-Schonlein purpura, thrombotic thrombocytopenic purpura (TTP); severe hemorrhage, Immune thrombocytopenia (ITP) • Acquired disorder leading to immune-mediated destruction of platelets and possibly inhibition of platelet release from the megakaryocyte • Kids? Usually an acute disease following a viral infection • Adults? More chronic and usually secondary – associated with an underlying disorder • Autoimmune, especially lupus (SLE) • Infections: HIV, HCV, EBV, Helicobacter pylori Lab tests • Test for HIV, hepatitis C, EBV and other infections depending on the patient, of course • Coomb’s test if anemia is present (to rule out combined autoimmune hemolytic anemia) • Is this a 27-year-old female with anemia and thrombocytopenia? • Is this a 27-year-old male with anemia and thrombocytopenia? Drugs definitely reported to cause isolated thrombocytopenia • • • • • • • • • • • • Abciximab (Reopro) Acetaminophen Acyclovir Aminosalicylic acid Amiodarone Amphotericin B Ampicillin Carbamazepine Chlorpropamide Danazol Diclofenac Digoxin • • • • • • • • • • • • Eptifibatide HCTZ Ibuprofen Levamisole Octreotoide Phenytoin Quinine Rifampin Tamoxifen Tirofiban TMP/SMX vancomycin Other drugs that decrease platelets or cause platelet dysfunction • Prescription drugs and platelets: SSRIs (fluoxetine/Prozac; paroxetine/Paxil/Pexeva; sertraline/Zoloft; citalopram/Celexa; escitalopram/Lexapro)—increased risk of bleeding • Valproic acid – keep eye on platelet counts— more problems… Heparin-induced thrombocytopenia • Thrombocytopenia due to heparin differs from that seen with other drugs in two major ways 1) The thrombocytopenia is not usually severe (not less than 20,000) 2) HIT is not associated with bleeding and, in fact, markedly increases the risk of thrombosis due to antibody formation to a complex that activates platelets Causes of platelet bleeding • Don’t forget ETOH abuse also causes thrombocytopenia Causes of platelet dysfunction • Ask about OTC and complementary and alternative therapies; over-the-counter such as NSAIDS (24 hours for ibuprofen)*, ASA (7 days); *Don’t have to stop Celebrex before surgery • the G’s—gingko, ginseng, glucosamine, garlic, ginger; omega-3s, vitamin E Platelets • Just a reminder…some patients can have plenty of platelets but the platelets don’t work • Qualitative Platelet dysfunction • How well do they “plug a hole”? OLD: Measure the bleeding time (3-6 minutes) • NEW: PFA – Platelet Function Assay One last point about platelets… • Can you hemorrhage with low platelets?…yes • The rate of the fall is more important than the total number of platelets in most instances • However, very low platelets, less than 10,000 increase the risk of hemorrhage no matter how fast the platelets fell Erythropenia () and anemias • • • • What do you need to make happy, healthy RBCs? Good parents (good genes)--hemoglobinopathies Healthy thyroid (metabolism and production of RBCs) Healthy kidney (the hormone erythropoietin to stimulate the production of RBCs in response to hypoxia) • Iron (dietary deficiency in growing kids and pregnant moms; celiac disease—poor absorption in distal duodenum; —the major source of iron in adults is recycled RBC—not dietary; hence—loss of blood increases risk) • B12 –animal protein, stomach IF, ileum for absorption, vegetarians, drugs such as metformin, PPIs, Crohn’s, aging • Folic acid (B9)—fruits and veggies So what can go wrong? • • • • • • Lousy genes Hypothyroidism Renal failure Iron deficiency B12 deficiency Folic acid deficiency Anemia • The skin and mucous membranes may be pale if the hemoglobin is less than 80 – 100 g/L (8-10 g/dL) • Focus on the areas where vessels are close to the surface such as the mucous membranes, nail beds, and palmar creases • If the palmar creases are lighter in color than the surrounding skin when the hand is hyperextended, the hemoglobin level is usually less than 80 g/L (8 g/dL) Get the most bang for your buck with 3 tests • Hemoglobin • MCV (mean cell volume)—what is the SIZE of the RBC? Are they too small? microcytic anemia; are they too big? Macrocytic anemia; are they normal size but just too few of them? Normocytic anemia • Reticulocyte count—is this patient “reticking”—is the bone marrow producing RBCs? 0.5-2% of total RBC count; takes 7-12 days to make and release a “retic” from the bone marrow Some other numbers… • • • • • Hemoglobin adult females (12-16 g/dl) (120-160 g/L) males (14-18)(140-180g/L What is anemia defined as? Hemoglobin under 12 g/dl (120 g/LL) for females and under 14 g/dL (130 g/L for males) 3 tests for anemia that are most important • MCV (mean cell volume)—what is the SIZE of the red blood cell? Too small (microcytic)? 9 out of 10 cases are caused by iron deficiency anemia; to BIG (macrocytic)? 7 out of 10 are due to either a B12 deficiency or a folic acid deficiency; normal size (normocytic)? Check the thyroid and the kidneys! Microcytic anemia • MCV 65 (normal 83-97 fl) • 9/10 with iron deficiency anemia • Adults Where’s the bleed? Female? Male? Exercise? NSAIDS? • Are you pregnant? • Growing kid? Lousy diet • Not growing? Celiac disease from malabsorption of iron in the duodenum • Tea drinking? • Two other causes of microcytic anemia—lead poisoning, Thalassemia Iron and RBCs • How do we get iron? • Food—especially as children for vertical growth • Food—not so much in adults as we are not growing vertically and we usually get plenty of iron from our diet (only need 1 mg from diet of the 20 mg used per day—the other 19 mg is recycled through the senescence of old RBCs) • Pregnancy -- need extra iron to grow a baby How do we become deficient in iron? • Bleeding—anywhere; women have 20% less blood than men, hence, lower iron stores and a greater risk of iron deficiency anemia; also have periods premenopausally which increases risk of iron deficiency due to RBC depletion (and depends on type of period) • Bleeding—ALWAYS THINK GI, GI, GI Macrocytic anemia • MCV greater than 100 fL • MCV between 100 and 120—think booze • MCV greater than 120—think B12 or Folic acid deficiency (also known as megaloblastic anemia) Drugs that cause megaloblastic anemia • • • • • • • Acyclovir (anti-herpes drug) ASA Anticonvulsants Azathioprine (Imuran) Colchicine (gout) INH (TB) Metformin (Glucophage, Glumetza, Fortamet)—type 2 diabetes, PCOS) • MTX (methotrexate) • Proton Pump inhibitors (more in a minute) B12 … a few more notes • Normal B12 range is 200-800 pg/mL • 2,000 to 5,000 mcg of B12 is stored in the liver for 5-7 years; • Use about 2.4 mcg per day for making RBCs, keeping the myelin in our central and peripheral nervous system healthy, and making serotonin in our “happy” centers • Takes 5-7 years of no B12 intake to deplete Clinical conditions associated with B12 deficiency • Big, immature RBCs—called megaloblastic anemia (MCV is greater than 100 fl) • Cognitive dysfunction—#1 cause of nutritional dementia • Peripheral neuropathy (one of three top causes in elderly) • Depression (B12 is a co-factor in the production of serotonin) • So you have NO energy, you’re demented, can’t feel your feet and depressed…JEEZZZZ…how important is B12? High-risk patients for B12 deficiency • Over 55 • Lack of intrinsic factor (IF); autoimmune gastritis; gastrectomy patients • No animal protein in the diet; vegetarians; Tea and Toasters; alcoholics • Liver failure • Malabsorption—Crohn’s disease, celiac disease; gastric by-pass surgery • Metformin (glucophage) • Proton Pump Inhibitors—inhibit the pump that pumps HCL acid AND Intrinsic factor; Intrinsic factor binds B12 and moves it to the ileum for absorption • (Am J Clini Nutr (2007);86:1384) B12 supplements? • The 4 S’s • • • • Swallow it Suck it Snort it Shoot it… • Don’t overdose… You need Folic acid (B9) to make happy, healthy RBCs • Dr. George Herbert • 40 days and 40 nights to deplete bone marrow stores • Maintenance of healthy RBCs--anemia • Maturation of the neural tube (first 28 days)-NTDs • Take folic acid 400 mcg (0.4 mg) BEFORE you get pregnant + eat • Green leafys and citrus fruits Drugs that block folic acid synthesis that are taken longer than 40 days and 40 nights… • • • • TMP/SFX (Bactrim, Septra) Rheumatrex (Methotrexate) Phenytoin (Dilantin) Oral contraceptives • Supplement with folic acid Normocytic anemia • RBCs 3,000,000 • MCV normal • The anemia of chronic disease—CKD, hypothyroidism, chronic inflammation), cancer (unless a bleed is involved) 3 tests for anemia that are most important • Reticulocyte count—how well is the bone marrow making RBCs? • Is this patient “reticking”? • Is the retic count HIGH? Hemolytic anemia • FYI: Corrected retic count for patients with anemia (NEXT time)—there is a formula • High retic count means that the bone marrow is making RBCs, but something is destroying them rapidly—either in peripheral blood or bone marrow (hemolytic) • Consider drug-induced hemolytic anemia • Drugs? Penicillin, cephalosporin, procainamide, quinidine, quinine, sulfonamide—drug-induced hemolytic anemias Diseases with hemolytic anemias and high retic counts • • • • • Sickle cell? Genetic hemoglobinopathy Thalassemia? (as above) G6PD deficiency?(as above) Autoimmune hemolytic anemia (lupus, drugs) Hemolytic uremic syndrome (drugs, Shiga toxin producing E.coli) Coomb’s test • Coomb’s test—what is it used for? If +, it means an autoimmune process with antibodies against RBCs (drugs, lupus) Thank you… • Barb Bancroft, RN, MSN, PNP • Chicago, IL • www.barbbancroft.com Selected Bibliography • Bakerman’s ABC of Interpretive Laboratory Data 3rd Printing • Harrison’s Hematology and Oncology. 2010. McGraw Hill. • Kee JL. Laboratory and Diagnostic Tests. 2014. Pearson. • Lam JR, et al. Proton pump inhibitors and H2 receptor antagonist use and vitamin B12 deficiency. JAMA 2013:310(22):2435-2442 Bibliography • DeJager J, Kooy A, Lehert P, et al. Long-term treatment with metformin in patients with type2 diabetes mellitus and risk of vitamin B12 deficiency: randomized placebo controlled trial. BMJ 2010;340:c2181). Sando KR, Barbora J, Willis C et al. Recent diabetes issues affecting the primary care clinician. Southern Med J 2011;104(6):456-61)