Right or Commodity?
advertisement

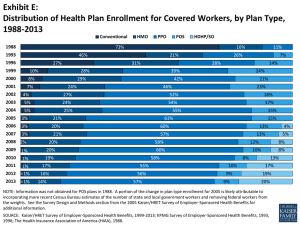
Health Care: Right or Commodity? The Affordable Care Act and the Marketization of Health Care Adam Gaffney, MD Physicians for a National Health Program NY-Metro Forum: October 14, 2014 Primary Arguments • A right to health care – Not simply a question of “universal access to health insurance.” – Financial barriers to access and health care inequality not consistent with a “right” to health care. • The ACA does not create a right to health care – Uninsurance persists – Underinsurance or “malinsurance” persists – Health care inequality persists • Health care “rights” vs. “commodity” dialectic matters Two Different Conceptions: Right or Consumer Commodity • Health care “right/commodity” dialectic stretches back into history. – Writing ~ 17C, Chinese ethicist Chu Hui-ming wrote: “In antiquity it was said: There are no two kinds of drugs for the lofty and the common; the poor and the rich receive the same medicine.” – Kung Hsin, Confucian physician: For an “enlightened physician,” a “patient’s wealth or poverty is of no concern … they prescribe drugs according to a formula which is valid for everyone.” Unschuld, Paul U. Medical Ethics in Imperial China. Berkeley: University of California Press, 1979, page 63 and 69. Health Care as a Right • The “Right to Health” – FDR: 1944 SOTU Address: “The right to adequate medical care.” – Universal Declaration of Human Rights: Included many social/economic rights including right to medical care – WHO Constitution: “…the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being…” • Postwar Period – National Health Service in Britain – Movements towards universal health care in many nations http://museum.hackney.gov.uk/object9232 Truman’s NHI • Truman: NHI “will mean that proper medical care will be economically accessible to every one covered by it, in the country as well as in the city, as a right and not as a medical dole.”1 • “I consider it socialism. It is to my mind the most socialistic measure that this Congress has ever had before it” 2 –Senator Robert Taft 1 Quoted in Beatrix Hoffman. Health Care for Some, 59. 2 Quoted in Monte Poen, Truman Versus the Medical Lobby, 88. “The major issue has been decided. Do individuals have a right to medical care by virtue of their being a citizen of the United States, a human being? I think that answer has been given”1 -Wilbur Cohen. Images from http://www.ssa.gov/history/lbjsm.html 1 Wilbur Cohen, Toward new human rights, 1977. New York Times, August 9, 1971; quoted in Hoffman, 163. Health Care as a Right … • The Kennedy-Griffiths 1970 Health Security Bill S.4323 – A single national health insurance w/o means testing (no significant role for private insurers) – No cost sharing: Elimination of all co-payments • 1971: Nixon’s Response to the Kennedy-Griffiths Bill – Means testing: Expanded Medicaid-like program for the poor (up to 122% of poverty) – Employer mandate – Maintained private insurance – Cost-sharing: Deductibles, Copayments Paul Starr, Remedy and Reaction, 53-54 Beatrix Hoffman, Health Care for Some, 164 The Neoliberal Health Care Turn 1) Health care is ultimately a commodity or consumer good 2) Individuals differ in the amount of health care goods they desire (in relation to other goods). 3) There is no “universal” standard of health care for all. 4) “Free” care the problem: Patient’s should use their “own money” to avoid moral hazard 5) “For-profit” medicine key • asdf “Medical care is neither a right nor a privilege: it is a service that is provided by doctors and others to people who wish to purchase it … whether to buy a doctor’s service rather than some other commodity or service belongs to the consumer as a logical consequence of the right to his own life.” The Rise of Corporate Medicine • Corporatization of the HMO – Consolidation/Mergers – For-profit HMOs: 18% in 1981 > 60% by 19861 2 1 Gray, Bradford H. 2006, page 315. 2 http://www.modernhealthcare.com/article/20120303/MAGAZINE/303039958 National Hospice and Palliative Care Organization. "Nhpco's Facts and Figures." (2013). “Consumer-Driven Health Care” • 1970s: Health care “consumerism” – empowering patients; having say in treatment decisions; opposing medical paternalism; community involvement in healthcare.1 – 1971 Editorial in Archives of Internal Medicine: examples include free clinics, the community takeover of Lincoln Hospital2 • 2000s: “Consumer-Directed Health Care” care plans = HDHPs + HAS – 2003 Medicare Modernization Act creates the current CDHP 1 Tomes 2006, “Patients or Health-Care Consumers?” 2 Bogdonoff 1971. “Consumerism in medicine.” Arch Intern Med 128(3):469-71. Neoliberal Ideology: Health Care as a Commodity • Friedrich Hayek – 1960: “The conception that there is an objectively determinable standard of medical services which can and ought to be provided for all … has no relation to reality.” • Milton Friedman – 1991: “End both Medicare and Medicaid and replace them with a requirement that every U.S. family unit have a major medical insurance policy with a high deductible …”1 – 2001: “The patient, the recipient of the medical care, has little or no incentive to be concerned about the cost – since it’s somebody else’s money.”2 1 Hayek , The Constitution of Liberty. New York: Routledge, 2011. 1 Milton Friedman, “Gammon's Law Points to Health-Care Solution, Wall Street Journal, November 12, 1991: 1. 2 ---, “How to Cure Health Care,” The Public Interest Winter, 2001 The Affordable Care Act • Expands access while assuming many of the tenets of health care neoliberalism • Nixon plan elements – A [limited] employer mandate – Expanded means-tested program for the poor (Medicaid, up to 138% FPL) • Individual mandate – A requirement of the health insurance industry • Accommodates – Skin in the game: trend towards higher cost-sharing: copayments, deductibles, co-insurance – Corporatization of medicine • Does the ACA create a right to Health Care? – “Two kinds of medicine for the rich and poor?” or – Class-based medicine I. Employer-Based Insurance -Study of employer-based health insurance -62% increase in premiums -Rising cost sharing 26.7% Worker contribution 28.6% Worker Contribution Cost Sharing: Definitions • Copayments • Fixed amount for a health care service • Deductible • Amount paid for health care services before health insurance contributes • Coinsurance • Percent of cost of health care service paid by the insured after the deductible is met – Out-of-pocket maximum • After premium, most the insured is liable for • In-network/covered services KFF/HRET Survey of Employer-Health Insurance -From 2006 to 2014, the percentage of covered workers with a general annual deductible increased from 55% to 80%. -Percentage of workers in a Consumer-Directed Health Plan (High-Deductible Health Plan + HSA) 2006: 4% 2014: 20% Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2006-2014 Covered Workers with a General Annual Health Plan Deductible for Single Coverage $1,400 $1,200 $1,000 $800 $600 $400 $200 $0 2006 2007 2008 2009 2010 2011 2012 Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2006-2014 2013 2014 Separate from the general annual deductible…. • Separate cost sharing for hospital admission – – – – – Separate annual deductible: 3% [average $490] Copayment: 15% [average $280] Coinsurance: 62% [average 19% of bill] Both copayment and coinsurance: 10% Charge per day: 5% [average $297] • Separate cost sharing for outpatient surgery – Copayments: 16% [Average copayment: $157] – Coinsurance: 64% [Average: 19% of bill] – Both Copayment and Coinsurance: 7% Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2014 Copayments • Physicians Visits – Copay • Percent of plans: 89% Primary Care, 72% Specialists • Average Copay: $24/$36 • Average Coinsurance: 18%/19% • Drugs – Three, four, and five tiers of copayments AND coinsurance. – Very high for so-called “specialty” drugs Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2014 https://www.bcbsnc.com/content/services/formulary/rxdef.htm http://www.bcbsm.com/index/health-insurance-help/faqs/plantypes/pharmacy/what-are-specialty-drugs.html “With the new pricing system, insurers abandoned the traditional arrangement that has patients pay a fixed amount, like $10, $20 or $30 for a prescription, no matter what the drug’s actual cost. Instead, they are charging patients a percentage of the cost of certain high-priced drugs, usually 20 to 33 percent, which can amount to thousands of dollars a month” -Generics reported to rise in price > 600 – 1000% By Caroline Mayer July 1, 2013 “Even with Stage IV lung cancer, there are moments when 32-year-old Chip Kennett feels blessed. Over the course of two weeks in April, those moments were many, as 325 friends and family members contributed $56,800 over the Internet to help defray his out-of-pocket medical costs … The Kennetts acknowledge they are lucky to have good health insurance …. Even so, the Kennetts have paid thousands of dollars in out-of-pocket expenses, including the insurance plan’s co-pay requirements and its $5,000 annual deductible ($7,000 for out-of-network doctors) for both 2012 and 2013. They also face large bills for their share of medication costs, including $485 a month for a blood-thinning injection … and $480 a month for a bone-strengthening injection.” • More companies offering HDHPs as only option (GE, JP Morgan, Honeywell) • ~50% increase in number of employers that plan to offer HDHP as the only plan option in 2015 (10% in 2010; 22% in 2014; ? 32% in 2015) -Analysis of ED visits and hospitalizations over two years among enrollees inured in high deductible plans in Massachusetts -Resulted in 25-30% reduction in “high-severity ED visits”(defined as a diagnosis with 75%+ likelihood of requiring emergency department care) over both years, with a reduction in hospitalization by 23% in year 1 but a rise in year 2. II. The Obamacare Exchanges: Individual Health Insurance • Actuarial Value: 60% for the “Bronze Plans”, 70% in the “Silver Plans,” 80% in the “Gold Plans,” 90% in Platinum. – Copays – Deductibles – Coinsurance NY State of Health – Standard Bronze Plan (Family) • $6,000 deductible • Out-of-pocket maximum: $12,700 for a family with incomebased adjustments … • 50% coinsurance after deductible for: – – – – – – – – “Ambulance services” Emergency department (unless admitted) Urgent Care Center “Advanced imaging” “Diagnostic tests” Dialysis Hospice care Inpatient care for end of life care (preauthorization required) Source: NY State of Health Standard Products; courtesy of Len Rodberg Different medicine for the “common and the lofty”? http://www.whatmattersbywellmark.com/premiums.php Out-of-Pocket, Out-of-Money? KFF 2012 CWF, 2014 Out-of-pocket limits: A Changing Target BOTTOM LINE: For a family of 4 making with income of $60,000, out-ofpocket liability doubled, from ~$6,000 to ~$12,000. http://www.salon.com/2014/04/11/a_pro_single_pay er_doctors_concerns_about_obamacare/ Out-of-Pocket Maximums: A Changing Target • How/Why? ACA specifies that if the original limits would increase the actuarial value of the plans above what is required by law (i.e. would result in insurance companies paying for > 70% of your health care bill for a silver plan), government would increase out-ofpocket maximum. • asdf -Favored by insurance industry, some Democrats -”Copper Plans” would have actuarial value of ~50% -Presumably OOP limits would have to be increased -Next up? III. “Private Option” Medicaid • 2010: Supreme Court makes the ACA’s expansion of Medicaid optional for states. • States now have leverage to obtain “waivers” to experiment with Medicaid expansion – in a conservative direction. • Arkansas, Iowa: Obtained waivers to expand Medicaid through the “Private Option” (voucher to buy plan on the exchange). Pennsylvania has followed. The “Private Option” • Arkansas: Medicaid legislation required establishment of “independence accounts that operate similar to a Health Savings Account” and that would allow participants to “purchase cost-effective high-deductible health insurance” that would “promote independence and self-sufficiency.” "We believe in consumerism," according to the director of the Arkansas Department of Human Services. By making the poor act more like consumers, "we think they'll use care more appropriately and get a sense of how insurance works." Waiver: Gives enrollees the “private health insurance experience” and “promotes consumerism” & “preserve[s] dignity.” Also “the infusion of market principles works to educate members and prepare them to participate in the private market.” Does It Have to Be This Way? Out-of-Pocket Health Care Spending per Capita, 2007 Adjusted for Differences in Cost of Living Dollars 890 800 720 580 600 573 542 528 485 470 351 400 343 246 213 200 0 US NOR CAN AUS* * 2006 Source: OECD Health Data 2009 (June 2009). ITA SWE OECD Median GER NZ UK Courtesy Len Rodberg FR NETH Cost Sharing = Cost Saving? Source: Patryk Perkowski and Leonard Rodberg, unpublished data 2014. Courtesy of Leonard Rodberg. http://www.nytimes.com/2014/09/27/upshot/the-benefits-of-economic-expansions-areincreasingly-going-to-the-richest-americans.html?abt=0002&abg=0 A right to health: No two types of medicine for the lofty and the needy ... • Cost sharing in an era of rising inequality inevitably contributes to class-based medicine regardless of the intent of the provider. • A right to health care is much more than “universal access” to insurance. It requires: – Equality of access – No financial barriers to care • True universalism does not square with for-profit system: no need for product design with “everyone in and nobody out.” • The fight for single-payer – About more than universal access, administrative savings – About health care equality – Part of a larger campaign against rising inequality