PCP, continuity NP, RN, MA, Clerk, Behaviorist Primary Care Team
advertisement

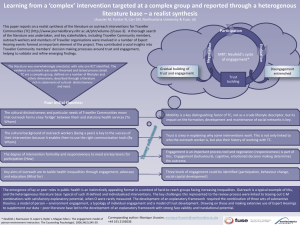
Building Blocks of High-Performing Primary Care The Share-the-CareTM Model 10 Template of the future 1 Engaged leadership 8 9 Prompt access to care Coordination of care 5 6 7 Patient-team partnership Population management Continuity of care 2 3 4 Team-based care Data-driven Empanelment improvement SF Partnership for Population-focused care SFCCC, CEPC, SFDPH, SFHP Level 3: 5% Complex healthcare needs Complex Care Management Team: RN, SW, Health Coach Level 2: 80% Multiple chronic conditions: diabetes, HTN, COPD Primary Care Team: PCP, continuity NP, RN, MA, Clerk, Behaviorist Primary Care Team: Level 1: 15% Uncomplicated chronic disease or risk factors: obesity, prediabetes PCP, continuity NP, RN, MA, Clerk, Behaviorist GMC Care Management Team Roles Team member Roles RN Care Manager Medical Assistant Health Coach Provider (Resident, attending, or NP) Initial assessment and Care Plan Complex clinical issues and medication issues Clinical back-up for Health Coach Outreach to patients Coaching toward care plan goals Focus on self-management Primary point of contact for patients Refer patients Collaborate with CM team Titrate medications, plan diagnostic work ups Coordinator Manages referrals, data tracking, reporting Social Worker Referrals to entitlements and community-based programs Physician CM lead Program development and evaluation Clinical back-up to team Lead quality improvement Care Management Weekly Dashboard: Summary of Nov 26-30, 2012 avg/wk 4 wks ago 3 wks ago 2 wks ago last week Hospitalizations 2 0 2 0 2 New Hospitalizations Home Visits 1 1 0 0 0 2 Clinic Visits 4 6 1 5 1 Phone Calls 50 59 66 25 35 Home Visits Consults 15 61 34 20 21 0 Who's in the hospital this week? Year prior to During CM Percent What's coming up? Who are our new patients? Patient Name (11/25 - ) enrollment in reduction Phone Assessments Patient Name (11/28 -) CM Number of Days Hospitalized per month before and after Care Management Hospital days per year per 18 5 patient 9.37(n = 21) 5 mo prior 23 22 6 8 1 mo after 2 mo after 1 4 mo prior 3 mo prior 1.48 2 mo prior 1 mo prior 13 7 3 mo after 4 mo after 5 mo after 2 31% 6 mo after Total Care Management Patients Enrolled Total Care Management Patients Enrolled 1 7 Total 2 3 6 3 40 #REF! 6 Enrolled 4 10 5 IA 5 1 35 PRE 5 Pre 40 10 1.02 Utilization data for patients in CM for > 6 months (n=27) CRITICAL 3 TOTAL 39% 59 ED Visits per Level Breakdown year per patient 6 mo prior 5.75 5 4 1 Jan 1 2 8 Feb Mar 15 Apr #REF!8 7 4 2 30 33 35 35 Aug Sep Oct Nov 61 4 24 25 Jun Jul 4 19 May Enrolled Dec PRE Printed on: 1/11/2013 2012 Colorectal Cancer Outreach Project • Joint effort: SFDPH-PC, CEPC , SFHP • Training: colon CA, registry, outreach skills. Outreach Work - off site, early evening. Mass mail out, phone banks • CEPC: In Time training on registry use, scripts + role play talking to patients, coaching during phone banks • 10 clinics, 35 staff – 4900 postcards mailed (4 languages), 6 phone bank sessions: 2400 calls, 1200 FIT tests done in outreach group • Repeated in Sept 2012 • Screening rate 10 participating clinics up 19% over baseline from 02/2012 to 11/2012 (at 54% 11/2012) Slide Courtesy of Lisa Golden, M.D. Building Blocks of High-Performing Primary Care The Share-the-CareTM Model 10 Template of the future 1 Engaged leadership 8 9 Prompt access to care Coordination of care 5 6 7 Patient-team partnership Population management Continuity of care 2 3 4 Team-based care Data-driven Empanelment improvement