Outcome measurement – International perspective 7th February 2014 Variation in health outcomes is an international problem 2x variation in 30-­‐day mortality rate from heart attack in US variation in bypass surgery mortality in the UK variation in complication rates from radical prostatectomies in the Netherlands variation in reoperation rates after hip surgery in Germany variation in mortality after colon cancer surgery in Sweden variation in capsule complications after cataract surgery in Sweden Variations in health outcomes can be found in care teams, within institutions, nationally, internationally… 4x 9x 18x 20x 36x St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 1 “Magic bullets” we have tried to reduce variation Clinical pathways, standardized care protocols Evidence-­‐based medicine, guidelines Checklists Lean management Process measures EMR, computer-­‐aided decision support (…) St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 2 Physicians typically don’t believe in top down solutions Clinical pathways, care protocols Evidence-­‐based medicine, guidelines Checklists Lean management Process measures EMR, computer-­‐aided decision support (…) St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 3 Santeon – a group of top clinical hospitals that wants to explore pioneering solutions and to provide best care St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 4 Our core belief Physicians, nurses and therapists are intelligent, creative people who must acquire and synthesize knowledge and often adapt established guidelines to make the best treatment decision for an individual patient but (as every person who works in an environment of insecurity ) they need meaningful and timely feedback in order to learn and improve St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 5 Martini-Klinik
UKE GmbH Strukturierter Qualitätsbericht 2010
Martini Klinik fam
aculty Nine consultants, different specialization, equal voting rights St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. A-2 Institutionskennzeichen des Krankenhauses
6 urethral sphincter is essential to preserving
r RP. The pelvic floor is a complex system of
amic forces. The insertion of the urethral
this system is the prerequisite for its
ular function [7]. In this paper, we describe
or an individualised apical preparation to
l functional length of the urinary sphincter
ic integrity during RP.
(medial dorsal raphe), providing a point of fixation (Fig. 3) [6,13]. The
puboperinealis portion of the levator ani (puboperinealis muscle, levator
urethrae muscle) forms a hammock around the urethra and terminates
at the perineal body between the urethra and the anterior aspect of the
rectum (Fig. 3) [14]. Voluntary contraction of the puboperinealis and
rectourethralis muscle pulls the urethra forward and upward, resulting
Urethral sphincter muscle is partially covered by the prostate in closure and termination of the urinary stream [7]. Further lateral
support to the sphincter is provided by the Mueller’s ligaments
(ischioprostatic ligaments, Walsh’s pillars) [7,10,12,15,16] (Fig. 3), which
s and patients
[()TD$FIG]
utive patients who underwent RP between May 2008
e analysed. All surgical procedures were performed by
surgeons (T.S., H.H., M.G.). The prospective collection of
d by our internal reviewer board, and all patients
nformed consent. All surgical cases were performed
opubic approach described by the authors previously
effect of our surgical modifications on early and long-
n a statistically representative cohort, a consecutive
on–full functional-length urethra [non-FFLU; n = 285]
undergoing surgery by the three surgeons within 1 yr
tinence rates were assessed using a self-administrated
nd 12 mo after removal of the catheter. Continence was
of no pads and no leakage of urine. To assure the
of our surgical modifications, we performed intra-
rential frozen sections from the cranial and caudal
of the urethra during the development phase of the
cryosections showed tumour-free margins. Since July
ditionally inked the intraprostatic urethral resection
ess exactly the rate of positive surgical margins (PSMs)
by our modified technique.
considerations
by anatomic and functional studies, an important
the urethral sphincter is located intraprostatically
and the colliculus seminalis
The
Source: Eur[2,3,6,8,11,13].
Urol 60 (2011): 320-329
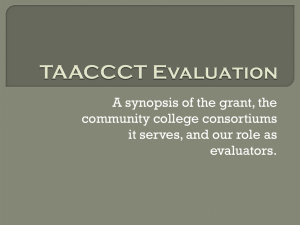
St. Antonius 2014 JDW.pptx Fig. 1 – Transversal section of the prostatic apex. A considerable part of
the urethral sphincter is located intraprostatically between the prostatic
apex and the colliculus seminalis.
SMS = smooth muscle sphincter; SS = striated sphincter
(rhabdosphincter); CS = colliculus seminalis; PA = prostatic apex.
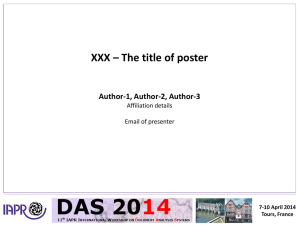
Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 7 Depending on localization up to 40% of sphincter muscle tissue are lost by removing the prostate 322
EUROPEAN UROLOGY 60 (2011) 320–329
[()TD$FIG]
Fig. 2 – Anatomic variability of the prostatic apex. Depending on the individual apex shape, between 10% and 40% of the functional urethra is covered by
parenchymal apex tissue. Otherwise, the prostatic apex is covered by some muscular tissue on the ventral and rectal aspects as rudiments of embryonic
and adolescent prostatic development.
Source: Eur Urol 60 (2011): 320-329
can easily be reconstructed by integration into the ventral anastomotic
sutures during RP to avoid deviations of the urethra.
St. Antonius 2014 JDW.pptx 2.3.
Surgical technique
puboperinealis portion of the levator ani to the urethra and the perineal
body is carefully preserved when it is gently pushed distally, enabling
Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 8 clear visualisation of the circumference of the urethra. During dissection
of the dorsal venous complex (DVC), a space between the DVC and the
fascia of the rhabdosphincter can be identified by blunt preparation with
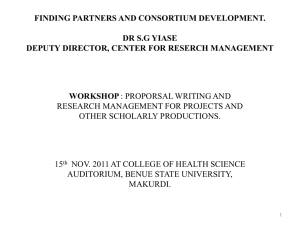
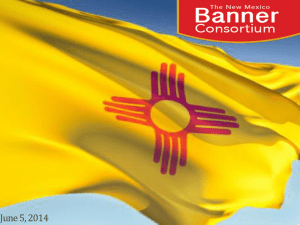
Example slide quality review IIEF-5-Score
3 Monatsbrief – Potenz
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
1-7 schwere ED
8-11 mittelschwere ED
12-16 mild-mittelschwere ED
17-21 milde ED
22-25 keine ED
Confidential ! Operateur
n
Graefen
c
o
Haese
n
Heinzer
fi
Huland
d
Michl
e
Salomon
n
Schlomm
t
Steuber
i
Budäus
a
Heuer
l gesamt
22
26
30
36
27
13
12
21
3
1
191
St. Antonius 2014 JDW.pptx 22-­‐25 keine ED (%)
6 (27.3)
2 (7.7)
0 (0.0)
4 (11.1)
1 (3.7)
0 (0.0)
0 (0.0)
1 (4.8)
0 (0.0)
0 (0.0)
14 (7.3)
17-­‐21 milde ED (%)
4 (18.2)
5 (19.2)
1 (3.3)
5 (13.9)
3 (11.1)
5 (38.5)
2 (16.7)
1 (4.8)
1 (33.3)
0 (0.0)
27 (14.1)
12-­‐16 8-­‐11 mild-­‐mittelschwere ED mittelschwere ED (%)
(%)
1 (4.5)
1 (4.5)
3 (11.5)
2 (7.7)
0 (0.0)
2 (6.7)
4 (11.1)
2 (5.6)
5 (18.5)
3 (11.1)
2 (15.4)
0 (0.0)
3 (25.0)
1 (8.3)
3 (14.3)
3 (14.3)
0 (0.0)
1 (33.3)
0 (0.0)
0 (0.0)
22 (11.5)
18 (9.4)
1-­‐7 schwere ED (%)
6 (27.3)
4 (15.4)
15 (50.0)
10 (27.8)
6 (22.2)
1 (7.7)
2 (16.7)
4 (19.0)
0 (0.0)
0 (0.0)
123 (64.4)
kein GV (%)
4 (18.2)
10 (38.5)
12 (40.0)
11 (30.6)
9 (33.3)
5 (38.5)
4 (33.3)
9 (42.9)
1 (33.3)
1 (100.0)
66 (34.6)
Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 9 FFLU = full functional-length urethra.
salvage or palliative setting (not included in the analyses),
406 patients with the FFLU technique, and 285 patients
with our conventional (non-FFLU) technique. There
were no significant differences in baseline and surgical
characteristics between the FFLU and non-FFLU groups
(Table 1).
The continence rates at 7 d and 12 mo after catheter
removal were 50.1% and 96.9% in the FFLU group and 30.1%
and 94.7% in the non-FFLU group, respectively ( p < 0.001,
p = 0.59; Fig. 10 and 11; Table 2). The reported number of
required pads correlated significantly with the reported
urinary leakage during coughing, laughing, sneezing, or
Comparison of outcome data in the quality review showed interesting variation [()TD$FIG]
Fig. 11 – Urinary control 1 wk after catheter removal.FFLU = full functional length urethra.
St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 10 After showing favorable results, FFLU was rapidly adopted 326
EUROPEAN UROLOGY 60 (2011) 320–329
[()TD$FIG]
Source: Eur Urol 60 (2011): 320-329
Fig. 10 – Impact of full functional-length urethra preparation on early urinary continence in a consecutive series of 691 radical prostatectomies. Average
numbers of pads used in a 24-h period per patient were calculated on a monthly basis and presented for each surgeon.
St. Antonius 2014 functional-length
JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. FFLU
= full
urethra.
11 physical activities (data not shown). The two groups had no
significant differences in the overall frequency of PSMs
One year after radical FFLU patient still (p =
0.39),
PSMs
in pT2prostatectomy, tumours ( p = 0.78),
and
PSMs in
the
showed improved continence rates separately
inked intraprostatic
urethral resection boarder
(Table 1).
Table 2 – Urinary control 12 months after radical prostatectomy
Pads/24 h
0
1–2
3–5
>5
FFLU (n = 324)
Non-FFLU (n = 282)
No. (%)
No. (%)
314
7
2
1
(96.9)
(2.2)
(0.6)
(0.3)
231
10
2
1
(94.7)
(4.1)
(0.8)
(0.4)
p
0.59
–
–
–
FFLU = full functional-length urethra.
use of a
catheter
Every
patients
consecu
the resu
the effec
question
removal
individu
function
after cat
remainin
techniqu
patients
with th
postoper
Source: Eur Urol 60 (2011): 320-329
St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 12 Patient-­‐reported outcomes one year after prostatectomy -­‐ Martini Klinik and average German Hospitals Martini Klinik 93,5 % Average German Hospitals 75,5 % Average German Hospitals 56,7 % Martini Klinik 34,7 % Average German Martini Hospitals Klinik 4,5 % 0,4 % 1 yr full con+nence 1yr severe erec+le dysfunc+on 1yr severe urinary incon+nence Source: Martini Klinik, BARMER GEK Report Krankenhaus 2012, Patient-­‐reported outcomes (EORTC-­‐PSM), 1 year after treatment, 2010 St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 13 Rapid growth after launch of Martini Klinik in 2005 2,225 1,973 +18,5% CAGR.
Prostatectomies/year, # 1,755
1,541
Martini Klinik
Hamburg University Medical Center, Urology Department
1,335
1,024
789
679
486
320
69
94
81
1992
1993
1994
120
142
1995
1996
195
1997
547
562
2002
2003
382
230
1998
1999
2000
2001
2004
2005
2006
2007
2008
2009
2010
2011 Source: Martini Klinik, quality report
St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 14 Key success factors for outcome-­‐driven care improvement •
Develop a system that continuously screens literature and other sources (fellowships, meetings, site visits) for interesting outcome variation •
Discuss variations openly and provide freedom to try out new solutions •
See outcome variations as a chance for collective learning and improving •
Lead by example, walk the talk and start change and learning at the top of the pyramid •
Create a “ we challenge the status quo” – culture (Apple!) •
Find international partners to compare with – best practice solutions can often be found in unexpected places St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 15 ICHOM is a nonprofit dedicated to accelerating development and impact of outcomes measurement ICHOM's three founders with the desire to unlock the potential of VBHC... ...launched ICHOM as a nonprofit + Independent 501(c)3 organization + Idealistic and ambitious goals + Global focus + Engages diverse stakeholders Our mission: We are transforming health care by empowering clinicians worldwide to measure and compare their patients’ outcomes and to learn from each other how to improve. St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 16 ICHOM organizes Working Groups to define Standard Sets of outcomes we recommend all providers track ICHOM Standard Set Outcomes ICHOM facilitates a process with international physician and registry leaders and patient representatives to develop a global Standard Set of outcomes that really matter to patients Physician and registry leaders St. Antonius 2014 JDW.pptx Measures Tier 1 Tier 2 Tier 3 Patient representatives Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 17 Example: ICHOM Localized Prostate Cancer Working Group Adam Glaser, St James’ Institute of Oncology; NHS Jim Catto, University of Sheffield, European Urology Anna Bill-­‐Axelson, Swedish Prostate Cancer Registry Frank Sullivan Prostate Cancer Institute John Fitzpatrick, Irish Cancer Society Steven Jay Frank, MD Anderson David Swanson, MD Anderson Andrew Vickers, MSKCC Adam Kibel, Dana Farber/BWH Michael O’Leary, Dana Farber/BWH Anthony D’Amico, Dana Farber/BWH Neil Martin, Dana Farber/BWH Michael Blute, MGH Howard Sandler, Cedars-­‐Sinai Ronald Chen, University of North Carolina Dan Hamstra, University of Michigan Ash Tewari, Weill Cornell Medical College Hartwig Huland and Markus Graefen, Martini Klinik Michael Froehner, Günter Feick*, Bundesverband Prostatakrebs Selbsthilfe (BPS); Europa UOMO Thomas Wiegel, University Hospital Ulm C.H. Bangma, Erasmus Medical Center Francesco Montorsi, European Urology Editor in Chief Alberto Briganti, Vita-­‐Salute San Raffaele University Hospital, Milan Jabob Ramon, Sheba Medical Center Kim Moretti, South Australian Prostate Cancer Clinical Outcome Collaborative Mark Frydenberg, Prostate Cancer Registry of Victoria Ian Roos*, Cancer Voices Victoria *Patient representative St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 18 ICHOM Standard Set for Localized Prostate Cancer Treatment approaches covered Watchful waiting Active surveillance Prostatectomy External beam radiation therapy ▪ Brachytherapy ▪ Androgen Deprivation Treatment ▪ Other ▪
▪
▪
▪
© 2013 ICHOM. All rights reserved. When using this set of outcomes, or quoting therefrom, in any way, we solely require that you always make a reference to ICHOM a s the source so that this organization can continue i ts work to define more standard outcome sets. St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 19 Once Standard Set Is Defined, ICHOM Working Group Goal Is To Drive Adoption Flyer
User Manual
Academic Publication
A Standard Set of Outcome Metrics for Measuring
the Impact of Prostate Cancer Treatment
▪
▪
Beautifully designed rendition of ICHOM Standard Set Promoted at conferences, Harvard health care courses, and on the ICHOM website
▪
▪
St. Antonius 2014 JDW.pptx Full detail of Standard Set for institutions interested to start collecting or payors looking to integrate into reimbursement programs Includes definitions, inclusion and exclusion criteria, time points for data collection, and index events ▪
▪
Announces the Standard Set to the medical community Explains process to arrive at Standard and motivation for each outcome and risk factor selected Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 20 ICHOM’s ultimate goal is to accelerate the pace of learning and improvement based on meaningful global comparisons Capturing data Data Collection Aggregation Aggregation for for use use Physician reported PROMs EMRs other databases Analysis and Insight Report generation Value based actions Reporting & Using Data St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 21 In our first year, we’ve successfully developed Standard Sets in four conditions, and now we want to ramp up quickly Conditions targeted for 2014 ▪ Stroke ▪ Hip and knee osteoarthritis ▪ Macular degeneration ▪ Lung cancer ▪ Parkinson’s disease ▪ Depression and anxiety ▪ Cleft lip and palate ▪ ... St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 22 ICHOM's plan is to cover more than 50 conditions by 2017 4 conditions 2013 12 conditions 24 conditions 40 conditions 50+ conditions 2014 2015 2016 2017 Share of disease burden in industrialized countries 37% 70% 45% 57% 9% 2013 St. Antonius 2014 JDW.pptx 2014 2015 2016 2017 Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 23 We are proud of our Sponsoring Partners 1. Excluding donations by Cofounders St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 24 For more information please visit www.ichom.org St. Antonius 2014 JDW.pptx Copyright © 2014 by the International Consortium for Health Outcomes Measurement. All rights reserved. 25