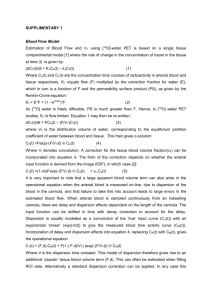
ECMO Intro and Cannulation
advertisement

ECMO AT THE U of M • Two era’s 1974 & 1986 • 1974 - 12 patients. Kolobow Membrane Lung – Roller Pump – Adult and Peds. Patients. No Survivors • 1986 to present - ? Patients. Several different oxygenators, Centrifugal pump only! • ?% overall survival CIRCIUTS FOR ECMO • • • • ARTERIAL VENOUS VENOVENOUS PERIPHERAL CENTRAL (OPEN CHEST) CANNULATION TECHNIQUE NEONATE PERIPHERAL • • • • • Neck cannulation Positioning of patient Sedation Surgical Prep Ideal Cannulae Position Ideal Arterial Cannula Placement A V ECMO • Cannula in Ascending Aorta just above Aortic valve (adjacent coronary ostia) • Supplies oxygenated blood to coronaries and the rest of the circulation. • Cannula tip should avoid proximity with the Aortic valve leaflets and stay out of left ventricle. SINGLE CANNULA VENOVENOUS • Dual luman cannula • Smallest size 14 fr. - limits use to patients above 4 kg. • 15 Fr. – 4kg to < 9kg two lenghts • Flow recirculation 15-30% • Requires higher flows • No lung rest - must ventilate • Requires good cardiac function VENEO/VENOUS IN ADULTS Peripheral cannulation • Drainage from Femoral vein • Return SVC via Jugular access (Or visa versa) • Access may be percutanious or direct cut down • Percutanious is better (less bleeding) • Requires ventilation (no lung rest) • Requires good cardiac function VENO/ARTERIAL ADULTS • Peripheral -Femoral vein, Femoral Artery – Limited distribution of blood centrally – Must have reversal of flow in Aorta for oxygenated blood to reach Heart and Brain – Must place distal perfusion cannula in Femoral artery • Central cannulation - Aorta, Rt. Atrium – Complete cardiopulmonary support