the slide set
advertisement

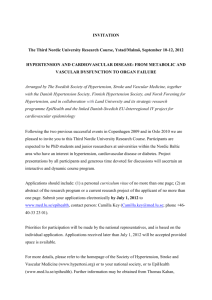
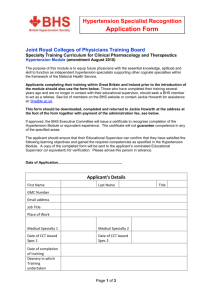
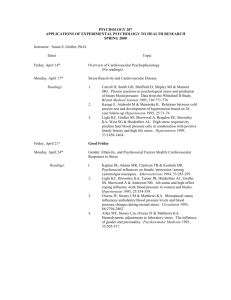
Is it useful to control blood pressure faster in hypertensive patients? Based on: Gradman AH et al. Hypertension. 2013;61:309-318. Cardiovascular diseases vs hypertension • 1 out 3 deaths is due to cardiovascular diseases (2007).1 • Hypertension is the 1st risk factor of cardiovascular diseases.2 • Each increase of 20/10 mm Hg (SBP/DBP) doubles the risk of cardiovascular death.3 • International guidelines advise to control blood pressure below 140/90 mm Hg.4 1. 2. 3. 4. Roger VL et al. Circulation. 2011;123:e18-e209. Hobbs, Richard FD. Vasc Health Risk Manag. 2007;3:711-719. Lewington S et al; Prospective Studies Collaboration. Lancet. 2002;360:1903-1913. Mancia G et al. Eur Heart J. 2013;34:2159-2219. Gradman et al study design • 1762 adult patients with uncontrolled hypertension started on combination therapy (newly initiated on hypertensive therapy). • Respectively analyzed through electronic medical chart (2005-2009). • Matched to an equal number of patients from the add-on therapy cohort (starting with monotherapy). • Mean SBP/DBP of both cohorts 150/84 mm Hg at baseline. • 54% of patients in each cohort had stage 1 hypertension. • The study end points included risk of CV events or all-cause death, time to BP goal attainment,* and rates of health care resource use. *Time to BP goal attainment was defined as the time from treatment initiation to the first of two consecutive target BP readings <140/90 mm Hg or <130/80 mm Hg for patients with diabetes mellitus or CKD. 81% decrease of acute myocardial infarction, P<0.0001, in favor of combination therapy group Figure 1. Incidence rates and incidence rate ratios of cardiovascular events. 34% risk reduction for CV events and all-cause death with firstline combination compared to patients initiated on monotherapy and switched later to combination. Median time to target BP achievement was 18.5% faster with combination than with initiation monotherapy P=0.0040 (9.7 months vs 11.9 respectively) Figure 2. Kaplan-Meier estimates of achieving target blood pressure for each exposure group for all patients. 32% more time was needed to control BP in patients with CV events, median time to target BP achievement (10.6 months vs 15.8) P=0.0011 Figure 3. Kaplan-Meier estimates of achieving target blood pressure for patients with and without a cardiovascular event during the follow-up for all patients. Conclusion • Median time to target BP achievement was 18.5% faster with first-line combination.1 • 34% risk reduction for CV events and all-cause death with first-line combination compared to patients initiated on monotherapy and switched later to combination.1 • More rapid achievement of target BP was found to be the main contributor to the estimated risk reduction.1 • These results reinforce the 2004 VALUE study results on the need for an earlier blood pressure control and its direct link to CV event protection: “BP goals need to be reached within a relatively short time (weeks rather than months).”2 “The blood pressure response after just 1 month of treatment predicted events and survival.”3 • 1. 2. 3. This study enhance the need for an optimized combination to be prescribed in newly diagnosed patients to control blood pressure faster, in order to protect patients earlier from CV events. Gradman AH et al. Hypertension. 2013;61:309-318. Julius S et al. Lancet. 2004;363(9426):2022-2031. Weber MA. Lancet. 2004;363:2049-2051.