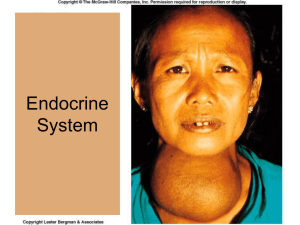
Endocrine Pathology
and Reproductive Pathology
Definitions
• Endocrinology- the study of hormone and glandular
abnormalities- diabetes, thyroid problems, and circus performers
• Hormones- A chemical substance synthesized and secreted by
a specific organ or glands..
• Secreted in small amounts at variable, but predictable rates.
• Circulation through the blood.
• Binding to specific cellular receptors either in the cell membrane or
within the cell.
– Endocrine- hormones that have a biological effect far away.
– Paracrine- hormones that have a biological effect nearby.
– Autocrine- hormones that have a local effect
The Endocrine System
• Exocrine glands transport their
hormones to target
tissues via ducts.
• Endocrine
Emergencies:
– Anterior Pituitary
Hormones from
common:
• Diabetes
• to the unusual:
– Thyrotoxicosis
Endocrine glands
•
•
•
•
•
Pancreas
Pituitary
Thryoid/Parathyroid
Adrenal
Ovary and Testes (reproductive pathology
lecture)
Types/classifications:
– Lipid soluble: bind to plasma proteins to move
• Sex hormones
• Thyroid hormones
• Adrenal hormones
– Water-soluble: able to move more freely
• Pancreatic hormones
• Digestive hormones
Hormone Classification
• Proteins-thyroid stimulating hormone,
insulin, parathyroid hormone
• Amino acids-thyroid hormone,
epinephrine
• Steroids-cortisol, aldosterone,
testosterone
Mechanism of Action of
Hormones
• Circulate in blood stream bound to
transporter proteins or free
• Free hormone is the active hormone
• Enter cells to alter biological activity
Hormone Action
peptide and cathecolamines
R
TSH
TSH
TSH R
protein
T-4
I
2nd
messenger
I
effect
I
I
Hormone Action
Steroid, Thyroid
T-3
TBG
T-3
T-3
R
T-3 R
T-3 R
Increased HR
-receptors
Hormone Functions
• Growth and development: Thyroid, GH,
Sex Steroids, Cortisol
• Reproduction: Estrogen, Testosterone,
FSH, LH, Thyroid
• Homeostasis: Thyroid, Cortisol
• Changes in environment: Cortisol, Thyroid
Aldosterone
• Metabolism Thyroid
• Fluid and electrolyte balance Aldosterone
Interaction of Hormones
Organ
temp metab
T-4
Gluco
Protein
growth neo
synthesis
gensis
HR
Sex
steroids
GH
Skeletal
growth
Hormone Actions
• Produce a response
– Oxytocin stimulates smooth muscle
contraction
– ADH stimulates water absorption
– Prolactin stimulates lactation
• Stimulates an endocrine response
– TSH stimulates thyroid hormone
– LH stimulates testosterone and progesterone
– ACTH stimulates cortisol
Feedback Regulation of the Anterior Pituitary:
Hypothalamus
-
Short Loop
Feedback
?
+
-
Pituitary
+
Target Organ
-
Long Loop
Feedback
Negative feedback
• Important aspect of hormone regulation
• May be exerted by another hormone
– testosterone inhibits LH
– thyroxine inhibits TSH
• May be exerted by a nonhumoral signal
– Calcium inhibit PTH
– Glucose inhibits glucagon
Negative feedback
• Lack of appropriate negative feedback
response provides clues to the
pathophysiology
– Causes of low thyroid hormone?
Negative feedback
• Lack of appropriate negative feedback
response provides clues to the
pathophysiology
– Causes of low thyroid hormone?
• Pituitary problem; ie inadequate TSH
• Primary thyroid problem; can’t make adequate
thyroxine
– How do you differentiate?
Negative feedback
How do you differentiate?
• Measure both TSH and thyroxine
• If both are low
–inappropriate negative feedback
response
–conclude pituitary defect
• If thyroxine is low but TSH is elevated,
conclude primary hypothyroidism
–problem is at level of thyroid g
Patterns of Hormone Secretion
• Constant (thyroid axis)
• Episodic
– On demand (after a meal; during stress)
• Insulin; ACTH
– Pulsatile (most hormones)
– Diurnal (many hormones)
• Light entrained (ACTH/cortisol)
• Sleep entrained (GH, testosterone)
Patterns of Hormone Secretion
• Constant
• Episodic
– On demand
– Pulsatile (most hormones)
– Diurnal (many hormones)
– Infradien
• Ovarian hormones during the menstrual cycle
• Gonadal hormones in seasonally reproducing
species
Endocrine Rhythms:
"It don't mean a thing if it ain't got that swing!"
ACTH
0800
2000
LH
GH
0800
0800
Cortisol
2000
0800
0800
2000
0800
TSH
Testosterone
0800
2000
0800
0800
2000
0800
0800
2000
0800
Endocrine Disorders
• Fall into 2 categories
– Too much
• Often involves tumour
• May be ectopic
– Too little
• Autoimmune response
• Overworked (no longer responds adequately)
Clinical Endocrinology
• Hypofunction of a gland
• Hyperfunction of a gland
• Receptor defect
• Second messenger defect
Endocrine Hypofunction
• Congenital defects in hormone
biosynthesis
• Autoimmune destruction of glands
• Surgery or trauma to glands
• Infiltration by tumors, infection
Endocrine Hyperfunction
•
•
•
•
•
•
Hormone secreting Pituitary tumor
End organ secreting tumor
Autoimmune disease
Inflammation/Infection
Iatrogenic/Facticious
Ectopic hormone secreting tumor
Assessment of Glandular
Activity
• Measure the end organ hormone
• Measure the pituitary regulating hormone
• Suppression tests-to evaluate for hormone
overactivity
• Stimulation tests-to evaluate for
underactivity
• Imaging studies
Diagnosis
• History and physical
• Measure hormones
– One measurement is not diagnostic
– Immunoassays
• Imaging
– Ultrasound or MRI to locate lesion
Treatment
• Hormone deficiency
– Hormone replacement
– Ex. Insulin for diabetes mellitus
• Hormone excess
– Inhibitory drug therapy
• Bromocryptine for hyperprolactinemia
• Androgen antagonist for hirsutism (excess hair)
– Ablation therapy
• Surgical removal of lesion, leaving gland intact
The pancreas
• Located in the left upper
abdominal cavity
• Exocrine and endocrine
glands
• The endocrine function is
due to the cells of the
islets of the Langerhans
-- α cells glucagon
-- β insulin
-- δ somatostatin
Glucose regulation
• Glucose level controlled
by insulin and glucagon
• Insulin promotes a
decrease in blood
glucose
• Glucagon promotes an
increase in blood glucose
Glucose regulation
Fate of glucose
Figure 3.21
Diabetes Mellitus
• Sweet urine (greek)
• Inadequate insulin secretion from
pancreas or insensitivity to insulin leads to
– Increased blood glucose
– Increased glucose in urine
– Increased urine output (polyuria)
– Increased drinking (polydipsia)
• Prevalence is 6.2% (US stats)
• Incidence is 1 million new cases/year
Chronic Complications DM
•
•
•
•
•
Heart disease (2 – 4 fold increase)
Stroke (2 – 4 fold)
Blindness (leading cause of adult blindness)
Neural (60 – 70 % mild – severe impairment)
Kidney disease (leading cause of end stage
renal disease)
• Amputation (60% on non-traumatic amp.)
• Pregnancy complications
Diabetic foot
Diabetes Mellitus
• Type 1 or insulin dependent diabetes
– Juvenile onset diabetes
• Type 2 or insulin independent diabetes
– Adult onset diabetes
Diabetes Mellitus
• Type 1 or insulin dependent diabetes
– Juvenile onset diabetes
– Due to loss of insulin production
– Requires insulin
• Type 2 or insulin independent diabetes
– Adult onset diabetes (often associated with
obesity)
– Insulin levels are high but not high enough
– Insulin resistance
– Boost insulin production or reduce insulin
demand through life style modifications
Pathophysiology
• Because glucose is not getting into cells,
metabolism changes
– Catabolism of fats and proteins instead of
carbohydrates
– Leads to increased fatty acids and ketoacids
– Ketoacidosis results in lowering of pH
• Diabetic coma
• Decompensated metabolic acidosis and death
Diagnosis
• Clinical signs
– PPP (polyuria, polydipsia, polyphagia)
– Fatigue (starvation state reduces
metabolism)
– Weight loss
• Laboratory test
– Elevated fasting glucose
– Glucose tolerance test
Treatment
• Insulin dependent diabetes
– Insulin (fast/short acting;
slow/long acting; intermediate;)
• Subcutaneous injection
• Continuous infusion pump
– Monitor glucose
Treatment
• Non-insulin dependent diabetes mellitus
– Diet (complex carbs, fiber, and protein)
• Reduces the demand for insulin
– Exercise
• Increases uptake of glucose by skeletal muscle by
increasing sensitivity to insulin
– Oral hypoglycemic drug
• Stimulate the beta cells of pancreas to release
insulin (sulfonilurea)
• Reduce insulin resistance (metformin)
Complication of Diabetes
• Acute
• Chronic
Acute Complication
• Insulin induced-hypoglycemia (insulin
shock)
– Error in insulin dose (too much)
– Skipping a meal following insulin dose
– Exercising
– Vomiting
Insulin Shock (insulin-induced
hypoglycemia
• Symptoms (impaired neurologic function)
–
–
–
–
Inability to concentrate
Slurred speech
Lack of coordination
Staggering
• Symptoms are often mistaken as alcohol
intoxication
Acute hypoglycemia
• Symptoms (stimulation of sympathetic NS)
– Sweating
– Tachycardia
– Pallor (vasoconstriction)
– Tremor
– Anxiety
– Loss of consciousness, seizure, death
Acute Complications
• Treatment
– Conscious
• Fruit juice, honey, candy, sugar
– Unconscious
• Intravenous glucose
• Do not administer anything by mouth
Diabetic Ketoacidosis
• Acute (several days rather than hours)
• Caused by
– Inadequate insulin
•
•
•
•
Infection
Stress
Underdosing
Food or alcohol binge
• Results in hyperglycemia & mobilization of
lipids
Ketoacidosis
• Symptoms related to dehydration,
metabolic acidosis, electrolyte imbalance
• Dehydration
– Thirsty
– Dry mucosa
– Warm dry skin
– Low blood pressure
– Oligouria
Ketoacidosis
• Symptoms related to dehydration,
metabolic acidosis, electrolyte imbalance
• Metabolic acidosis (ketoacidosis)
– Rapid respirations
– Acetone breath (sweet, fruity)
– Lethargy
– Unconsciousness if pH falls (ketoacids bind to
bicarbonate)
Ketoacidosis
• Symptoms related to dehydration,
metabolic acidosis, electrolyte imbalance
• Electrolyte imbalance ( Na+2, K+2, Ca+2)
– Abdominal cramping
– Vomiting
– Lethargy
Ketoacidosis
• Treatment
– Administer insulin
– Rehydrate
– Replace electrolytes
– Treat acidosis with bicarbonate
Differential diagnosis of the
unconscious diabetic
• Is it a diabetic coma or ketotic coma?
• Because the cause is different, the
treatment has to be different
Chronic complications of diabetes
•
•
•
1.
Chronic means years
Due to chronic hyperglycemia
Vascular
Mikroangiopati menyerang kapiler dan arteriol:
mata –retinopati diabetika, ginjal–
nefropatidiabetika, syaraf perifer–
neuropatidiabetika, otot dan kulit.
2. Makroangiopati – mengakibatkan penyumbatan
vaskular jika terjadi pd arteri perifer –
klaudikasio intermiten dan gangren
eksteremitas, pd areteri coronaria – angina
pectoris & infark myokard
• Neural
– demyelination of peripheral n. --- numbness
– Autonomic ns --- incontinence, impotence
• Infections
• Spontan abortus, IUFD, big baby,
premature
Neurohypophysis
• Nerve cell bodies in
hypothalamus
• Axons to
neurohypophysis via
infundibulum
• Secrete two major
hormone: ADH &
Oxytocin
ADH (antidiuretic hormone),
vasopressin
– Targets DCT and collecting
tubules
– H2O reabsorption
– blood volume
– BP
– concentration of urine,
volume
23.4b
Diabetes Insipidus
“to pass through; having no flavor”
Three causes
1. Lack of ADH (neurogenic)
• ADH stimulate water absorption of kidney tubule
2. Resistant to ADH (nephrogenic)
3. Excessive thirst (dipsogenic)
Kerusakan pd nuc supraoptik
Poliuri, polidipsi,dehidrasi
What is difference in urine of DI and DM?
sekresi ADH
Diabetes insipidus
Parathyroid glands
• Four nodules located in
the back of the thyroid
gland
• Secreted parathyroid
hormone or
parathormone or PTH
• Action of PTH opposes
action of calcitonin
• Both hormones play a
role in calcium
metabolism
The Function of Calsium
• Important cation in many intra and extra cellular
process
• Extra cellular – mineralization of bone, blood
clotting, and plasma membrane function
• Intracellular – skeletal and cardiac muscle
function, normal action potential, the secretion of
hormone,neurotransmitters, and digestive
enzyme, maintenance transport ion across
membrane, regulation of enzyme function
Calcium regulation:
• Calcitonin promotes
blood calcium decrease,
by:
- 1. calcium deposition on
bone
- 2. calcium dumping by
the kidney
• PTH promotes blood
calcium increase by:
- 1. bone resorption
- 2. calcium reabsorption
by kidney
- 3. increase calcium
absorption by intestine
Calcium Metabolism:
Figure 23-20: Calcium balance in the body
Figure 19.20
Hypercalsemia
• Excess calsium > 10,5 mg /100ml
• Causa
1. PTH dependent hypercalsemia: usually
due to parathyroid adenoma
2. PTH Independent hypercalcemia:
A. PTH related peptide secretion from a
malignancy( bronchus ca, liver ca that
secrete peptide similar to PTH)
B. Vitamin D intoxication
Vitamin D Intoxication
• Hypercalcemia is not necessarily due to a frank
elevation in 1,25(OH)2D but may be due to small
but significant biologic activity of 25(OH)D, and
that elevated 25(OH)D may displace 1,25(OH)2D
from its plasma carrier protein, increasing its
free, biologic activity. The increase in GI
absorption of calcium increase plasma calcium
and and suppresses PTH. This allows increased
calcium excretion and result in marked
hypercalciuria
Symptom
• Neuropsikiatri:Tiredness and lethargy with
muscle weakness
• UT : Polyuria, nocturia, polydipsia and Increased
incidence of kidney stones
• GIT: Nausea, vomiting and constipation
• Cardivasa: hypertension,Increased cardiac
contractions
• Bones: PTH stimulates Ca+2 release from bone
osteoporosis + bone cyst and erosion pd
pinggir2 subperiosteal tulang panjang - osteitis
fibrosistika
Hipocalcemia
•
•
Reduced Ca+2 in the circulation < 9mg per 100ml
Causa:
1. Primary Hypo parathyroid – removal of parathyroid gland
due to thyroidectomi, autoimmune destruction of this gland
and intake vitamin D in adequate
2. Secondary Hypo parathyroid – gastrointestinal mal
absorption of calcium and vitamin D
3. Pseudo hypo parathyroid – PTH receptor function is
defective, and the patient resistant to its action
( appear similar but PTH level Increase because respond to
hypocalcaemia still appropriate but the respond to action of
the PTH in appropriate )
Symptom of hypocalcemia
– Nerves
• Increased excitability leads to muscle twitches and
spasms ex peripheral ( tetany), and central (
seizures) nerve irritability ( manifest with positive
Chvostek’s and Trousseau’s sign indicating
increased facial and radial nerve overactivity)
– Cardiac muscle
• Reduced cardiac output and prolonged Q-T
interval
• Different from skeletal muscle because cardiac
muscle has little intracellular Ca+2
Therapy
• Garam kalsium dan Vitamin D untuk
meningkatkan absorpsi kalsium dlm usus.
• Dosis garam kalsium ( kalsium gluconat,
kalsium laktat, kalsium klorida) 10-15 grm
• Dosis Vitamin D 50.000 – 150.000 unit per
hari
Calcitonin
• Synthesized in C cells (parafollicular cells
dispersed in thyroid)
• Discovered by Dr. Harold Copp; Dept
Physiology UBC in 1961
• Calcitonin has opposite effect to PTH
– Decreases [Ca++] by increasing bone uptake
of Ca++ and reducing absorption at kidney
and intestine
Other causes of calcium imbalance
• Hypercalcemia
– Bone cancer
– Immobility
– What levels of PTH/Calcitonin would you
expect?
• Hypocalcemia
– Renal disease
• Decreased activation of Vit D and increased P04
• Vit D necessary for Ca++ absorption; P04 inhibits it
– What levels of PTH/Calcitonin would you
expect?
Pituitary Gland Pathology
•
•
•
•
•
•
Thyroid stimulating hormone (TSH)
Growth hormone (GH)
Adrenocorticotrophin (ACTH)
Prolactin (PRL)
Luteinizing hormone (LH)
Follicle stimulating hormone (FSH)
Pituitary Tumours
Symptoms of Pituitary Tumours
•
•
•
•
•
Headache (intracranial pressure)
Drowsiness
Seizure
Visual defects (pressure on optic chiasm)
Abnormal hormone secretion
Pituitary tumours
• Abnormal hormone secretion
– Hyperprolactinemia
• Most common type of pituitary tumour
• Galactorrhea
• Amenorrhea
– ACTH
• Cushings disease
– GH
• Gigantism (prepubertal)
• Acromegaly (postpubertal)
Pituitary tumours
• Can destroy pituitary gland
– Compression compromises vascular supply
– Panhypopituitaryism
• Hypopituitarism unrelated to tumour
– Sheehan’s syndrome
• Another cause of panhypopituitarism
• Vascular collapse following an obstetrical hemorrhage
– Pituitary stalk transection
• MVA
• Panhypopit. except PRL is elevated
Pituitary tumour treatment
• Hormone deficiency
– Hormone replacement
– Multiple hormones for panhypopituitarism
• Hormone excess
– Inhibitory drug therapy
• Bromocryptine for hyperprolactinemia
– Ablation therapy
• Surgical removal of lesion, leaving gland intact
Feedback
control of
growth
hormone
Regulation of Growth Hormone
Secretion
• GH secretion controlled primarily by
hypothalamic GHRH stimulation and
somatostatin inhibition
• Neurotransmitters involved in control of
GH secretion– via regulation of GHRH and
somatostatin
Regulation of Growth Hormone
Secretion
• Neurotransmitter systems that stimulate
GHRH and/or inhibit somatostatin
– Catecholamines acting via a2-adrenergic
receptors
– Dopamine acting via D1 or D2 receptors
– Excitatory amino acids acting via both NMDA
and non-NMDA receptors
Regulation of Growth Hormone
Secretion
-adrenergic receptors stimulate
somatostatin release and inhibit GH
-adrenergic receptors inhibit
hypothalamic release of GHRH
Regulation of Growth Hormone
Secretion
• Additional central mechanisms that control
GH secretion include an ultra-short
feedback loop exerted by both
somatostatin and GHRH on their own
secretion
•
Growth hormone vs.
metabolic
state
When protein and energy intake are adequate, it is
appropriate to convert amino acids to protein and
stimulate growth. hence GH and insulin promote
anabolic reactions during protein intake
• During carbohydrate intake, GH antagonizes insulin
effects-- blocks glucose uptake to prevent hypoglycemia.
(if there is too much insulin, all the glucose would be
taken up).
• When there is adequate glucose as during absorptive
phase, and glucose uptake is required, then GH
secretion is inhibited so it won't counter act insulin
action.
Growth hormone vs.
metabolic state
• During fasting, GH antagonizes insulin action and helps
mediate glucose sparing, ie stimulates gluconeogenesis
• In general, during anabolic or absorptive phase, GH
facilitates insulin action, to promote growth.
• during fasting or post-absorptive phase, GH opposes
insulin action, to promote catabolism or glucose sparing
Growth
hormone
and
metabolic
state
Clinical assessment of GH
• Random serum samples not useful due to
pulsatile pattern of release
• Provocative tests necessary
– GH measurement after 90 min exercise
– GH measurement immediately after onset of sleep
• Definitive tests
– GH measurement after insulin-induced
hypoglycemia
– Glucose suppresses GH levels 30-90 min after
administration– patients with GH excess do not
suppress
– Measurement of IGF-1 to assess GH excess
Acromegaly and Gigantism
• Caused by eosinophilic adenomas of
somatotrophs
• Excess GH leads to development of
gigantism if hypersecretion is present during
early life– a rare condition
– Symmetrical enlargement of body resulting in true
giant with overgrowth of long bones, connective
tissue and visceral organs.
• Excess GH leads to acromegaly if
hypersecretion occurs after body growth has
stopped.
– Elongation of long bones not possible so there is
over growth of cancellous bones– protruding jaw,
thickening of phalanges, and over growth of
visceral organs
Acromegaly
Acromegaly
A) before
presentation;
B) at admission
Harvey Cushing’s
first reported case
The thyroid gland - Chp 21 p 623-625
• Located in the neck, just below
the larynx
• Secrete 2 types of hormone:
- thyroid hormones stimulate
cell metabolism,
triiodothyronine (T3) and
thyroxine (T4) – iodine is
needed to synthesize these
hormones
- calcitonin decrease blood
calcium
Figure 6.8a
Thyroid hormones
• T3 and T4 secreted
by the follicular cells
• Stored as colloid
• Parafollicular cells (C
cells) secrete
calcitonin (Chp 19)
Thyroid Hormones T3 and T4
• Target organs: all cells
• Role: Increase cell metabolism, oxygen
consumption
• Permissive role for some other hormones
(growth hormone)
Thyroid disorders (normal PSL)
Goiter
• Both hypo and hyperthyroidism can have
goiter as a symptom
• Goiter is a swelling of the neck due to
hypertrophy of the thyroid gland
• How can one explain that?
Goiter in hypothyroidism
•
•
•
•
•
•
Most often due to a lack of dietary
iodine
The thyroid hormone is unable to
synthesize a functional thyroid
hormone (T3 and T4)
The person express symptoms of
hypothyroidism
The nonfunctional T3/T4 cannot
promote a negative feedback on
TRH and TSH
the hypotalamus and pituitary
gland increase their secretions
the thyroid gland is stimulated to
secrete more T3 and T4 …
In children, the lack of functional
T3/T4 result in cretinism, a form a
mental retardation
Goiter in hyperthyroidism
• The cells secreting TRH or
TSH on the hypothalamus and
pituitary gland (respectively)
have become abnormal and no
longer are sensitive to the
negative feedback they
continue to secrete TRH or
TSH continuous stimulation
of the thyroid gland with
excess thyroid hormones
being formed
• symptoms of
hyperthyroidism
Thyroid Disorders
• Hypothyroidism (inadequate thyroid
hormone secretion)
• Causes
– Pituitary deficiency of TSH
– Thyroid gland malfunction
• TSH measurement will differentiate
between the two causes
Hypothyroidism
• Hashimotos thyroiditis
– Autoimmune disease of thyroid
• Myxedema
– Adult onset
• Cretinism
– Undiagnosed congenital hypothyroidism
– Mental retardation; growth restriction
– Neonatal screening now standard (TSH)
Hypothyroidism
•
Clinical symptoms
–
–
–
–
–
–
–
–
–
–
–
–
–
•
Reduced metabolism
Endemic goiter (non functional)
Pale, cool, edematous
Cold intolerant
Slow heart rate (bradycardia)
weakness
Decreased appetite/weight gain
Menstrual irregularities or Heavy menstrual
periods
loss of libido
Constipation
Memory and mental impairment and
decreased concentration (Slowed thinking )
Reflex delay
Depression
Treatment; thyroxine
Thyroiditis
• Inflammation of the
thyroid gland
• Can be acute,
subacute, chronic
• Hashimoto’s Disease
– Chronic thyroiditis
– Caused by a reaction
of the immune system
against the thyroid
gland.
Iodine Deficient Goiter
• Seen in geographic
areas where the
natural supply of
iodine is deficient
Goiter Formation
Iodized salt
Figure 20-9.Three women of the himalayas with typical endemic goiters.
Figure 20-1. Map showing world wide distribution of iodine deficiency disorders (IDD) in developing countries.
Myxedema
• Most extreme, severe stage of
hypothyroidism
• Hypothermia
• Increasing lethargy
• Coma
Figure 21-19. The dramatic case of Maria Richsel, the first patient to have come to Kocher’s attention with
postoperative myxedema following total thyroidectomy. A. The child and her younger sister before the
operation. B. The changes nine years after the operation. The younger sister, now fully grown, contrasts
vividly with the dwarfed and stunted patient. Also note Maria’s thickened face and fingers, which are
typical of myxedema. Because of this and other patients with the same problem, Kocher stopped
performing total thyroidectomies. For this work, demonstrating the physiological importance of the thyroid
gland in man, Professor Kocher was awarded the Nobel prize. From: Kocher T. Uber Kropfextirpation und
ihre Folgen, Arch Klin Chir 29:254, 1883, with permission.
Congenital Hypothyroidism
Cretinism
Stunted growth
Neurological/
cognitive
defects/mental
retardation
Infantile
appearance-puffy
face protuberant
abdomen
Hyperthyroidism
• Hyperthyroidism or toxic goiter; (Graves
disease)
• Increased thyroid hormone secretion
• Symptoms
– Increase metabolism
– Increased sympathetic NS
– Exophthalmus
• Treatment
– Radioactive iodine; surgery; medication
Clinical Manifestations
1. Heat intolerance.
2. Palpitations, elevated systolic BP.
3. Weight loss.
4. Menstrual irregularities and decreased libido.
5. Increased serum T4, T3.
6. Exophthalmos (bulging eyes)
7. Goiter.
8. Insomnia.
9. Muscle weakness.
10. Heat intolerance.
11. Diarrhea.
Figure 10-5.
(a) This MRI image from a
patient with Graves'
ophthalmopathy provides a
coronal view of the eyes. In
this depiction the muscles
appear white, and are
enormously enlarged,
especially in the left eye.
(b) In this transverse view the enlarged muscles are
seen (appearing dark against the light fat signal) and
the exophthalmos is apparrent.
I123 uptake and scan
Adrenal gland
• Located on superior surface
of kidney
• Adrenal medulla
– Secretes norepinephrine &
epinephrine
– Targets sympathetic effector
organs
– Emotional arousal
• Adrenal cortex
– Secretes steroid hormone
– sER
Adrenal cortex
• Aldosterone
• Cortisol
• Sex steroid ( androgen , esterogen)
Figure 6.12b
Figure 21.15
Adrenal gland hormones
Regulation
Glands
Hormones
Target
organs
Action
Pathology
Reflex
Adrenal medulla
Epinephrine
ANS target
organs
Fight/flight
Stress
Blood Pressure
Adrenal cortex
- Mineralocorticoid =
aldosterone
DCT from renal
tubule
- promote sodium
reabsorption
Not enough"
Addison disease
CRH ACTH
Glucocorticoid =
cortisone
Many cells
Mobilize fuels –
stress adaptation
Excess hormone:
Cushing
syndrome
GnRH GN
Estrogen
Testosterone
Sexual organs
- Sex organ
maintenance
- Gamete
development
Infertility
Adrenal Gland Diseases
• Adrenal Medulla
– Pheochromocytoma
• Adrenal Cortex
– Cushing’s Syndrome
– Addison’s Disease
Pheochromcytoma
– Benign tumour of adrenal medulla
– This tumor causes hypersecretion of epinephrine and
norepinephrine which produces an effect similar to
continuous sympathetic nerve stimulation
– Symptoms include headache, hypertension, elevated
metabolism,palpitation, sweating, hyperglicemia and
anxiety
– The body to become totally fatigued and susceptible
to other disease
– Surgery
Cushing’s Syndrome
Excess glucocorticoids
– ACTH secreting tumour
( Pituitary or Paraneoplastic syndrome)
– Adrenal tumour (glucocorticoid
secreting)
– Glucocorticoid therapy of chronic
inflammatory conditions (iatrogenic)
Metabolic effect of glucocorticoid
• Promote breakdown protein in the
muscle,skin and vascular – muscle
weakness and atrophy, striae,
hematome,petekiae or echimoses
• Promote bone resorption / decrease bone
formation – osteoporosis – pathologies
fracture ( vertebrae – collapse vertebrae,
LBP and tall)
Metabolic effect of glucocorticoid
• Promote lipolysis and ketogenesis
• Truncal distribution / truncal obesity – the
distribution of adipose tissue accumulate in
central of the body – moon face, buffalo hump,
memadatnya fossa supraklavikularis
• Increased gluconeogenesis ( liver use amino
acid from muscle and glycerol from fat as
gluconeogenic precursors )and decrease insulin
mediated glucose up take in muscle and fat –
hyperglycemia
• Immune system -- Anti-inflammatory, suppresses
immune response
Metabolic effect of glucocorticoid
• Immune system -- Anti-inflammatory, suppresses
immune response.
Anti-inflammatory – suppresses hyperemia, cell
extravasations, cell migration, permeability of
cell,also suppress release of kinin vasoaktif from
plasma protein and phagocytes, effect on mast
cell suppress histamine synthesis and
anaphylaxis reactions
• Increase gastric secretion – hcl and pepsin
increase and decrease mucous protective factor
– gastric ulcers
Features of Cushing’s
• Cushingnoid
– Obesity
– Moon face
– Buffalo hump
– Reduced muscle mass in
limbs
– Stria
– Increased hair growth
Cushings
Buffalo hump
Striae, hirsutism, central adiposity
Adrenal Adenoma
Cushing’s Syndrome
• Other features
– Osteoporosis
– Insulin resistance
• gluconeogenic effect of cortisol
– Delayed healing/increased infection
• Immune suppression
– Reduced stress response; may require
glucocorticoid therapy
Diagnosis
• Pengukuran kadar cortisol plasma dan urine
• Tes spesifik – ada/ tidaknya irama sirkadian
normal dan ada/tidaknya feedbaack negatif
• Pemeriksaan sinar X tengkorak – sella tursica
rusak– tumor hipofise
• Angiografi vena adrenal– distorsi pola memberi
kesan hiperplasi adrenal/ tumor adrenal
• Photo scanning adrenal
Terapi
• Tumor – reseksi tumor transfenodial
• Ada hyperfungsi ttp tumor tdk dpt
ditemukan nyata dipergunakan iradiasi
kobalt pd kel hipofisis sbg penggantinya
• Adrenalektomi total dg diikuti pemberian
kortisol dosis fisiologi
Farmakologi dan Penggunaan
kortikosteroid sintetik
•
Aktivitas anti inflamasi/ peradangan sering digunakan
dlm klinik baik lokal maupun sistemik untuk terapi
asma, rheumatoid artritis, reaksi alergi akut dll
• Dg merubah struktur kimia – sifat farmakologis nya
juga berubah mis
1. pemasukan ikatan ganda diantara mol carbon 1 &2 dr
kortisol dihslkan prednisolon yg aktivitas
antiperadangannya lebih hebat dan aktivitas retensi
natrium lbh kecil dr senyawa induknya
2. Pemasukan atom fluorin dlm posisi alfa pd karbon 9
intisteroid– 9 alfa –flurokortikoid – efek retensi natrium
kuat spt aldosteron
Addison’s Disease
• Deficiency of adrenalcortical hormones
– Glucocorticoids
– Mineralocorticoids
– Androgens
• Primary adrenal insufficiency is usually caused by
autoimmune destruction, destructive tumours (
lung cancer) or tuberculosis of the adrenal gland
• Secondary adrenal insufficiency is usually caused
by: hipopituitarism, abrupt withdrawal of long term
exogenous glucocorticoid therapy – adrenal
insufficiency because of suppression of the HPA
axis
Addison’s disease
Hypoglycemia ( Cortisol – diabetogenic effect)
sodium and potassium imbalance, dehydration,
hypotension ( aldosteron)
Anorexia, rapid weigh loss
general weakness
Poor stress response ( Cortisol – need for
normal stress respond)
Risk of infection
Hyperpigmentation (Cortisol – suppress MSH)
Rambut axila dan pubis rontok dan rambut
ekstremitas berkurang nampak jelas pd wanita
Features of Addison’s d.
Diagnosis dan terapi
• 17 hidroksikortikoid urine, kdr kortisol
plasma rendah, kdr ACTH plasma
meningkat
• Pemberian ACTH intravena tdk
meningkatkan kdr kortisol plasma
• Serum elektrolit abnormal : hiponatremia,
hiperkalemia, dan asidosis metabolik
• Terapi dg 20-30mg kortisol dan analog
aldosteron 9 alfa flurokortisol
Reproductive Pathophysiology
• Review of female reproductive system and
normal menstrual cycle
• Review of male reproductive system and
infertility
• Female infertility
– Menstrual related
– Structural
• Cancer
– Testicular, prostate, ovarian, cervical, uterine, breast
Female Anatomy
Female Anatomy
Structure and Function
• Ovaries
– Produce gametes and steroids
• Fallopian tubes
– Collection (fimbriae) and transport of ova
– Site of fertilization
• Uterus
– Site of implantation and gestation
• Cervix
– Portal between vagina and uterus
Hormones of the menstrual cycle
• Ovarian hormones
– Estrogen and progesterone
• Pituitary hormones
– Gonadotrophins (LH and FSH)
• Brain hormone
– GnRH
GnRH or LHRH
decapeptide
various n. project to median eminence
pulsatile release
receptor downregulation
Hypothalamus
Pituitary LH & FSH
Follicle stimulating hormone
–
–
–
granulosa cell proliferation
induction of aromatase
stimulation of estrogen
Luteinizing hormone
–
–
–
stimulation of testosterone
triggers ovulation
stimulates progesterone
FSH
LH
Steroidogenesis
in the Ovary
LH
LH
receptor
cholesterol
ATP
cAMP
androstenedione
androstenedione
Theca interna
circulation
basement membrane
androstenedione
ATP
Aromatase
Granulosa cells
cAMP
estrogen
FSH
receptor
FSH
Follicular fluid
Ovarian hormones
estrogen (granulosa cells)
progesterone (corpora luteal cells)
testosterone (theca interna cells)
Estrogen targets
granulosa cells
mammary gland
uterus
hypothalamic - pituitary axis
Progesterone targets
mammary gland
uterus
hypothalamus
Menstrual Cycle
Follicular phase
–
–
–
1st day of menses to ovulation
Endometrial proliferation
Estrogen > Progesterone (estrogen dominated)
Luteal phase
–
–
–
from ovulation to menses
endometrial secretion
Progesterone > Estrogen
Male Reproduction
• Structure
• Function
• Dysfunction (male infertility)
Male Anatomy
Male Reproduction
• Testes
– Sperm production (Spermatogenesis or
gametogenesis)
– Testosterone production (steroidogenesis)
Male Reproduction
• Testes
– Descend prior to birth into the scrotum
– Lower temperature necessary for functional
sperm
– Composed of seminiferous tubules (site of
sperm production)
Semiferous Tubule
Seminiferous Tubule
Male Anatomy
• Intratesticular
– Seminiferous tubule
– Efferent ducts (collection ducts)
– Epididymis (maturation; short term storage)
• Extratesticular
– Vas deferens (vasectomy)
– Ampulla (situated just above SV; storage)
– Seminal vesicles (site of seminal fluid
production and storage)
Seminal Vesicles
• Located near bladder
• 95% of ejaculate is
seminal fluid
• Energy source for
sperm (fructose)
Prostate gland
• Encapsulates the
urethra and
ejaculatory duct
• Secretion raises pH of
sperm
• Bulbourethral gland or
Cowper’s gland
– Adds alkaline mucous
to ejaculate
Male Reproductive Hormones
• GnRH
– Stimulates LH/FSH
• FSH
– Stimulates spermatogenesis
• LH
– Stimulates steroidogenesis
• Testosterone
– Sperm maturation, secondary sex charact.,
vocal cords, hair follicle, muscle, libido
Male Infertility
• Infertility; no conception after 1 year of
unprotected, regular intercourse
• 40 % of infertility is associated with a male
factor
– 20 % male alone; 20 % both male and female
• Majority of male infertility associated with
abnormal semen parameters
Semen Analysis
• Volume (2-4 ml)
• Viscosity
• Sperm density
– Greater than 20 million/ml
– Average is 100 million/ml
• Sperm motility
– Greater than 40 %
• Sperm morphology
– Less than 60 % abnormal
considered normal
Male Infertility Treatment
• Life style changes
– Marijuana, cigarettes, work environment
• Medical therapies don’t exist
• Fertility enhancement procedures
– Intrauterine insemination of concentrated sperm
– In vitro fertilization (IVF)
• Ovarian stimulation, oocyte collection, fertilization in vitro, in
vitro embryo development for 2-4 days, embryo transferred
into uterus
– Intracytoplasmic sperm injection (ICSE) combined
with IVF
ICSE
Female Infertility
• Anovulation
– Amenorrhea lack of menstruation
• Structural
– Congenital or secondary
• Immunologic
– Antibody production against sperm
– Immune response to fetus
Anovulation (amenorrhea)
• Primary amenorrhea
– Menarche never occurred
– Genetic disorders
• Turners syndrome (XO)
– Congenital disorders of brain, pituitary, ovary
or uterus
• Secondary amenorrhea
– Cessation of menstrual cycles after a period
of regular cycles
Causes of 2O amenorrhea
• CNS or pituitary tumours
– Prolactinoma most common
• Inhibition of GnRH secretion
– Stress, excessive exercise, weight loss
• Obstruction of outflow tract
– Leiomyoma (fibroid; benign tumour of
myometrium)
– Asherman’s syndrome (scarring of uterine
lining)
Uterine Fibroids
Treatment of 2O amenorrhea
• Surgical resection of tumours
• Education about stress reduction
– Importance of healthy diet, exercise in
moderation
• Oral Contraception therapy if not trying to
conceive
– osteoporosis prevention
• Endocrine therapy
– Bromocryptine to suppress prolactin
– Stimulate gonadotrophin level
Blocked fallopian tubes
Scarring due to endometriosis
Blocked fallopian tubes due to PID
Contraceptive tubal resection
Endometriosis
• Ectopic endometrium
– endometrium outside
the uterine cavity
• Scarring
• Pain
– dysmenorrhea
– dyspareunia
Endometriosis
Structural causes contin.
• Blocked fallopian tubes
– Pelvic inflammatory disease (stds or ruptured
appendix)
• Treatment
– Surgical reanastomosis
– Resection of endometriosis
– IVF
Tubal Reanastomosis
Medical treatment of endometriosis
or fibroids
• Hormonal therapy
– Inhibition of menstrual cycle
• GnRH agonist (lupron, zoladex)
• Danazol (androgenic steroid)
• OC
– Medical therapies that do not interfere with
the menstrual cycle (and therefore do not
interfere with fertility) do not exist
Reproductive Cancers
•
•
•
•
•
•
Testicular
Prostate
Cervical
Uterine
Ovarian
Breast
Testicular Cancer
• Most common tumor in young men
• Primarily in men 15 – 35 yo
• Metastasize to lymph nodes, lungs, liver
and bone
Testicular cancer etiology
• Familial component
• Increased in undescended testis
• Connection with infection or trauma is not
supported
Testicular Cancer
Signs & Symptoms
• Hard painless unilateral mass
• Picked up on self exam
• Diagnostic test
– CT scan, tumor markers (hCG, AFP)
Testicular Ca Treatment
•
•
•
•
Orchidectomy
Radiation
Chemotherapy with cytotoxic drugs
Cure rate is excellent
Prostate Pathophysiology
• Benign prostatic hyperplasia (BPH)
– Enlargement of the prostate (central area)
– Formation of nodules around the urethra
– Does not progress to cancer
• Prostate cancer
– Adenocarcinoma surface epithelia
– Metastasis to lymph nodes, liver, bone,
adrenal, lung in advanced stage
BPH
• Symptoms
– Hesitancy and reduced urinary stream due to
compression of urethra
– Urinary retention can lead to cystitis
• Treatment
– Surgical (infrequent)
– Medical
• Anti-androgen
• Alpha adrenergic blocker
Prostate Cancer
• Etiology unknown
– Genetic, environmental, hormonal?
• Early detection is vital
– Prostate specific antigen (PSA)
• Also elevated with BPH and infection
– Rectal examination
– Diagnosis confirmed by ultrasound and biopsy
Treatment of Prostate Ca
• Surgery (prostatectomy) and radiation
– Implants
– Anti-androgen (flutamide) if tumor is androgen
sensitive
Cervical Cancer
• Starts as dysplasia of squamous epithelial cells at
columnar junction of the external os.
• Early detection by Pap smear
• Signs and symptoms include spotting and watery
discharge (can lead to anemia & wgt loss in severe
cases
Cervical Cancer
Columnar junction
Early invasive
disease
Squamous epithelium
Cervical Cancer Etiology
• Linked to oncogenic stds
– Herpes simplex virus type 2
– HPV (human papillomavirus)
• Incidence increases with multiple sexual
partners
• Average age is 35 for early stage disease
• Takes 5 - 10 years to develop into invasive
disease
Signs and Symptoms
• Asymptomatic at the early stage (in situ
carcinoma)
• Pap smear will detect dysplasia prior to in
situ carcinoma
• Spotting is an indication of invasive
carcinoma
Cervical Cancer Treatment
•
•
•
•
Surgery and radiation
5 year survival is 100 % if detected early
Annual Pap
Vaccine?
– Clinical trials of a HPV vaccine very promising
Carcinoma of Uterus
• Most common in the 55 –
65 age range
• Screening test not
available
• Unexpected bleeding is
the initial sign
• Confirm with endometrial
biopsy
Carcinoma of Uterus
Pathophysiology
• Endometrial hyperplasia leading to
dysplasia
• Unopposed estrogen stimulation
– Source is fat cells in postmenopausal women
– Menstruation is protective
– HRT should include a progestin when uterus
is present
Uterine Cancer Treatment
• Hysterectomy
• Radiation
• 90% five-year survival if non-invasive
(confined to the uterus; lymph nodes neg)
Ovarian Cancer
• 1.8% life time risk
• 30,000 NA women diagnosed each in 2000
(15,400 died from ovarian cancer; more than all
the other reproductive cancers combined)
• Asymptomatic at early stages
• No tumor marker
• Symptoms (bowel or bladder problems) occur
only in late stages
• Prognosis extremely poor (5 yr survival rate only
15 - 20%)
Risk Factors
• Personal or family history of breast, ovarian,
endometrial, prostate or colon cancer
• One or more first-degree relatives (mother,
sister, daughter) who have ovarian cancer
• Several family members with ovarian and/or
breast cancer
• Carrying a BRCA1 or BRCA2 gene mutation
• Uninterrupted ovulation (infertility, never used
birth control pills or never pregnant)
• Increasing age
Ovarian Cancer Therapy
• Surgery
– Debulking tumor
– Remove obstruction
• Chemotherapy
• Radiation
• Palliation
Ovarian Cancer Prophylaxis
• Prophylactic oophorectomy in women with
multiple risk factors
– Strong family history
– Breast cancer before age 50
– BRCA1/2 mutation
Breast Cancer
• Second most common
cause of death due to
cancer in women
– Life time risk is 1 in 9
– 50 % in women with BRCA
gene mutation (mean age of
detection = 41 yo)
– Risk of dying from breast
cancer is 1 in 30
By age 30
By age 40
By age 50
By age 60
By age 70
By age 80
Ever
1 in 2212
1 in 235
1 in 54
1 in 23
1 in 14
1 in 10
1 in 8
Breast Cancer Etiology
• Familial
– daughters with mother with bc have >risk
• Increased incidence with delayed
childbirth
– Hormones of menstrual cycle?
– Breast differentiation with lactation/breast
feeding?
Breast cancer treatment
• Surgery/radiation/chemotherapy
• If estrogen receptor positive
– Tamoxifen (estrogen antagonist)
– Aromatase inhibitor (letrozole or arimidex)