Bronchoscopy - Respiratory Therapy Files
advertisement

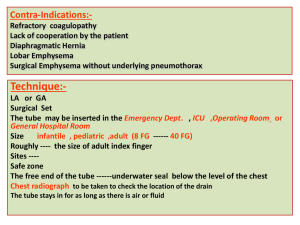
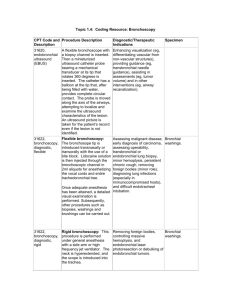
Bronchoscopy • A technique for assessing and examining the bronchi by means of a bronchoscope, which is used for both therapeutic and diagnostic purposes Rigid Bronchoscope • Consists of a hollow metal tube with a light on its distal end. • Tube is inserted orally, then passed between the vocal cords into the trachea. • Is useful for removing aspirated foreign bodies and thick secretions from the lungs. Flexible Fiberoptic Bronchoscope • Consists of a collection of thin, threadlike glass strands called fiberoptic filaments with a light source projected to its distal end for visualization. • Is better tolerated by patients than the rigid bronchoscope because of its more flexible nature; it is therefore more commonly used. Flexible Fiberoptic Bronchoscope Indications • Removal of foreign bodies • Removal of mucus plugs and thick secretions – Is normally performed when secretions cannot be removed by routine suctioning techniques • Atelectasis that affects a lobe or an entire lung • Pulmonary hemorrhage – To locate the area of bleeding – To control bleeding by instillation of epinephrine or iced saline lavage at the bleeding site • When tracheal intubation is difficult as a result of upper airway trauma, obesity, tumors, or spinal deformity – The ET tube is slipped over the fiberoptic bronchoscope; the scope should protrude well past the end of the ET tube. – The vocal cords are visualized, and the scope is advanced through the cords to the midtracheal level, where the ET tube is then advanced over the scope to the proper position. The scope is then withdrawn. • Biopsy of suspected tumors • When sputum is needed for culture and sensitivity studies Complications • Hypoxemia – – • – • – • Results from irritation of the airway. Bronchodilator should be readily available. Arrhythmias – – Result from vagal stimulation. Monitor ECG and remove bronchoscope until cardiac status is stabilized. Results from sedatives given before the procedure. Monitor respiratory status closely. Hypotension – – • May occur during insertion. May occur after biopsy. Respiratory depression – Bronchospasm – – • Makes advancing the tube more difficult. Bronchodilator should be readily available. Hemorrhage – – Laryngospasm – • Monitor oxygen saturation during procedure. Increase oxygen percentage during procedure. • Results from vagal nerve stimulation. May result from sedatives given before the procedure. Pneumothorax – – Results from inadvertent puncture of the lung. Monitor respiratory status closely. Preparation • A mild sedative should be administered to the patient 1 to 2 h before the procedure. – Diazepam (Valium) or midazolam (Versed) – conscious sedation: just enough to allow the patient to follow commands yet still be comfortable. • The airway must be dry during the procedure to aid in visualization – Atropine 1 to 2 h before the procedure. – Atropine may also decrease vagal tone, resulting in a decreased potential for bradycardia and hypotension, which can occur during the procedure. • The bronchoscope should be lubricated with a water-soluble jelly for nasal insertion. – Lidocaine (Xylocaine) jelly is used both as a lubricant and for its anesthetic effects. – In some cases, the RCP administers aerosolized lidocaine before the procedure. RT Role During Bronchoscopy • Prepare the patient and explain the procedure. • Administer aerosolized local anesthetic to the patient's upper airway. • Conduct patient monitoring throughout the procedure. – – – – – Pulse and blood pressure Respiratory rate ECG Oxygen saturation Level of consciousness • Collect sputum and tissue samples that the physician has obtained and prepare them for laboratory analysis. • Clean the bronchoscope properly after the procedure. The Centers for Disease Control and Prevention recommends that bronchoscopes be sterilized by immersion in glutaraldehyde (Cidex) for 3 to 10 h. » • (Persing, Gary. Respiratory Care Exam Review: Review for the Entry Level and Advanced Exams, 3rd Edition. Elsevier Health Sciences, 112009. 5.2).