King LTS-D Airway Device Training for First Responders
advertisement

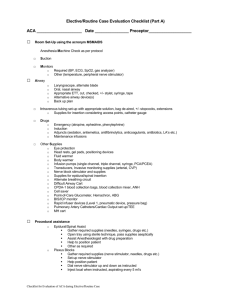
King LTS-D Blind Insertion Airway Device HCEC First Responder Organization Training Goal • To prepare HCEC First Responder Organization personnel to safely utilize the King LTS-D Blind Insertion Airway Device within the scope of the HCEC Fire and Rescue Medical/Trauma Guidelines Objectives • Upon completion of the didactic and practical sections of this program, the candidate will be able to: – Integrate the King LTS-D BIAD into traditional basic life support airway management – Demonstrate safe insertion of a King LTS-D BIAD – Demonstrate and/or describe procedures for ensuring proper placement of the BIAD Assessment • Skills will be verified using an advanced airway training mannequin under the supervision of an approved HCEC FRO Trainer • Candidates must perform the skill without critical errors as listed on the HCEC Psychomotor Skill Verification sheet for Blind Insertion Airway Device Definition • The King LTS-D is a single use blind insertion airway device (BIAD). • May be used by HCEC FRO EMT-B’s, EMTI’s and Paramedics, under the Fire and Rescue Medical/Trauma Guidelines, who have been credentialed by the HCEC Clinical Division Description • A curved tube with ventilation ports between • • • • two inflatable cuffs. The distal cuff is designed to seal the esophagus. The proximal cuff is designed to seal the oropharynx. At the proximal end of the tube is a 15mm connector to be used with standard breathing circuit or resuscitation bag. The King airway is latex free product. Size determined by Pt’s height: • Yellow: 4-5 ft • Red: 5-6 ft • Purple: > 6 ft Indication • Cardiac arrest after assuring continuous compressions, defibrillation and BLS airway management have been completed. Contraindications • Patients who are conscious or who have an intact gag reflex. • Patients with known esophageal disease, i.e. varices, alcoholism, cirrhosis, etc. • Patients known or suspected to have ingested caustic substances. • Deforming facial trauma that prevents proper sealing of the airway Precautions: • Vomiting and aspiration • Excess pressure in abdomen Instructions for use • Use appropriate PPE. • Prepare, position, and oxygenate the patient. • Choose appropriate size based on patient’s • • • height. Test cuffs by inflating to recommended volume of air and deflate cuffs completely before attempting to insert. Generously lubricate tube using a water based lube. Have suction available. Insertion: • Position the head in a slightly • • • sniffing position, unless spinal injury is known or suspected, then maintain cervical alignment and keep the head in a neutral position. Insert King rotated 45-90 degrees laterally and insert into mouth As you gently advance the tube rotate tube to midline. Advance tube until base of connector aligns with teeth or gums. Cuff inflation: • Inflate cuffs with minimum volume necessary to • • • • seal the airway according to tube size. Attach to resuscitator bag and ventilate, gently withdrawing the airway until ventilation is easy and free flowing. Monitor end tidal CO2 if available. Assure chest rise and fall. Auscultate breath sounds. Secure tube, using a commercially approved device, noting depth of tube placement. Transition of care: • Relay to the receiving medic unit: – Time, size and depth of tube placement. – Patient response to procedure. Remember: • When placing a King airway during CPR minimize interruption of CPR and place tube while CPR is in progress. • If spinal injury is known or suspected, maintain a neutral head alignment and initiate cervical spine precautions concurrently with airway management. Hands-On Practice