Using Root Cause Analysis to Tackle C.difficile Infections
advertisement

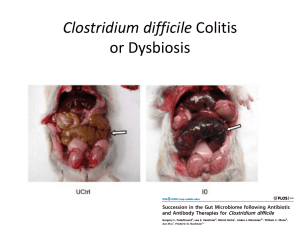
Using Root Cause Analysis to tackle C. difficile infections Dr. Tony Maggs Director of Infection Prevention & Control Torbay Hospital South Devon Health Care, NHS Foundation Trust Audio Conference Call October 13, 2010 www.macoalition.org Collaborative Updates Regional Workshops – Register Now! Antibiotic stewardship workgroup November 8th 8:30am-12:30pm at St. Luke’s Hospital, New Bedford, MA November 9th 8:30am-12:30pm at Western Massachusetts Hospital, Westfield, MA November 10th 1-5pm at Metro West Medical Center, Leonard Morse Campus, Natick MA 10 hospitals enrolled First call November 5, 1pm Space still available (froberts@macoalition.org) Team leader feedback email Our own PDSA: share your feedback and requests Using Root Cause Analysis to tackle C difficile infections…. Dr Tony Maggs, Director of Infection Prevention & Control - on behalf of the Infection Control Team and all the staff of Torbay Hospital 13th October 2010: Massachussets CDI Prevention Learning Collaborative South Devon Healthcare NHS Foundation Trust Local population of around 280,000 - 25% over 65 (national average 19%) Torbay District General hospital 3,773 staff (= 3,140 FTE) 450 beds (around 15% side rooms; ≈$150M backlog maintenance) In top 3 nationally for day case rates Average length of stay 3.6 days (down from 4.7 in 2004) Bed occupancy >85% ‘Managed through culture’ SDHFT hospital acquired C difficile infections 1.6 1.4 Rate per 1,000 bed days 1.2 1.0 0.8 0.68 / 1,000 bd 0.6 0.20 / 1,000 bd (70% reduction) 0.4 0.2 0.0 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 2004 2005 2006 2007 2008 2009 2010 How did we improve? Root Cause Analysis Environmental cleaning routine use of hypochlorite; greater frequency; dedicated cloths per bed space Antibiotic prescribing better guidelines; frequent audit and feedback; more education for junior docs Hand hygiene when and how (SPI 2) SDHFT hospital acquired C difficile infections 1.6 1.4 Rate per 1,000 bed days 1.2 Started RCA process 1.0 0.8 0.6 0.4 0.2 0.0 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 Qtr2 Qtr3 Qtr4 Qtr1 2004 2005 2006 2007 2008 2009 2010 Root cause analysis Started for hospital acquired cases in autumn 2007 Investigational team must include; a medical rep (consultant or junior doctor) a nursing rep an infection control rep - plus others as appropriate Aimed to be as flexible as possible during RCA no blame establish timeline: • “what do you want to celebrate and share?” • “what do you wish had never happened – and how would you avoid it next time around?” Root cause analysis Early learning - often a multitude of things going wrong - ‘shame / embarrassment‘ is a powerful driver for change! - talking about problems / sharing learning at clinical meetings → getting C difficile on clinical agenda Principal benefits More understanding about risk (“trigger questions”) C difficile is not an inevitable part of modern healthcare – it is an avoidable event Root cause analysis – clean safe care http://www.clean-safe-care.nhs.uk/ArticleFiles/Files/CDI_RCA_Tool_F%20.xls 2008 - tried the new tool • stifled discussion } • medics switched off • ‘closed’ analysis Very detailed / data driven (eg policy revision dates & compliance audits) -> formalise our processes • lay out RCA process • make local ownership more consistent • work up full list of trigger questions • incorporate ‘good bits’ into local tool • better control of action plans Root cause analysis Hospital acquired C difficile infection (10 days) Root Cause Analysis Review of standard practices (lead by matron) Action Plan Serious Adverse Event Group (signed off by associate director of nursing and clinical director) (for information) Healthcare Associated Infection Group (monitored by trust operational group charged with implementing annual Healthcare Associated Infection Action Plan) Speed is key…… • How quickly was diarrhoea flagged up? • How quickly was the patient isolated? • How quickly was the area cleaned? • How quickly was the sample collected? • How quickly was empirical treatment started? • How quickly were other treatments reviewed? • How quickly did the lab report the result? • How quickly was a positive test responded to? • How quickly was any failure to improve reacted to? Root cause analysis – selected trigger questions (1) • Was D&V assessment undertaken and documented within the medical notes on admission? • Has the patient had C difficile within the last 12 months? Was this reflected in the medical notes? • Was the patient weighed on admission? Evidence of malnutrition? • If the patient started antibiotics, was this in keeping with trust guidelines? Did the potential benefit of antibiotic treatment outweigh the potential risks? Root cause analysis – selected trigger questions (2) • When did the patient commence with diarrhoea and was it documented in the medical records? • Is there an assessment of diarrhoea severity in the medical notes (e.g. frequency, stool consistency, systemic upset including WCC, CRP etc)? • Was empirical treatment for C difficile given? • If not already happened, following the positive lab report, how quickly was C difficile treatment commenced? • How were other clinical teams on the ward made aware of this new diagnosis? Root cause analysis – selected trigger questions (3) • Was the side room cleaned twice daily with hypochlorite solution and was this recorded? • What method of hand hygiene was promoted? How? • Were doses of treatment ever missed, eg through patient refusal or medical condition? Is this reflected in the medical notes? South Devon Healthcare NHS Foundation Trust Internal target of zero clusters of C difficile National target in 2009/10 of <= 70 cases Actual number 27 cases (8 possible clusters - doubtful) → better care for patients; better life for staff In nearly half of all months, we only have one hospital acquired C difficile case → everything becomes more manageable