RISK OF RECURRENCE OF CLOSTRIDIUM
DIFFICILE INFECTION WITH PPI USE
Nilofar Rahman, MD
CLOSTRIDIUM DIFFICILE ORGANISM
Identified in 1978
“J strain”
B1/NAP1/027 strain
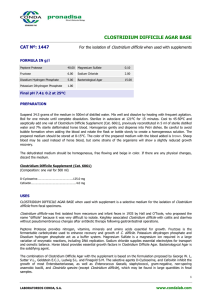
INCIDENT RATES IF C. DIFF. INFECTION
EPIDEMIOLOGY OF C. DIFF INFECTION
RISK FACTORS FOR RECURRENCE OF CDI
Advanced age
Non- CDI targeted antibiotic exposure
Longer hospital stay
Inadequate antitoxin-antibody response
Concomitant use of PPIs
STUDY DONE BY LINSKY ET AL.
STUDY DESIGN
1549 Incident c. diff toxin
1408 treated with oral metronidazole or
vancomycin
1166 treated within 3 d before or after
index CDI
527 PPI exposure
639 no PPI exposure
Study population
PRIMARY EXPOSURE AND OUTCOMES
Exposure measure: PPI within 14 days
Outcome measure: C. diff toxin in 15-90 after incident CDI
Covariates:
Age, sex
Comorbid conditions
CDI- targeted antibiotic
Non-CDI targeted antibiotic
RESULTS
RESULTS CONTD..
Model
Hazard ratio(95% CI)
P value
Unadjusted
1.42(1.11-1.82)
0.006
Adjusted
1.42(1.10-1.83)
0.008
Non-CDI antibiotic
exposure
1.71(1.11-2.64)
0.01
No antibiotic
exposure
1.30(0.94-1.79)
0.12
Study done by Kim et al.
EXPOSURE VARIABLE AND STUDY DESIGN
Exposure variable: PPI use 3D prior to CDI
Study design
Recurrent group
Non-recurrent
group
RESULTS
UNIVARIATE ANALYSIS
Age > 65 (60%, P=0.02)
Fed via NGT (48.1%, P=0.04)
Low albumin ( 2.3+/- 0.5g/dl vs. 3.1 +/- 0.4g/dl)
PPI use (63% vs 39.8%, P=0.01)
MULTIVARIATE ANALYSIS
RISK FACTORS
ADJUSTED ODDS CI (95%)
RATIO
P VALUE
Age>65
1.32
1.12-3.87
0.03
Concurrent PPI use 1.85
1.35-4.91
0.028
Serum
albumin<2.5g/dl
3.48
1.64-7.69
0.016
NGT
1.25
0.91-2.65
0.068
Since use of PPIs is a modifiable risk factor for recurrence it is
appropriate to review, constantly, the use of PPIs in patients with
CDI.
THANK YOU
REFERENCES
1. Mylonakis E, Ryan ET, Calderwood SB. Clostridium difficile--Associated diarrhea: A review. Arch Intern Med.
2001;161:525–533.
2. Leffler DA, Lamont JT. Treatment of Clostridium difficile-associated disease. Gastroenterology. 2009;136:1899–1912.
3. Maroo S, Lamont JT. Recurrent clostridium difficile. Gastroenterology. 2006; 130:1311–1316.
4. Do AN, Fridkin SK, Yechouron A, Banerjee SN, Killgore GE, Bourgault AM, Jolivet M, Jarvis WR. Risk factors for
early recurrent Clostridium difficile-associated diarrhea. Clin Infect Dis. 1998;26:954–959.
5. Lowenkron SE, Waxner J, Khullar P, Ilowite JS, Niederman MS, Fein AM. Clostridium difficile infection as a cause of
severe sepsis. Intensive Care Med. 1996;22:990–994.
6. Pron B, Merckx J, Touzet P, Ferroni A, Poyart C, Berche P, Gaillard JL. Chronic septic arthritis and osteomyelitis in a
prosthetic knee joint due to Clostridium difficile. Eur J Clin Microbiol Infect Dis. 1995; 14:599–601.
7. Fekety R, McFarland LV, Surawicz CM, Greenberg RN, Elmer GW, Mulligan ME. Recurrent Clostridium difficile
diarrhea: characteristics of and risk factors for patients enrolled in a prospective, randomized, double -blinded trial. Clin
Infect Dis. 1997;24:324–333.
8. McFarland LV, Surawicz CM, Rubin M, Fekety R, Elmer GW, Greenberg RN. Recurrent Clostridium difficile disease:
epidemiology and clinical characteristics. Infect Control Hosp Epidemiol. 1999; 20:43–50.
9. Cunningham R, Dale B, Undy B, Gaunt N. Proton pump inhibitors as a risk factor for Clostridium difficile diarrhoea. J
Hosp Infect. 2003;54:243–245.
10. Yearsley KA, Gilby LJ, Ramadas AV, Kubiak EM, Fone DL, Allison MC. Proton pump inhibitor therapy is a risk
factor for Clostridium difficile-associated diarrhoea. Aliment Pharmacol Ther. 2006;24:613–619.
11. Cadle RM, Mansouri MD, Logan N, Kudva DR, Musher DM. Association of proton -pump inhibitors with outcomes in
Clostridium difficile colitis. Am J Health Syst Pharm. 2007; 64:2359–2363.