Infectious Disease Update
Christopher Belcher MD FAAP
Director, Pediatric Infectious Diseases
Peyton Manning Children’s Hospital
Indianapolis, IN
Case #1
• 2 yo girl previously healthy
• Presented to ER with fever
• Found leukopenia / neutropenia and
thrombocytopenia
• Moderately ill, no rash, no HSM
• A piece of historical information led to the
diagnostic test.
Case #1
Case #1 – P. falciparum Malaria
•
•
•
•
•
Family had spent a month in Nigeria
Claim to have taken antimalarials
Parasite burden initially above 3%
Was treated with atovaquone / proguanil
Received treatment in hospital – defervesced,
showed count recovery, and clearance of
parasitemia
CLOSTRIDIUM DIFFICILE COLITIS
Clostridium difficile
• Presentation:
– Often fever, abd pain, diarrhea - bloody, mucousy
– Associated with antibiotic use, abd surgery
• Has been held children under 2 do not have the
receptor for the toxin
– Issue being re-examined
• Outcomes
– Morbidity - diarrhea, fever, prolonged hospital stay
– Toxic megacolon / colectomy
Background: Impact
• Hospital-acquired, hospital-onset:
165,000 cases, $1.3 billion in
excess costs, and 9,000 deaths
annually
• Hospital-acquired, post-discharge
(up to 4 weeks): 50,000 cases,
$0.3 billion in excess costs, and
3,000 deaths annually
• Nursing home-onset: 263,000
cases, $2.2 billion in excess costs,
and 16,500 deaths annually
Campbell et al. Infect Control Hosp Epidemiol. 2009:30:523-33.
Dubberke et al. Emerg Infect Dis. 2008;14:1031-8.
Dubberke et al. Clin Infect Dis. 2008;46:497-504.
Elixhauser et al. HCUP Statistical Brief #50. 2008.
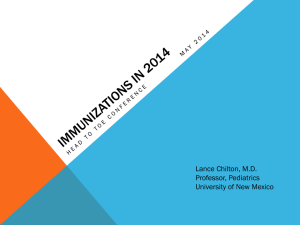
From: Clostridium difficile Infection in Hospitalized Children in the United States
Arch Pediatr Adolesc Med. 2011;165(5):451-457. doi:10.1001/archpediatrics.2010.282
Figure Legend:
Trend in Clostridium difficile infection (CDI) in hospitalized children.
Date of download: 9/4/2012
Copyright © 2012 American Medical
Association. All rights reserved.
Clostridium difficile
• Since 2005 an increase in resistant, aggressive
C. difficile colitis (NAP-1)
• Associated with fluoroquinolone resistance
and increased toxin production
• Incidence 22.5 vs 6 per 1000 admissions in
2004 vs 1997
• 30-day attributable mortality rate was 6.9% vs.
1.5% in 1997
N Engl J Med 2005;353:2433-2449,2503-2505.
Risks Factors for Disease
• Antibiotics put patients at risk
– Adults : fluoroquinolones
– Children : penicillins and cephalosporins
• Clindamycin resistant strain “J” was more
prevalent in 1990s
• Risks in children include: cancer and IBD
Findings of Children Discharged with C.
difficile from pediatric hospitals
•
•
•
•
•
•
Increasing trend from 1997 - 2006
20% higher mortality rate
36% more likely to have had a colectomy
Increased LOS 4x, charges 2x
11 times more likely to have IBD
More likely to be on immunosuppression or
antibiotics
• UNLIKE adults, no increase in severity
Arch Ped Adolesc Med 2011; 165: 451-7
What to do with Infants
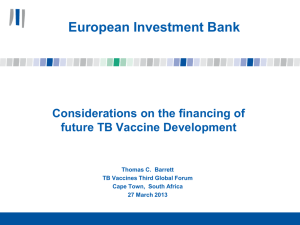
• C. difficile can be a part of the normal flora in
newborns and young infants
• 70% can be colonized and asymptomatic
• The environment, not maternal transmission
seems to be the major factor
• After 2 years of age, the gut flora should
mimic an adult and it is not normal
J
.
C
C. difficile Colonization by Age Up to 13 Years of Age
David A. Enoch , Matthew J. Butler , Sumita Pai , Sani H. Aliyu , J. Andreas Karas Clostridium difficile in children: Colonisation and disease
Journal of Infection Volume 63, Issue 2 2011 105 - 113
Testing for C. difficile
• C difficile culture
• C difficile toxin detection: EIA, mouse IP
• C difficile molecular methods (PCR)
– 027/Nap1/BI
• In a study of 5 testing methods – molecular
methods detected 35-54% more positive
specimens
• Only need to order PCR once - ONCE
Chapin KC. J Mol Diagn. 2011; 13:395-400
Clostridium difficile Prevention and
Treatment
• Prevention
– Good hygiene
– C. difficile spores NOT killed by alcohol
– Limit antibiotic use
• Treatment
–
–
–
–
–
–
–
STOP the antibiotics
Metronidazole
Oral vancomycin
Fidaxomicin
Nitazoxanide (Alinia)
Under study: ramoplanin, CB-183315
Others: po bacitracin, tinidazole, IVIG, cholestyramine,
probiotics, fecal enemas
Metronidazole Therapy
• Can be given iv or po
• 30 mg/kg/day divided q 6 hours x 10 days
– Maximum 2gm/day
• 20% or more may relapse after therapy
Vancomycin Therapy
• Only given po for C. difficile
– Can use capsules (125mg, 250 mg)
– or IV solution orally
• IV vancomycin does not enter gut
• 40 mg/kg/day po divided into 4 doses
– Maximum 500mg/dose
• The best way to create VRE
– Vancomycin resistant enterococci
Fidaxomicin
•
•
•
•
•
•
Narrow spectrum macrocyclic antibiotic
ONLY approved in adults
200mg twice a day for 10 days
No more effective than vancomycin
Lower relapse rate
Orphan drug status for children under 16
Probiotic Therapy
• 138 hospitalized adults received probiotics or
placebo
(Plummer S, et al. Clostridium difficile pilot… Int Microbiol . 2004;7:59-62)
– Of those with diarrhea:
• 2.9% of probiotic group were C. diff positive
• 7.2% of placebo group were C. diff positive
• The relapse rate of adults with recurrent C. diff was
lower when given probiotics
(McFarland LV, et al. A randomized placebo-controlled… JAMA .
1994;271:1913-1918)
• Metaanalysis shows benefit for AAD and C. diff with
S. boulardii and L. rhamnosus
(Am J Gastroenterol 2006;101:812-822)
• But data are still mixed and no clear recommendation can be
made
The Potential for Vaccines
• Approaches to Vaccines:
– Toxoid Vaccine to toxin A and B
•
•
•
•
Similar to other toxoid vaccines – tetanus, diphtheria
Delivered IM
Do produce antibody responses
Further in development cycle
– Recombinant subunit vaccines
• Truncated toxin A and B
• Newer in development cycle
(Aboudola et al., 2003; Kotloff et al., 2001; Intercell , 2011).
http://www.discoverymedicine.com/Dale-N-Gerding/2012/01/25/clostridium-difficile-infection-prevention-biotherapeutics-immunologics-and-vaccines/
Case #2
•
•
•
•
15 year old boy, previously well
Developed red scaly lesions L clavicle and arm
No relief with hydrocortisone
Sent to dermatology for psoriasis
Case #2
Case #2
• Biopsy of the lesion revealed:
– Blastomyces
• We live in the land of Histoplasma
• Treated with Itraconazole
VACCINE SAFETY
Vaccine Safety
• CDC email study of 476 families
• Concerns included:
– 38% - too many shots in one visit
– 34% - too many vaccines in 2 years
– 32% - vaccines may cause fever
– 30% - vaccines may cause autism / neurol
– 26% - vaccine ingredients are unsafe
– 23% - no safety concerns
Health Aff. 2011; 30:61151-9
Vaccine Safety - Who Do Parents Trust
• 1500 parents online national survey
– 76% said they trust their doctor "a lot”
– 26% said they trust other HCP "a lot"
– 23% said they trust government experts "a lot"
Pediatrics 2011; 127:S107-12
Vaccine Safety - Who Do Parents Trust
• Family and friends 67% reported as
"somewhat trustworthy"
• Parents of children harmed by vaccines 65%
reported as "somewhat trustworthy"
• Celebrities "somewhat trustworthy" by 24%
• Mothers more likely than fathers to report
influence by parents of children harmed by
vaccines, media, celebrities
Vaccine Safety
• Institute of Medicine - literature review
• Vaccines: MMR, VAR, HepA, HepB, HPV, MCV,
DTaP
– NO association of MMR vaccine with autism based
on scientific literature
– NO association of Type I diabetes with MMR or
DTaP
– NO association of asthma, RAD, Bell's palsy with
TIV
Institute of Medicine http://www.iom.edu/Reports/2011/
Adverse-Effects-of-Vaccines-Evidence-and-Causality/Report-Brief.aspx
Vaccine Safety
• The report did find convincing evidence for:
– Var association with disseminated varicella and
with zoster
– MMR vaccine and febrile seizures as well as
measles inclusion body encephalitis
– Hypersensitivity with: MMR, Var, TIV, HepB, MCV,
TT
Vaccine Safety
• The report did find evidence that favored
acceptance for:
– HPV and anaphylaxis
– MMR and transient arthralgia in females and
children
• Most other associations - the evidence was
inadequate to accept or reject
Vaccine Safety - What to Do
• US Dept of Health and Human Services Study
• 272 new mothers
– Given written vaccine safety info and VIS
– One of 3 groups: prenatal, 1 wk, 2mo
• All groups improved attitude
• Preferred info before 2 month visit
Pediatrics 2011; 127:S120-6
Vaccine Safety - What to Do
• Know what parents are reading and talking
about
• Listen to parental concerns
• Dispel myths and misunderstandings with
information
• Top down your office MUST believe in
vaccination and BE vaccinated
Case #3
•
•
•
•
10 day old infant
Delivered by NSVD
Clinically well
Developed a rash
Case #3
Case #3
• At this point the correct thing to do is:
– Obtain HSV swabs and start acyclovir
– Obtain a culture and apply mupirocin
– Obtain a dermatology consult
• The diagnosis was confirmed as:
– Incontinentia pigmenti
MISCELLANEOUS INFLUENZA
UPDATES
2012-13 Influenza Vaccine
Composition
• A/California/7/2009 (H1N1)
• A/Victoria/361/2011 (H3N2)
• B/Wisconsin/1/2010
How to Deal with Egg Allergy
MMWR Weekly August 17, 2012 / 61(32);613-618
2012-13 Vaccine for Children <9
MMWR Weekly August 17, 2012 / 61(32);613-618
Quadrivalent Influenza Vaccine
• Traditional influenza vaccine is trivalent –
containing 2 A strains and one B strain
• B strains are usually one of two lineages –
Victoria and Yamagata
• In the first 10 flu seasons this millennium the
lineage in the vaccine did not match what
circulated HALF the time!
• Thus, putting in two B strains is an attractive
strategy for future seasons 2013-14
www.cdc.gov/flu/weekly/
H3N2v Influenza
• Most symptomatic cases are typical of
seasonal influenza
• No evidence of sustained human to human
transmission
• All isolates contain M gene of 2009 H1N1
strain that increases human transmission
• Concern when exposed to pigs (not eating
pork)
• Our PCR detects as unclassified Influenza
Case Count: Detected U.S. Human Infections with
H3N2v by State since August 2011
States Reporting H3N2v
Hawaii
Illinois
Indiana
Iowa
Maine
Maryland
Michigan
Minnesota
Ohio
Pennsylvania
Utah
West Virginia
Wisconsin
Total
Cases in 2011
2
3
2
3
2
12
Cases in 2012
1
4
138
12
6
4
107
11
1*
3
20
307
http://www.cdc.gov/flu/swineflu/h3n2v-case-count.htm#table1
Case Count: Detected U.S. Human Infections with
H3N2v by State since August 2011
States Reporting H3N2v
Hawaii
Illinois
Indiana
Iowa
Maine
Maryland
Michigan
Minnesota
Ohio
Pennsylvania
Utah
West Virginia
Wisconsin
Total
Cases in 2011
2
3
2
3
2
12
Cases in 2012
1
4
138
12
6
4
107
11
1*
3
20
307
http://www.cdc.gov/flu/swineflu/h3n2v-case-count.htm#table1
Case #4
• A thirteen year old girl previously well
• Developed moderately painful nodules on her
palms
• No systemic symptoms
Case #4
Case #4
• Diagnostic considerations include:
– Syphilis
– Papular purpuric gloves and socks syndrome
– Non tuberculous mycobacterium
– Enterovirus 71
Case #4
• Diagnostic considerations include:
– Syphilis
– Papular purpuric gloves and socks syndrome
– Non tuberculous mycobacterium
– Enterovirus 71
Case #4
ID MISCELLANY
PMCH ER E. coli Urine Sensitivities
Antibiotic
Susceptible
Intermediate
Resistant
AMPICILLIN
80
0
82
51%
31
19%
AMPICILLIN/SULBACTAM
CEFAZOLIN
CEFTRIAXONE NON CSF
CIPROFLOXACIN
GENTAMICIN
NITROFURANTOIN
TRIMETHSULFAMETHOXAZOLE
49%
0%
112
69%
19
12%
154
95%
3
2%
5
3%
162
100%
0
0%
0
0%
155
96%
0
0%
7
4%
153
94%
0
0%
9
6%
158
98%
3
2%
1
1%
119
73%
0
0%
43
27%
Tuberculosis Testing in Children
• Mantoux skin test is the gold standard
– 15mm is positive for most over 4 years old
– 10mm if they have risk factors (<4 yo, overseas,
contact with high risk, medical conditions)
– 5mm if they are very high risk (household contact, dz,
suppressed)
• Interferon gamma release assays
–
–
–
–
Quantiferon TB or T-SPOT
Only require single visit for blood draw
No false positives with BCG
Unreliable under 5 years old
DTaP Vaccine Administration Site
•
•
•
•
Study of over 230,000 patients
5th dose DTaP (age 4-6)
75% given in the arm
0.4% of children had medically attended local
reaction
• 47.4 vs 32.1 (arm to leg) reactions / 10,000
• Thus, the leg may be an attractive site.
Jackson LA et al. Pediatrics. 2011;127:e581-5876
Rabies Prevention
• Virus transmitted in saliva of infected animal
– Bats are most common source in IN
– Tiny teeth and claws
– Exposure considered if bat contact cannot be ruled out in
room of sleeping or your individual
– ***DON’T let them kill the animal***
• PEP involves:
– wound cleaning
– rabies immune globulin 20 IU/kg around wound / IM
– vaccine - 1ml IM on days 0, 3, 7, 14
• 2009 changed recommendation for PEP vaccine from 5
doses to 4 (got rid of day 28)
Pneumococcal Disease in 2011
• Had been seeing 140-180 cases of vaccine
preventable invasive pneumococcal disease /
year
• In 2011 was down to 40
• Likely due to introduction and boosters with
PCV13
• Drug resistant S. pneumoniae was not seen at
PMCH in 2011
Pneumococcal Meningitis
Meant to Gross You Out
• Hospital Curtains (Schweizer, ICAAC 2011)
– 42% of curtains had VRE
– 21% had MRSA
– 92% were colonized with a pathogen in 1 week
• Ties and lab coats are nasty too!
Case #5
•
•
•
•
•
6 year old boy
Had 1 week of fever, cough
Presented with Hb 2.6 Hct 7.8 WBC 1.8
Required transfusion in PICU
Found to have a warm reactive antibody
Case #5
• Testing was postive for:
– Influenza
– Adenovirus
– Mycoplasma pneumoniae
– Parvovirus B19
Case #5
• Testing was postive for:
– Influenza
– Adenovirus
– Mycoplasma pneumoniae
– Parvovirus B19
Case #5
Infectious Disease Update
Christopher Belcher MD FAAP
Director, Pediatric Infectious Diseases
Peyton Manning Children’s Hospital
Indianapolis, IN