N.Gonorrhoae
بنام خداوند بخشندهٌ مهربان
Neisseria
gonorrhoeae
Department of Medical Microbiology
N.Gonorrhoae
سومین بیماری مقاربتی( )STDدر آمریکا و در ایران ؟
فیزیولوژی – مورفولوژی.
سلولهای باکتری نشبتآ کوجک µ 2-1و بشکل دیپلوکوکسی.
کلنیهای آن برروی محیطهای کشت شکالت آگار،تایرمارتین و
مارتین لویس آگار در ابتدا شفاف،کوچک و حدود1میلیمتراست.
اسیدهای چرب و یونهای فلزی ازرشد باکتری ممانعت می کنند.
N.Gonorrhoae
ادام ٌه فیزیولوژی
باکتری بشدت به خشکی،نوروبی غذائی (خارج از بدن)حساس
بوده،برای رشددرمحیط کشت نیاز به آتمسفری از co2%5دارد
تیپ کلنیهای باکتری از T5 – T1می باشد.
تیپهای T1و T2ویروالن بوده بقیه غیر ویروالن هستند.
برای تعیین هویت باکتری بایستی مورفولوژی کلنی ها در محیط
کشت-داشتن سیتوکروم اکسیدازوتجزی ٌه اکسیداتیو گلوکوزو...
بررسی الکتروفورتیک آنزیمهای هگزوکیناز
N.Gonorrhoae
ساختــار سلولی
اندوتوکسین آن شباهت زیادی به اندوتوکسین مننگوکک دارد.
حاوی lipidAو coreپلی ساکاریدی است ولی o side
chainندارند.
در اینجا نیز همانند مننگوکک اندوتوکسین باکتری به فضای(آب)
میان بافتی ترشح( )releaseمی شود.
LOSباکتری می تواند دراتصال به سطح سلولهای اپی تلیال با
پیلی همکاری کند.
N.Gonorrhoae
ادام ٌه ساختــار سلولی
(Pilusجمع )piliباکتری اتصال اصلی گونوکک به سلولهای اپی تلیال را
تآمین ) )columnarEpt.cell not Squamous cellsمی کند.
باید یادآور شد که باکتری می تواند در سلولهای مربوط به گلو و رکتوم نیز
کلونیزه شود.
این اتصال مي بایست مستحكم شده و با سطح سلولهاي اپیتلیال سازگار
شود.
بخش N-Terminalپروتئین pilinثابت و محكم()conserveوبخش
C-Terminalآن متغیر()Variableاست.
باكتریها براساس داشتن و نداشتن piliمتحمل phase variationمي
شوند .
N.Gonorrhoae
تغییرات فازیك
Pili درپاساژهاي متعدد از بین مي رود p- ---p+:ویا fim- ---- fim+
اما در تغییرات آنتي ژنیك ژن كد كنندهٌ پروتئین PilEكه پروتئین اصلي پیلي
است،دستخوش تغییراتي در سكانس خود مي شود .وبا ژن PilSایجاد نوتركیبي مي كند.
گفته مي شود تا 1000واریانت ممكن است بوجود بیاید.
تغییرات در بیان شدن پیلي در طي عفونت به این ترتیب است كه:
در پیشابراه مردان 17.5كیلو دالتون است.
در مجراي ادراري اولین زن سالمي كه مرد آلوده با او تماس مي گیرد19-18.5
كیلودالتون ،ودر Cervixعدد وزن ملكولي پیلي به 17كیلودالتون تقلیل مي یابد.
در Cervixدومین زن تماس گرفته شده این عدد به 18.3كیلو دالتون خواهد رسید.
S= Silent
E= Effective
N.Gonorrhoae
ادام ٌه پیلي
%20پیلي دستخوش تغییر مي گردد.
بدلیل تغییرات در بخش پیلي است كه تا بحال واكسن مطمئني وجود ندارد.
بعضي از محققین معتقدندپیلي فقط جهت اتصال نیست بلكه باعث نوعي
حركت براي باكتري مي شود. twitching motility:
PilAبخش اصلي پیلین است،بخش انتهائي را PilCتشكیل مي دهد.
PilQحالت ترشح شونده داردتا PilAاز OMبگذرد.
PilTنقش نوعي ATPaseرا بازي مي كند(.)Retraction motor
نقش موتور انقباضي(،)PilTمنقبض ،منبسط كردن PilAاست
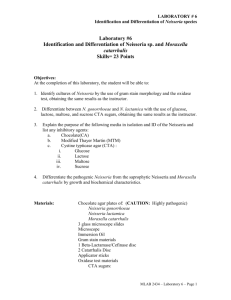
Speculative model of type IV pili. The major pilin (PilA) is the
structural subunit. The tip adhesin in Neisseria is PilC (labelled here
as C1/Y1).
NB Anchored in the
Inner Membrane
PilQ a secretin for
PilA to cross the OM
& is a pore protein
PilT an ATPase
Retraction ‘motor’
PilA collapses into the
OM & IM (retraction)
N.Gonorrhoae
پروتئین هاي OM
پروتئین Iیا ، porIپروتئین اصلي( OM )Majorاست كه به عنوان یك
porinعمل كرده،اجازه مي دهد بعضي مواد diffuseشوندوبراي زنده
ماندن داخل فاگوسیتها ضروري است.
پروتئین IIیا ) ) opaیك minorپروتئین است،كه در اتصال به PMNs
شركت كرده در endocytosisدخالت مي كند:این پروتئین نیز دستخوش
تغییرات مي شود.
پروتئین )rmp(IIIدر تجمع با porIبراي باكتري poreها را مي سازند.
گفته شده است این پروتئین باعث بلوكه شدن اثر باكتریسیدال سرم(توسط
)IgGمي شود ،یعني نوعي عمل Blocking Abانجام مي دهد.
N.Gonorrhoae
باقیماندهٌ ویروالنس فاكتورها
یكي دیگر از ویروالنس فاكتورهاي مهم باكتري IgA1است كه باعث شكسته شدنIgA
مخاطي مي شود.
توانا ئي جذب آهن سرم (توسط سیدروفورخاصي كه باكتري در جریان خون میسازد).
پاتوژنز
اتصال با piliو opaو حمل ٌه باكتري
شبیه نمائي با ساختارهاي میزبان ( ) Molecular Mimicry
آزاد شدن ملكولها و تركیبات سیستم ایمني(سلولي و هومورال)وآزاد شدن membrane
blebs:enhance endotoxic mediated toxicity and protect
. replicating bacteria by binding protein-directed Ab.
ممانعت از فعالیت PMNsوفعال شدن كمپلمان از طریق آلترناتیو
ایجاد انفالماسیون،فعال شدن TNFها و دیگر اینترلوكین ها Inflammationنهائي
وایجاد عالئم.
Neisseria gonorrhoeae
Spread and multiplication
Once attach to non-ciliated cells, multiply
rapidly and spread up urethra (male) or
through cervix (female)
Are not motile; aided external mechanisms
Eddy current in mucus
Attached to spermatozoa
Protected from IgA by IgA protease
Neisseria gonorrhoeae
Spread and multiplication
Invasion
Once attach, microvilli extend and embrace
organisms
Internalized by endocytosis into “nonprofessional
phagocytes” and transported in cell by
phagocytic vesicles
Neisseria gonorrhoeae
Spread and multiplication
Invasion
After internalization, transported to base of non-
ciliated cells
Vacuoles fuse with basement membrane and
discharge contents into subepithelial connective tissue
Either cause local damage or enter blood vessels and
cause disseminated disease
Neisseria gonorrhoeae
Survival in bloodstream
Most strains killed by antibodies
Target surface proteins and LOS
Resistant strains cause disseminated
disease
Distinguising characteristics
More sensitive to penicillin
Have specific nutritional requirements
Attachment sialic acid to CHO portion LOS; blocks
complement of activation and binding to other surface
proteins
Neisseria gonorrhoeae
Pathogenesis
Process
Introduced into vagina or urethral mucosa of
penis—attach to surface of epithelial cells and
multiply
Attach to unidentified specific receptors by pili (also
prevent phagocytosis)
Protein II—once cells brought close enough by pili,
adherence to cell occurs (also called OPA)
Neisseria gonorrhoeae
Damage
Ciliated cells—done by endotoxin and
fragments of murein (muramyl monomers,
same as Bordetella pertussis)
Studied most in fallopian organ culture
Ciliary mechanism important for transporting egg
from ovary to uterus and for clearing bacteria
from mucosal surface
After damage, fallopian tube susceptible to bacteria
from vaginal flora that ascend through the cervix and
uterus
Neisseria gonorrhoeae
Damage
Submucosal connective tissue, due to
inflammatory response
Male urethra—leads to local symptoms (pain on
urination and pus discharge)
Other diseases cause by other pathogens have some
of the same symptoms
Pain is more intense and urethral discharge is more
copious, thicker, and greenish-yellow
Neisseria gonorrhoeae
Outcome of infection
Males—symptoms usually subside in
several weeks, even without treatment
Repeated infections, in untreated, can lead to
scarring and stricture of urethra
Relatively unusual, because males usually seek
treatment
Neisseria gonorrhoeae
Outcome of infection
Females—local urogenital infection
frequently asymptomatic
Complications yield symptoms
Sequellae of fallopian tube damage
Ectopic pregnancy, recurrent PID by other organisms,
chronic pelvic pain, and infertility due to blockage or
damage to tubes
Can lead to death of woman and her unborn
child
Neisseria gonorrhoeae
Prompt treatment for either gender
decreases chances of disseminated
disease
Epidemiology: sexual transmission
Males—20% after intercourse
Females—50% after intercourse
Neisseria gonorrhoeae
Diagnosis
Gram— intracellular diplococci in vaginal,
cervical, or urethral specimens is
suggestive; start antibiotic therapy
Important to culture for confirmation
Biochemical tests
Oxidase+
Oxidize glucose, not maltose nor sucrose
Neisseria gonorrhoeae
Treatment
Used to be massive doses of penicillin
Now: If -lactamase resistant (plasmid;
same as Haemophilus influenzae);
cephalosporin, cefriaxone-IM
Resistance to penicillin, tetracycline,
aminoglycosides (chromosomal; change in
cell surface)—susceptibility test
Single dose oral therapy
Neisseria gonorrhoeae
Treatment
Single dose oral therapy: ciprofloxacin;
cifixime
Resistance increasing
If complicated by Chlamydia: doxycycline;
azithromycin
Studying Disease and
Development of Vaccine
Phase variation:
Expression of Ag
Antigenic variation:
Expression of different copies
High frequency processes