GERD - Gastroesophageal Reflux Disease
advertisement

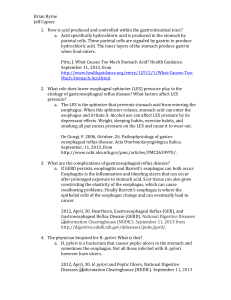
Gastroesophageal Reflux Disease Prof. Faisal Ghani Siddiqui FCPS; PGDip-bioethics; MCPS-HPE faisal@lumhs.edu.pk www.lumhs.edu.pk/faculties/surgery/gsurgery/faculty PREAMBLE • What is GERD? • LES? • What causes GERD? • How does GERD present? • What are its complications? INTRODUCTION What is GERD? Condition characterized by heartburn and regurgitation due to the loss of the HPZ GERD • Common; Accounts for majority of esophageal pathologies • Chronic disease; needs life-long medical treatment • Surgery is effective; provides longterm relief PATHOPHYSIOLOGY of gastroesophageal Reflux Disease • HPZ located at the EG junction • No distinct anatomical sphincter • 3-4 cms long • 10-25 mmHg • Relaxes during swallowing / belching Resting LES pressure Overall length of the sphincter Intraabdominal length of the sphincter Resting LES pressure Overall length of the sphincter Intraabdominal length of the sphincter LARGE MEALS REPEATED STOMACH DISTENSION SHORTENING OF LES INCOMPETENT SPHINCTER REFLUX Resting LES pressure Overall length of the sphincter Intraabdominal length of the sphincter Permanently Defective LES • Mean resting pressure < 6mm • Overall length < 2cm • Intra-abdominal length < 1 cm ACID / PEPSIN /DUODENAL CONTENTS EXPOSURE ESOPHAGITIS BE STRICTURE SYMPTOMS of Gastroesophageal Reflux Disease • Heartburn • Regurgitation • Dysphagia • Chest pain COMPLICATIONS of Gastroesophageal Reflux Disease REPEATITIVE ESOPHAGEAL INJURY MUCOSAL & INTRAMURAL FIBROSIS STRICTURE REPLACEMENT OF SQ. EPITHELIUM WITH COLUMNER EPITHELIUM BARRETT’S ESOPHAGUS Squamous epithelium replaced by columnar epithelium Norman Barrett 1950 Barrett’s Esophagus Endoscopically identified columnar mucosa, which on biopsy shows intestinal mucosa with goblet cells COMPLICATIONS OF BARRETT’S ESOPHAGUS ULCERATION STRICTURE CARCINOMA DYSPLASIA METAPLASIA DYSPLASIA ADENOCARCINOMA MANAGEMENT of Gastroesophageal Reflux Disease Management of GERD CONSERVATIVE TREATMENT INVESTIGATIONS SURGERY Management of GERD CONSERVATIVE TREATMENT INVESTIGATIONS SURGERY CONSERVATIVE TREATMENT • Antacids • Alginic acid • Metoclopromide / domperidone • Proton pump inhibitors • Change in life style Change in Life-style • Elevate head of the bed • Avoid tight fitting clothes • Eat small, frequent meals • Avoid eating before bedtime • Dietary changes PPI’s suppress acidity & relieve symptoms but do not control reflux Control of reflux better than control of symptoms! Antireflux surgery eliminates reflux! Management of GERD CONSERVATIVE TREATMENT INVESTIGATIONS SURGERY INVESTIGATE IF SYMPTOMS… • Persist or progress • Recur INVESTIGATIONS • Endoscopy • 24-hour pH monitoring • Manometry Management of GERD CONSERVATIVE TREATMENT INVESTIGATIONS SURGERY WHEN TO OPERATE? • Persistent or progressive disease • Young patients with documented reflux • Stricture • Barrett’s esophagitis GOAL OF SURGERY to restore normal structure/pressure of the LES while preserving patient’s ability to swallow, and to belch PRINCIPLES • Restore pressure (>12 mmHg) • Restore length (at least 3 cm) • Place adequate length in abdomen (1.5 – 2 cm) ANTIREFLUX PROCEDURES • Nissen fundoplication • Toupet partial fundoplication • Belsey Mark IV partial fundoplication COMPLICATIONS • Temporary dysphagia • Inability to vomit • Increased flatulence