Neonatal Candidiasis
advertisement

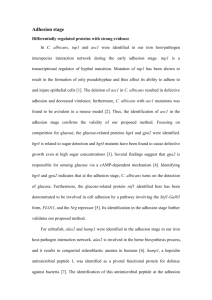
Neonatal Candidiasis Catherine M. Bendel, M.D. University of Minnesota Medical School, Minneapolis Neonatal Candidiasis Outline Epidemiology Risk Factors -- Yeast and Host Research correlates Clinical Presentation Diagnosis and Treatment Prophylaxis? Candida Commensal organism Eucaryotic and diploid (C. albicans) Dimorphic yeast Increasingly important nosocomial pathogen Nosocomial Candidiasis 6th most common nosocomial pathogen 4th most common cause of nosocomial septicemia (7.8% of all bloodstream infections) 2nd most common nosocomial pathogen in NICU - incidence 2-20% in ELBW 24% to 54% mortality in those who receive therapy High morbidity Pfaller. Clin Infect Dis 1996;22(Suppl 2):S89 Pittet & Wenzel. Arch Intern Med 1995;155:1177 Baltimore. Sem in Perinat 1998;22: 25 Benjamin. Pediatrics 2000;106:712 Numbers of Cases of Sepsis in the United States, According to the Causative Organism, 19792000. Martin GL et al, N Engl J Med 348:1546-54, 2003 Virulence Factors C. albicans accounts for the majority of Candida spp isolated Multiple intrinsic C. albicans virulence factors have been identified Systemic infections associated with specific host risk factors The gastrointestinal tract is considered a major portal of entry for C. albicans Frequency of Isolation of Candida species All patients 55% C. albicans 20% C. glabrata 9% C. tropicalis 7% C. krusei 15% C. parapsilosis 1% C. dubliniensis 2% others Neonates 58% C. albicans 34% C. parapsilosis 2% C. glabrata 4% C. tropicalis 2% others Phaller, J Clin Micro 2001:39 Fridkin, Pediatrics, 2006:117 Virulence Factors C. albicans accounts for the majority of Candida spp isolated Multiple intrinsic C. albicans virulence factors have been identified Systemic infections associated with specific host risk factors The gastrointestinal tract is considered a major portal of entry for C. albicans C. albicans virulence factors Adherence to host tissues (epithelium/endothelium) Receptor or adhesin mediated Cytolytic enzymes (proteinases, phospholipases) Hydrophobicity Variable phenotypic expression Morphologic switching Filamentous forms believed to facilitate adhesion and penetration of epithelium Andrutis. J Clin Microbiol 2000; 38: 2317 Cutler. Ann Rev Microbiol 1991;45:187 Mitchell. Curr Opin Microbiol 1998; 1:687 Gale. Science 1998;279:1355 Corner. Curr Biol 1997; 7:R761 Calcofluor stained cecal contents from a mouse colonized with C. albicans showing yeast and filamentous forms in vivo C. albicans CAG1 (+/-) incubated 3 h on Caco-2 enterocytes showing yeast cluster partially embedded C. albicans CAF2 (+/+) incubated 3 h on Caco-2 enterocytes with microvilli intimately associated with distal tip of germtube C. albicans CAF2 (+/+) incubated 3 h on Caco-2 enterocytes showing elongated enterocyte microvilli anchoring a C. albicans filament to the enterocyte surface Virulence Factors C. albicans accounts for the majority of Candida spp isolated Multiple intrinsic C. albicans virulence factors have been identified Systemic infections associated with specific host risk factors The gastrointestinal tract is considered a major portal of entry for C. albicans Host Risk Factors for Systemic Candidiasis Colonization with Candida species Prematurity, especially GA < 28 weeks Very low birth weight Prolonged hospitalization Indwelling catheters Neutropenia Broad spectrum antibiotic therapy Third generation cephalosporin exposure Steroids Host Risk Factors for Systemic Candidiasis Hyperalimentation Hyperglycemia Indomethacin Intestinal perforation > NEC/IP Abdominal or cardiac surgery Compromised anatomic barriers Apgar score <5 at 5 min Topical Petrolatum Ointment (Aquaphor) NEC or IP Strong association IP ~25% incidence of canididasis Empiric therapy Incidence of Systemic Candidiasis associated with TPO in infants with BW ≤ 1500 grams Campbell JR, Zaccaria E, & Baker CJ, Pediatrics 2000;105:1041-1045. Virulence Factors C. albicans accounts for the majority of Candida spp isolated Multiple intrinsic C. albicans virulence factors have been identified Systemic infections associated with specific host risk factors The gastrointestinal tract is considered a major portal of entry for C. albicans Skin and GI tract colonization C. albicans and others GI tract commensal Acquired perinatally Vertical transmission from mother Colonization within 710 days (skin & GI) Higher levels of colonization associated with increased risk of systemic disease C. parapsilosis Skin colonization in adults (tinea versicolor) Skin or GI tract colonization in neonates Acquired postnatally Transmission from caregivers Colonization later, usually >14 days: rate higher with increased LOS Research Correlates Mouse models of IV infection and GI tract colonization developed. Models then used to evaluate: The role of yeast filamentation in colonization and infection. The role of antibiotics and steroids in colonization and dissemination. Candida albicans strains Comparisons were made using three C. albicans strains (all URA3/ura3): CAF-2: “wild type”/parent strain; exhibiting a normal phenotype forming blastoconidia, germ tubes, hyphae and pseudohyphae. (Fonzi, Genetics 1993;134:717) HLC4: cph1/cph1,efg1/efg1; a nonfilamentous mutant described as growing exclusively as blastoconidida. (Lo, Cell 1997;90:939) BCa2-10: tup1/tup1; grows exclusively in filamentous form. (Braun, Science 1997;277:105) Oral (107) or intravenous (105) inoculation of mice with C. albicans CAF-2, HCL54 or BCa2-10 I.V. C. albicans oral C. albicans Antibiotics 3 days Monitor for death Sacrifice 1, 7, 14, & 21 days later C. albicans 3 days I.P. Dex Sacrifice Antibiotics in drinking water: • bacitracin • streptomycin • gentamicin Dexamethasone: • 2mg I.P. BID 6 6 * 4 3 -/- -/-/+ 3 * +/+ 3 -/- 4 -/-/+ 4 5 -/-/+ 5 * +/+ 5 Antibiotics + LPS Antibiotics -/- No 6 antibiotics +/+ Avg ±SE log10 viable C. albicans /g cecum Affect of antibiotic treatment on cecal colonization in mice INT1 Genotype NOTE: C. albicans was recovered from the mesenteric lymph nodes of only an occasional mouse and never from the kidneys, with all treatments. Bendel et al. SHOCK. 2000; 13:453-8. Dexamethasone administration Colonization facilitated by dexamethasone - increased to 107.5 C. albicans recovered from the mesenteric lymph nodes in 56% of mice C. albicans disseminated to the kidneys in 83% of mice Bendel et al, Pediatric Research 51:290;2002 8 Cecal Colonization * = p<0.05 % of mice with C. albicans in tissue Avg±SE log10 viable C. albicans /g cecum Cecal colonization and dissemination of C. albicans to mesenteric lymph nodes (MLN) and kidneys of orally inoculated mice MLN * = p<0.05 100 100 7 6 * 5 4 3 CAF2 HLC54 BCa2-10 C.albicans strain Kidneys * = p<0.01 * 21/24 75 75 * * 12/24 11/22 50 25 50 25 3/22 0/21 0/21 0 0 CAF2 HLC54 BCa2-10 C.albicans strain CAF2 HLC54 BCa2-10 C.albicans strain % Cumulative Survival Mortality in mice inoculated IV with C. albicans wild type and mutant strains “Filamentous” only 100 80 60 “Nonfilamentous” 40 20 “Wild Type” 0 0 5 10 15 20 25 30 Days after intravenous 105 C. albicans Avg±SE log10 viable C. albicans. per gram Persistence of C. albicans in the kidney and liver of intravenously inoculated mice Kidney 8 * * 6 * Liver 8 * = P<.01 & † = P<.05 vs. BCa2-10 Day 1 Day 7 Day 14 Day 21 6 * * 4 4 † 2 2 0 0 CAF2 HLC54 BCa2-10 C. albicans strain CAF2 HLC54 BCa2-10 C. albicans strain A 50 microns B 20 microns 50 microns A 20 microns B PCR Results Using specific primers for the INT1 locus of CAF-2, the EFG-A and EFG-D fragments of HLC54, and the altered TUP1 locus of BCa2-10, PCR was performed on two C. albicans colonies recovered from each cecum and one colony from each MLN, liver and kidney that was positive for yeast. Results confirmed that mice were colonized with the inoculated strain. Summary I All three C.albicans strains persisted in the GI tract. “Wild type” and “Nonfilamentous” strains colonized in similarly high numbers, while the numbers of cecal “Filamentous only” present were at least 100-fold lower. Summary II Of the three C.albicans strains studied: CAF-2 (wild type) was most virulent in IV inoculated mice as assessed by mortality HLC54 (defective in filamentation) was most virulent in orally inoculated mice as assessed by extraintestinal dissemination of C. albicans. BCa2-10 (constitutively filamentous) was avirulent in both models. Summary III Both yeast cell and filamentous forms of wild type and “nonfilamentous” strains were found in kidney sections, but tissue necrosis was associated only with filamentous forms. Therefore, “morphologic switching” provides candida with an advantage for persistence throughout the host under a variety of conditions. C. albicans Adherence to Cultured Epithelium - ELISA wash, lightly fix, wash Incubate C. albicans with enterocytes (pretreated for 24o with dexamethasone) Incubate with primary antibody Remove enterocytes from plastic dish Color development and O.D. at 450 nm Secondary antibody conjugated to HRP Increased adhesion of C. albicans strains to Int 407 neonatal enterocytes following pretreatment with dexamethasone * * % Change in Adhesion 100.00% * 100uM de x * 1000uM de x * * 50.00% * * * 0.00% CAF2 10uM de x CAG3 C. a lbi ca nsstr a in CAG5 * p< 0.015 Increased adhesion of C. albicans strains to Caco-2 adult enterocytes following pretreatment with dexamethasone 100uM de x % Change in Adhesion 100.00% 1000uM de x * * 50.00% * 0.00% CAF2 CAG3 C. a lbi ca ns str ai n CAG5 * p< 0.05 C. albicans CAF2 (+/+) incubated 3 h on Caco-2 enterocytes showing alignment of adherent filamentous form along enterocyte cell borders Summary I Dexamethasone pretreatment of enterocytes resulted in a significant, dose dependent increase in the adhesion of all three C. albicans strains to both neonatal and adult cell lines. Neonatal enterocytes (Int407) were more sensitive to the effects of dexamethasone therapy. Greater increases in adhesion were observed for all C. albicans strains, at all concentrations, when compared to the adult Caco-2 cell line. Summary II No differences were seen in the dexamethasone effect on the adhesion of CAG3 and CAG5, compared to CAF2 — equivalent increases were noted to both cell lines at each concentration tested. Following dexamethasone treatment, preferential adhesion of the C. albicans along enterocyte cellular junctions was observed, compared to more homogeneous adhesion in the untreated cell lines. Adhesion of Candida strains to human epithelial cell monolayers Clinical Candidiasis Candida species are responsible for a wide variety of clinical disease with variable presentation and degree of severity “Benign” colonization Locally invasive disease Catheter-related fungemia Widespread systemic disease The specific disease process depends on the interplay of both host risk and yeast virulence factors Congenital Candidiasis - Term Age at onset : Birth or < 24 hours Presence of Risk Factors: None Skin involvement: Hallmark Respiratory involvement: Occasionally Positive Blood culture: No Multiorgan involvement: Never Treatment: Topical Antifungals Prognosis: Excellent Congenital Candidiasis - Preterm Age at onset : Birth or < 24 hours Presence of Risk Factors: None Skin involvement: Classical candidal dermatitis Atypical diffuse erythematous dermatitis Respiratory involvement: Common Positive Blood culture: Uncommon Multiorgan involvement: Rare Treatment: Parenteral Antifungal, avoid central catheters Prognosis: Guarded Catheter-Related Fungemia Age at onset : > 7 Days Presence of Risk Factors: Necessary Skin involvement: Uncommon Respiratory involvement: Infrequent Positive Blood culture: Yes Multiorgan involvement: Rare Treatment: Parenteral Antifungal Catheter removal Prognosis: Good Catheter-Related Fungemia: Complications Specific to site and type of catheter Cystitis Peritonitis Pleuritis Mediastinitis Central venous catheters Right atrial or other vascular fungal mass Disseminated Candidiasis Age at onset : > 7 Days Presence of Risk Factors: Necessary Skin involvement: None / Uncommon Respiratory involvement: Frequent Positive Blood culture: Yes Multiorgan involvement: Frequent Treatment: Parenteral Antifungal Prognosis: Fair - Poor Disseminated Candidiasis: Common Complications Pneumonia Meningitis < 500 WBC, lymphocytes Normal glucose Normal or increased protein Renal involvement Cystitis Multiple or single abcesses Pelvic fungal balls Endophthalmitis Significant ROP Drohan et al, Pediatrics 2002;110(5). Disseminated Candidiasis: Less Common Complications Endocarditis, pericarditis Bone or joint involvement Peritonitis ( with bowel perforation) Liver abscess Splenic abscess Cutaneous nodules/subcutaneous abcesses Diagnosis Nonspecific signs and symptoms of sepsis Fever Uncommon Positive Culture — NO Rapid test available Blood Urine (catheterized or suprapubic tap) CSF Other fluids as indicated ETT, skin, mucous membrane, GI tract cultures indicate colonization only Diagnosis — Cultures Fungal isolater tube not usually helpful Cultures should be held for a minimum of 710 days: non-albicans species are slow growing Monitor blood cultures daily until no growth and then weekly while on therapy Specific Candida species should be identified Sensitivities to antifungal drugs should be determined Schelonkam RL and Moser SA, J Pediatr 2003:142:564-5 Diagnosis — Other Studies CBC with differential and platelet count Thrombocytopenia COMMON WBC can be low, normal or high Serum glucose BUN and creatinine Ultrasound: renal, cranial, cardiac Ophthalmologic exam Bilirubin and liver enzymes Treatment — Topical Nystatin Miconazole Clotrimazole Gentian Violet Treatment — Parenteral Amphotericin B - mainstay of therapy Daily dosage: No “test dose” required in neonates ± Initial dose 0.5 mg/kg IV over 2-6 hours Increase by 0.5 mg/kg/d to goal of 1.0-1.5 mg/kg/d Adjust for renal insufficiency Treatment — Ampho B Treatment Course 10-14 days for uncomplicated line sepsis 3- 6 weeks for disseminated or complicated sepsis. Cumulative dose of 30-35 mg/kg or clearance of disease — whichever comes first! Monitor systemic involvement for improvement/clearance — serial ultrasounds, repeat cx, etc. Treatment — Ampho B Complications of therapy: Renal insufficiency Monitor UOP, BUN,Cr qod initially; then q week if stable Renal failure reversible, but dialysis may be required Profound hypokalemia / hypomagnesemia Monitor K and Mg levels closely Hematologic - bone marrow suppression Monitor CBC and platelets qod initially and then q week Liver dysfunction Adjunctive Therapy: 5-FC 5-fluorocytosine - Synergistic Dosing: 50-100 mg/kg/day po divided q 12 hours Monitor levels Limitations: Oral Rapid resistance occurs if used alone Alternative Therapy Liposomal Amphotericin B (Ambisome) or Amphotericin B Lipid Complex (Ablecet) or Amphotericin B colloidal dispersion Dosing: 3-5 mg/kg/day IV over 2hours Appears to be safe and effective, but not superior to conventional Ampho B Diminished side effects, especially renal Limitations: Decreased renal absorption Comparison of Antifungal medications Kicklighter SD. NeoReviews 3;12:249-255. 2002 Medication Route Daily Dose Cost/500 mg (mg/kg/24) (acquisition) Amphotericin B IV Fluconazole IV,PO 3 - 6 $66 Abelcet IV 3-4 $93 Amph B Colloid Disp IV 5 $135 Ambisome IV 3-5 $199 Flucytosine PO 50 - 200 $7 0.5 - 1.5 $12 Alternative Therapy Fluconazole — IV (vorconazole next generation) Dosing, over 2-6 hours: Preterm ≤ 29 weeks: 5-6 mg/kg/72 hours Preterm 30-36 weeks: 3-6 mg/kg/48 hours Term: 6-12 mg/kg/24-72 hours Monitor levels Side effects: renal, hepatic and hematologic, but less than Ampho B Yeast Susceptibilities Fairview-University Medical Center – 2009 Candida albicans Candida glabrata Candida krusei Candida Candida tropicalis parapsilosis Ampho B 99% 99% 100% 100% 100% 5-FC 99% 98% 0% 93% 99% Fluco nazole 97% 44% O% 79% 95% Itraco nazole 92% 26% 39% 77% 95% Alternative Therapy Echinocandin Caspofungin Micafungin ? Prophylaxis ? Key to preventing disease appears to be diminishing colonization and risk of dissemination. Chemoprophylaxis ? Nystatin / Mycostatin (?efficacy, benign) Fluconazole (?efficacy, ? benign) Molecularly generated inhibitory proteins? Fluconazole Prophylaxis Kaufman et al, NEJM 200;345 IV fluconazole for the first six weeks of life in infants with BW ≤ 1000g Decreased levels of colonization (20 v 60%) Fewer invasive fungal infections (0 v 20%) Safe, no change in sensitivity patterns Caveats Extremely high rate of invasive infections TPO/Aquaphor used Unable to determine pressure for resistance . Many thanks to all who have helped with the research! Adhesion studies: Mary Keane & Beth Swanson Animal studies: MaryAlice Johnson & Robb Garni Microscopy: Stanley Erlandson & Michelle Henry-Stanley Everything: Carol Wells