Mazen Kherallah, MD, FCCP
Case Scenario
• 17 year old male with PMH cyctinosis
complicated with chronic renal failure requiring
kidney transplantation X2 that failed and placed
on chronic dialysis, patient acquired HBV
• Admitted on January 17, 2010 with:
– Fulminant hepatitis secondary to HBV
– Acute liver failure
– Coagulopathy
– Hepatic encephalopathy
Management
•
•
•
•
•
ICU monitoring
Dialysis continued
Vitamin K
Lactulose
Not candidate for liver transplantation
January 21, 2010
•
•
•
•
•
•
•
Respiratory distress
Fever
Developed bilateral pulmonary infiltrates
Intubated
FiO2 50%, pO2: 65 mm Hg
Yellowish endotracheal aspirate
WBC: 12.400
Which of the following organisms is unlikely
in this situation?
A. Pseudomonas aerugniosa
B. Escherichia coli
C. Staphylococcus aureus
D. Klebsiella pneumoniae
E. Haemophillus influenza
Tracheal Aspirate Gram Stain
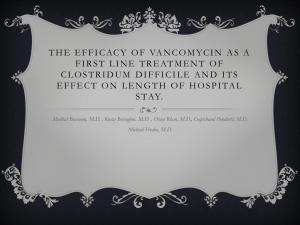
Common HAP Pathogens in ICU Patients
n=4365
Others
Data from the National Nosocomial Infections Surveillance (NNIS) system (1986–2003) for HAP. Gaynes et al. CID 2005;41:848– 54.
What empiric antibiotics would you choose
at this time?
A. Ceftriaxone + metronidazole
B. Ceftazidime + vancomycin
C. Pipercillin/tazobactam + vancomycin
D. Meropenem + vancomycin
E. Ciprofloxacin + amikacin + vancomycin
Hospital Acquired Aspiration Pneumonia
Antibiotic Selection
Pseudomonas
aeruginosa
•Piperacillin / tazobactam
•Ceftazidime
•Cefepime
•Ceftobiprole
•Carbapenems
•Aztreonam
•Ciprofloxacin
•± aminoglycoside
Anaerobes
GPC/MRSA
Enterobacteriacae
• Vancomycin
• Ticoplanin
• Telavancin
• Daptomycin
• Linezolid
• Qunupristin/Dalfopistin
• Tigecycline
• Clindamycin
• Metronidazole
• Amoxicillin/clavulanate
• Clindamycin
• Piperacillin/tazobactam
• Amoxicillin /
• Third- and fourthgeneration cephalosporins clavulanate
• Piperacillin /
• Carbapenems
tazobactam
• Fluoroquinolones
• Cefoxitin
• Tigecycline
• Carbapenems
• Moxifloxacin
• Tigecycline
Carbapenem
(Imipenem,
Doripenem
or
Meriopenem)
± AG
or
Ciprofloxacin
Glycopeptide
β -lactam/β-lactamase
inhibitor
(PIP/TAZ)
± AG
or±Ciprofloxacin
±±Glycopeptide
Cefepime
± AG
or
Ciprofloxacin
Glycopeptide
Ceftazidime
± AG
or Ciprofloxacin
±
Glycopeptide
Broncho-alveolar Lavage
ATS combination treatment guidelines for
healthcare-acquired pneumonia (HCAP)
β -lactam/β-lactamase
inhibitor (PIP/TAZ)
Antipseudomonal
Fluoroquinolone
(ciprofloxacin or
levofloxacin)
OR
Antipseudomonal
carbapenem
(imipenem or
meropenem)
OR
Antipseudomonal
cephalosporin
(cefipime or
ceftazidime)
+
OR
Aminoglycoside
(amikacin,
gentamicin
or tobramycin)
ATS/IDS. Am J Respir Crit Care Med 2005;171:388-416
Vancomycin
+
Linezolid
Antibiotic Course
Pip/Taz
Vancomycin
January 31, 2010
• Developed acute abdominal pain
• Distended abdomen with tenderness and
decreased bowel sounds
Perforated Viscus
• Managed conservatively secondary to high
risk surgery
Which of the following organisms is least
likely in this situation?
A. Bacteroides fragilis
B. Pseudomonas aerugniosa
C. Escherichia coli
D. Klebsiella pneumoniae
E. Enterococcus
Microbiology of Peritonitis
Primary
(Monomicrobial)
E. coli
Klebsiella spp.
Streptococcus spp.
Enterococcus spp.
Other gram-negative bacilli
S. anginosus
Secondary
(Polymicrobial)
B. fragilis group
Tertiary
(Polymicrobial)
Enterococci
E. coli
Clostridium spp.
Klebsiella spp.
Streptococcus spp.
Enterococcus spp.
Pseudomonas
S. epidermidis
Candida
Pseudomonas spp.
E. coli
©Copyright 2005 cmsp.com / All rights reserved
S. epidermidis
B. fragilis
©Copyright 2005 cmsp.com / All rights reserved
©Copyright 2005 gbf.de / All rights reserved
Barie PS. J Chemother. 1999;11:464-477.
LaRoche M, Harding G. Eur J Clin Microbiol Infect Dis. 1998;17:542-550.
64
What empiric antibiotics would you choose
at this time?
A. Ceftriaxone + metronidazole
B. Pipercillin/tazobactam
C. Imipenem
D. Tigecycline
E. Ciprofloxicin + metronidazole
Secondary Peritonitis
(Antibiotic Selection)
Enterobacteriacea
B. Fragilis Group
Enterococcus
Amoxicillin / clavulanate
Metronidazole
Ampicillin
Piperacillin / tazobactam
Clindamycin
Vancomycin
Carbapenems
Amoxicillin / clavulanate
Ticoplanin
3rd gen cephalosporins
Piperacillin / tazobactam
Telavancin
4rd gen cephalosporins
Cefoxitin
±Aminoglycosides
Aztreonam
Carbapenems
Daptomycin
Fluoroquinolones
Moxifloxacin
Linezolid
± aminoglycoside
Tigecycline
Qunupristin/Dalfopistin
Tigecycline
Tigecycline
Risk factors for ESBL, AmpC or MDR?
Abdominal Drainage Feb 1, 2010
Antibiotic Course
Pip/Taz
Vancomycin
Meroppenem
Vancomycin
Fluconazole
Feb 6, 2010
• No improvement with concervative
approach
• CT scan abdomen
CT Scan Report
• Significant wall thickening involving the large and small
bowel loops with patent abdominal vessels, probably
representing nonocclusive bowel ischemia with
differential diagnosis inflammatory bowel disease.
• Interval progression of ascites with interval regression of
pneumoperitoneum.
• Interval progression of bilateral pleural effusion with
passive basal atelectatic changes. The rest of the
examination is unchanged compared with the recent
previous study done on 1 February 2010.
ICU Course
•
•
•
•
•
Laporatomy revealed peritonitis
No clear perforation site
Washing and drains placed
Improved over the next days
Discharged to floor
February 19, 20010
•
•
•
•
•
•
•
•
•
Fever: T: 101.3
Hypotension: SBP 70
Tachypnea: RR 32
Tachycardia: 130/min
WBC: 28.4
pO2: 56 on FiO2 60%
Thrombocytopenia: 87,000
Anuric
Lactic acid: 4.2
Sepsis Continuum
Infection
SIRS
Microorganism
invading
sterile tissue
A clinical
response arising
from a nonspecific
insult, with 2 of
the following:
T >38oC or
<36oC
HR >90
beats/min
RR >20/min
WBC
>12,000/mm3
or <4,000/mm3
or >10% bands
Sepsis
Severe Sepsis Septic Shock
SIRS with a
presumed
or confirmed
infectious
process
Sepsis with
organ failure
Vascular collapse
Renal
Hemostasis
Lung
LA
Refractory
hypotension
Chest 1992;101:1644
Sepsis Syndromes
1992: SCCM/ACCP
Parasite
Virus
Severe
Sepsis
Infection
Sepsis
SIRS
Fungus
Shock
Trauma
BSI
Bacteria
Burns
What is the likely source of sepsis?
A.
B.
C.
D.
E.
F.
Line infection?
Nosocomial pneumonia?
Further cIAI with or without abscesses?
Urinary catheter-related infection?
C-diff colitis
Any of the above
Urinalysis
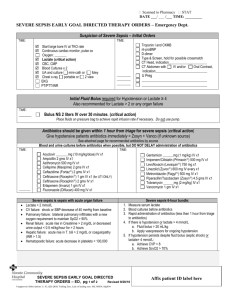
Severe Sepsis Management
Source Control
Early Goal
Directed
Therapy
Appropriate and
Adequate
Empiric
Antibiotics
Which of the following organisms is least
likely in this situation?
A. Bacteroides fragilis
B. Pseudomonas aerugniosa
C. Proteus mirabilis
D. Candida albicans
E. Enterococcus
CR-UTI
(Antibiotic Selection)
Candida
Pseudomonas
Enterococcus
Piperacillin / tazobactam
Ampho B
Ampicillin
Carbapenems
Azoles
Vancomycin
Ceftazidime
Ticoplanin
Cefepime
Telavancin
Ceftobiprole
±Aminoglycosides
Aztreonam
Daptomycin
Ciprofloxacin
Linezolid
± aminoglycoside
Qunupristin/Dalfopistin
Tigecycline
Risk factors for ESBL, AmpC or MDR?
What empiric antibiotics would you choose
at this time?
A. Ceftazidime
B. Pipercillin/tazobactam
C. Imipenem
D. Tigecycline
E. Ciprofloxicin
Blood Culture
Urine Culture
Antibiotic Course
Pip/Taz
Vancomycin
Meroppenem
Vancomycin
Fluconazole
Pip/Taz
Vancomycin
February 25, 2010
• Wound dehiscence
• Surgically reduced
• Complicated with intra-abdominal bleed
which was surgically and medically
controlled
19/2/2010
March 1, 2010
•
•
•
•
•
Distended abdomen
Decreased bowel sounds
Fever
WBC 2.5
Abdominal fluids: >1200 WBC, 85%PMN’s
Which of the following organisms is least
likely in this situation?
A. Bacteroides fragilis
B. Pseudomonas aerugniosa
C. Proteus mirabilis
D. Candida albicans
E. Enterococcus
Which of the following resistant mechanism
is likely in this situation?
A. ESBL
B. AmpC
C. KPC
D. Capabemases
E. Any of the above
What empiric antibiotics would you choose
at this time?
A. Tigecycline + anidulafungin
B. Colistin + anidulafungin
C. Meropinem + anidulafungin
D. Colistin+ Ceftazidime + anidulafungin
E. Piperacillin/tazobactam + anidulafungin
Tertiary Peritonitis
(Antibiotic Selection)
MDR Pseudomonas
Candida
Enterococcus
Meropenem
Ampho B
Ampicillin
Doripenem
Anidulafungin
Vancomycin
Imipenm
Caspofungin
Ticoplanin
Colistin
Micafungin
Telavancin
Cefepime
Fluconazole
±Aminoglycosides
Ceftobiprole
Voriconazole
Daptomycin
Aztreonam
Linezolid
Ciprofloxacin
Qunupristin/Dalfopistin
± aminoglycoside
Tigecycline
Risk factors for ESBL, AmpC or MDR?
March 1, 2010
Antibiotic Course
Pip/Taz
Vancomycin
Meroppenem
Vancomycin
Fluconazole
Pip/Taz
Vancomycin
Meropenem
Colistin
Caspofungin
Vancomycin
March 13, 2010
• Tertiary peritonitis
• Not responding
• Bacteremia
Peritoneal Fluid
March 13, 2010
March 13, 2010
Antibiotic Course
Pip/Taz
Vancomycin
Meroppenem
Vancomycin
Fluconazole
Pip/Taz
Vancomycin
Meropenem
Colistin
Caspofungin
Amikacin
Tigecycline
Findings
Quite large amounts of pleural effusion seen on the right side with
adjacent atelectasis and spread opacifications seen in the visualized
lower part of the lung. The amount of pleural effusion on the right
side is essentially unchanged compared to previous examination
dated February 6, 2010. On the left side, the pleural effusion seen
previously has resolved and there is now atelectasis seen in the
lower part of the left lung.
No free air intraabdominally. Nasogastric tube with its tip in the
duodenum. Double abdominal drains, one on each side. There are
dilated bowel loops, both small and large bowel, but there is gas
seen all the way to the rectum. There is some free fluid
intraabdominally with variable attenuation. No certain collection
though. The variability of the free fluid density is of uncertain cause,
contrast leak? though no free air. Blood/clotted blood? Kidney
transplants seen to the left and right in the pelvis. Splenomegaly.
Previous examination revealed extensive wall thickening of both
small and large bowel. Today, there is remaining wall thickness of
small bowel loops.
March 21, 2010
• Right pleural effusion
Persistent Bacteremia
March 23-April 23
Blood
Body Fluid
MDR Pseudomonas
What persistent pseudomonas bacteremia
indicate?
A. Persistent intra-abdominal infection
B. Persistent pneumonia
C. Catheter related blood stream infection
D. Enterovesicular fistula
E. Endocarditis
April 17, 2010
• Fever
• Increasing FiO2
What Organisms?
Stenotrophomonas maltophilia
Pseudomonas aeruginosa
Flavobacterium
April 17, 2010
What antibiotics would you add?
A. Bactrim
B. Doxyclycline
C. Tigecycline
D. Imipenem
E. Chramphenicole