King LT-D Airway Training Program
advertisement

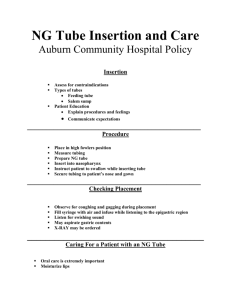
Verde Valley EMS Educational Outcome To enable EMS providers to appropriately, effectively, quickly and safely utilize the King LT-D® (KLTD) and King LTS-D® (KLTSD) airway devices in the prehospital environment. Advantages of the KLTD/KLTSD • Easier to place and use. One port to inflate One tube to ventilate Does not require extensive skill training • • • • • Can be placed quickly. Provides a means for positive-pressure ventilation. No interruption of CPR necessary. Little or no spinal movement necessary. Lower incidence of sore throat and trauma. Advantages of the King continued • Smaller than other devices (e.g., Combitube). • More cost-effective than other options. • Minimizes gastric insufflation. • LTS-D enables passing of gastric tube into stomach. • Comes in various sizes. #3: 4–5 feet #4: 5–6 feet #5: Greater than 6 feet Research & Experience • Preliminary research. Formal studies of the King LT-D/LTS-D are limited, but suggest positive results. Prehospital studies of the King LT-D/LTS-D are currently ongoing, and others will be published soon. Research articles available on the King System’s website (www.kingsystems.com). • Other agencies seeing positive results. As of February 2007, Clackamas County Fire District #1 had done 21 insertions with a 90% success rate. Anecdotal evidence from Clackamas suggests a higher rate of ROSC in cardiac arrest patients intubated with the King. Disadvantages • Patient must be unresponsive without a gag reflex. Design of the King LTS-D Pilot Balloon Proximal Opening of Gastric Access Lumen Primary Ventilatory Opening Proximal Cuff Stabilizes tube & seals oropharynx Multiple Distal Ventilatory Openings Bilateral Ventilation Eyelets Distal Opening of Gastric Access Lumen Distal Tip & Cuff Anatomically shaped to assist in passage behind larynx and normally collapsed esophagus King LTS-D Design Distal tip and cuff flattened for more anatomical fit behind larynx Multiple outlets and bilateral eyelets, in order to obtain best ventilation continued… Ramp directs tube exchange catheter out main ventilatory opening Comparison of Tube Sizes Range: 45–60 ml Range: 60–80 ml Range: 70–90 ml Indications • When tracheal intubation indicated, but unsuccessful or unavailable. • Access to the patient is limited (e.g., trauma patients, entrapment, etc.). • Difficult or emergent airways, in which other options may not be feasible. • Cardiopulmonary arrest (optional). Contraindications • Presence of gag reflex. • Caustic ingestion. • Obstructed airway. Same contraindications as the Combitube • Esophageal trauma or disease. Insertion Procedure • Have all equipment ready prior to attempt. • Test cuff inflation system for leaks. • Apply a water-soluble lubricant to the posterior distal tip of the device. • Hold KLTD/KLTSD in dominant hand at proximal connector. • Use a superior (to patient’s head) approach. • Perform tongue-jaw lift while keeping head in a neutral position. Head can be slightly extended or placed in the “sniffing” position if needed to facilitate placement. Insertion Procedure • With the King LT (S)-D rotated laterally 45-90 degrees such that the blue orientation line is touching the corner of the mouth, introduce tip into mouth and advance behind base of the tongue. • As the tube passes under the tongue, rotate the tube back to midline (blue orientation line faces chin). continued… Patient Insertion Insertion Procedure continued… • Without excessive force, advance tube until connector is aligned with teeth and/or gums. It is important that that the King is advanced all the way. Insertion Procedure • Using a syringe, inflate the cuffs with the appropriate volume of air. • Special (reusable) color-coded syringes can be utilized. #3: 45–60 ml #4: 60–80 ml #5: 70–90 ml continued… Insertion Procedure • Attach BVM to 15 mm connector. • While ventilating, simultaneously withdraw until ventilation is easy and free-flowing. There should be good tidal volume with minimal resistance. continued… Insertion Procedure continued… • Perform standard evaluation of lung sounds while ventilating through the King LT-D/LTS-D. • Attach and utilize end-tidal CO2 monitoring while the King LT-D/LTS-D is in place. • Readjust cuff inflation as needed. • Consider securing with tape or ET tube holder. Securing with tape or ET tube holder not required, but recommended. With cuffs inflated, King tends to fit snugly and securely. Proper Position of the KLTD/KLTSD The KLTSD Gastric Access Lumen • Lubricate gastric tube prior to inserting into the gastric access lumen. • Up to an 18 Fr catheter may be utilized. • Attach suction unit to catheter. • Once stomach contents are evacuated and suction no longer necessary, suction device may be detached. • Catheter may left in place to “plug” lumen, and to continue to decompress the stomach. Important Points & User Tips • To avoid tracheal placement maintain head in a neutral position. Ventilation will not occur if placed in the trachea. • If unable to ventilate, remove device and replace. • If water soluble lubricant used, do not apply near ventilatory openings. • Be prepared to re-inflate cuffs with another 10–15 cc in the event of air leakage (do not over-inflate). • Insertion depth is critical, as the ventilatory openings must align with the laryngeal opening. Important Points continued… Be certain to advance the King LT-D/LTS-D until the base of the connector is aligned with the teeth and/or gums… Failure to do so may result in a failed intubation attempt! Return of Spontaneous Breathing • If patient regains consciousness and respiratory drive, and is not tolerating the King, consider extubation. Place them on their side and fully deflate cuffs. Gently withdraw the tube. Have suction ready and be prepared for vomiting. • If patient regains respiratory drive, but remains unconscious but combative: Consider sedation with midazolam and vecuronium. Continue providing or assisting ventilations as necessary. Spontaneous Breathing continued… • During spontaneous breathing, the epiglottis or other tissue can be drawn into the ventilatory openings. This can result in obstruction. Advancing the King 1–2 cm normally eliminates this obstruction. King LTD Airway 2.0 & 2.5 Questions? Questions? Questions?