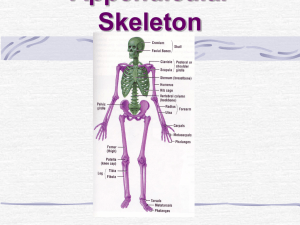
The Arm
advertisement

-video The Hand • We will start off at the hand. You will need an understanding of the bones that make up our hand, because they will act as insertion points for the forearm muscles Ulna Carpals Metacarpals Phalanges Radius The Forearm • is the area of the appendicular skeleton stretching from the elbow to the wrist - let’s take a look at the skeletal components of the forearm Head Neck Radial tuberosity Olecranon process Coronoid process ULNA Interosseus membrane RADIUS Styloid process The Forearm • is the area of the appendicular skeleton stretching from the elbow to the wrist - let’s take a look at the skeletal components of the forearm • SUPINATION is a very important movement of the forearm • we need to view the movement of the forearm from 2 different angles • At the elbow, the forearm is dominantly the ulna • At the wrist, the forearm is dominantly the radius Upon supination • radius spins on its axis at the elbow, but orbits around the head of the ulna at the wrist • movement stops when radius buts up against the ulna - The humerus is a long bone that connects the shoulder (scapula) and the lower arm (radius and ulna) Posterior Greater Tubercle Surgical neck Anterior Greater Tubercle Head Anatomical neck Lesser Tubercle Deltoid Tuberosity Olecranon fossa Lateral epicondyle Coronoid fossa Medial epicondyle Trochlea Capitulum Tubercle: A round nodule or “warty” outgrowth of a bone Fossa: A depression or hollow on a bone Trochlea: A grooved structure resembling a “pulley wheel” Posterior Muscles of the Forearm Extensor carpi radialis longus O: above lateral epicondyle of humerus Extensor I: basecarpi of 2ndulnaris metacarpal F: and abduct wrist Extensor O:extend lateral digitum epicondyle of humerus and ulna Extensor carpi radialis brevis I:O:base of 5th metacarpal lateral epicondyle of the humerus F: adducts Flexor O: lateral carpi epicondyle ulnaris ofwrist humerus I: extends all digitsand except thumb rd 1 O:base 2 heads: medial epicondyle, 1 olecranon I: of 3interphalangeal metacarpal F: extends joints (fingers) th metacarpal I: extends base of 5and F: abducts the wrist Thenar Eminence: muscles proximal to thumb (3) F: flexes and adducts the wrist -flex, adduct and oppose thumb Hypothenar Eminence: muscles proximal to little finger (3) -abduct, flex, oppose little finger Anterior Muscles of the Forearm Biceps brachii Brachialis Supinator O: lower anterior humerus Pronator teres I: coronoid process ulna O: Lateral epicondyle humerus Brachioradialis O: medial humerus F:epicondyle flexes elbow I: anterior & lateral aspect of and coronoid process of ulna O: above radius lateral epicondyle Flexor carpi radialis humerus I: lateral surface offorearm mid radius F: Supinating O:F: medial epicondyle I: styloid process radius humerus pronates forearm/ flex elbow second metacarpal (index) F: I: elbow flexor Flexor carpi ulnaris F: flexes and abducts hand Pronator quadratus O: anterior surface of distal ulna I: anterior surface of distal radialis F: pronates forearm Forearm Flexors: Part I -http://www.youtube.com/watch?v=DIwO1ld7vM8&feature=related Part II -http://www.youtube.com/watch?v=QSy9MB69AkM&feature=related Forearm Extensors: Part I -http://www.youtube.com/watch?v=Cw3xr8_rLMU&feature=related Part II -http://www.youtube.com/watch?v=XObJNybS1-I&feature=related Upper Arm: http://www.youtube.com/watch?v=vnb2iTnlAN0&feature=related Shoulder: Part I -http://www.youtube.com/watch?v=t5sLRGQ_Ews&feature=related Part II -http://www.youtube.com/watch?v=FDxe1hdHrHY&feature=related . . .a hinge joint formed by the articulation of the humerus of the arm and the ulna and radius of the forearm -video Elbow Ligaments Radial collateral ligament Ulnar collateral ligament (prevents excessive adbuction) (prevents excessive adduction) Tennis Elbow (lateral epicondylitis) -extensor carpi radialis brevis -chronic pain on lateral side of elbow - RICE & Physio -video (maintains articulation of radius with humerus) -video . . .three bones (clavicle, scapula and humerus) articulate forming this ball and socket joint Superior angle Medial border Inferior angle What view? Muscles of the Upper Arm Anterior Corachobrachialis O: coracoid process I: medial aspect of humerus F: Teres flexesmajor and adducts arm O:brachii inferior lateral border of scapula Biceps humerus O: I: short head –coracoid process; long head – supraglenoid tubercle adduction and F: medial rotation, extension of upper arm I: radial tuberosity (radius) Brachialis F: flexes supined elbow, supination Brachioradialis Triceps brachii O: lateral head –posterior aspect of humerus; long head –infraglenoid tubercle of scapula; medial head – posterior aspect of humerus I: olecranon process F: extends arm Posterior head Lateral head Anterior head Deltoid O: clavicle, acromium and spine of scapula I: deltoid tuberosity of the humerus F: anterior –flexes and medially rotates; lateral –abducts the arm; posterior –extends and laterally rotates arm Forearm Flexors: Part I -http://www.youtube.com/watch?v=DIwO1ld7vM8&feature=related Part II -http://www.youtube.com/watch?v=QSy9MB69AkM&feature=related Forearm Extensors: Part I -http://www.youtube.com/watch?v=Cw3xr8_rLMU&feature=related Part II -http://www.youtube.com/watch?v=XObJNybS1-I&feature=related Upper Arm: http://www.youtube.com/watch?v=vnb2iTnlAN0&feature=related Shoulder: Part I -http://www.youtube.com/watch?v=t5sLRGQ_Ews&feature=related Part II -http://www.youtube.com/watch?v=FDxe1hdHrHY&feature=related -there are really 3 joints in the shoulder: • glenohumeral • acromioclavicular • sternoclavicular - The shoulder must be flexible for the wide range of motion required in the arms and hands and also strong enough to allow for actions such as lifting, pushing and pulling. The compromise between these two functions results in a large number of shoulder problems Ligaments of the Shoulder Joint Coracoclavicular ligament Coracoacromial ligament Superior glenohumeral ligament Medial glenohumeral ligament Inferior glenohumeral ligament There is also a synovial fluid-filled capsule that encompasses the shoulder (attaches to the scapula, humerus and head of biceps) . The capsule is strengthened by the coracohumeral ligament Muscles of the Rotator Cuff - a group of muscles that extend from the scapula to the humerus and wrap around the shoulder joint basically holding it in place Supraspinatus Infraspinatus Subscapularis FRONT BACK Teres Minor Supraspinatus O: posterior surface of scapula above spine Insertion: all fuse to form tendon inserting on greater tubercle of humerus Infraspinatus O: poseterior surface of scapula below spine F: stabilize the shoulder; supra– abducts shoulder, infra and teres– laterally rotate shoulder Teres Minor O: later border of scapula Subscapularis O: anterior surface of the scapula I: Lesser tubercle of the humerus F: medially rotates humerus; stabilizes shoulder Forearm Flexors: Part I -http://www.youtube.com/watch?v=DIwO1ld7vM8&feature=related Part II -http://www.youtube.com/watch?v=QSy9MB69AkM&feature=related Forearm Extensors: Part I -http://www.youtube.com/watch?v=Cw3xr8_rLMU&feature=related Part II -http://www.youtube.com/watch?v=XObJNybS1-I&feature=related Upper Arm: http://www.youtube.com/watch?v=vnb2iTnlAN0&feature=related Shoulder: Part I -http://www.youtube.com/watch?v=t5sLRGQ_Ews&feature=related Part II -http://www.youtube.com/watch?v=FDxe1hdHrHY&feature=related Rotator Cuff Tears • The rotator cuff is made up of 4 different muscles: supraspinatus, infraspinatus, subscapularis and teres minor. •The term “cuff” refers to how the muscles cover the head of the humerus • May be ACUTE or CHRONIC Due to overheard motions Rotator Cuff Tears -video • The rotator cuff is made up of 4 different muscles: supraspinatus, infraspinatus, subscapularis and teres minor. •The term “cuff” refers to how the muscles cover the head of the humerus • May be ACUTE or CHRONIC Due to overhead motions • Symptoms: -pain in front of shoulder radiating down the arm (acute) “snapping” -pain when lifting/lowering arm -weakness in arm - crepitus “cracking” sound on movement ** symptoms may emerge gradually if tear is a product of overuse (chronic) ** Treatment - the vast majority of rotator cuff tears can be treated without surgery Non-operative treatments include: -physical therapy -anti inflammatory medications -cortisone shots -reduce inflammation, strengthen uninjured muscles around joint to compensate for injured muscles If surgery is necessary: -different options depending on severity, location of tear, physical activity level of patient and hopes for future use -proper rehab, stretching, avoiding movements that could reinjure the tendons