Grade 2C
advertisement

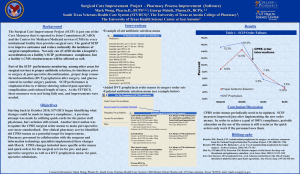
Prevention of Venous Thromboembolism in Nonorthopedic Surgical Patients ----Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Copyright: American College of Chest Physicians 2012© Learning Objectives • Describe a formal methodology for the evidencebased development of clinical practice guidelines • Review select studies of venous thromboembolism (VTE) prevention in surgical patients, as well as the limitations of the studies • Summarize recommendations for VTE prevention in specific surgical populations THERE IS NO LEVEL I EVIDENCE VTE • Thrombosis: the formation or presence of a blood clot within a blood vessel Merriam-Webster’s Medical Dictionary • Embolism: obstruction or occlusion of a vessel by a transported clot or vegetation, a mass of bacteria, or other … material Stedman’s Medical Dictionary Deep Vein Thrombosis (DVT) Pulmonary Embolism (PE) Goldhaber SZ. N Engl J Med. 1998;339(2):93-104. Pulmonary Angiography Bliss et al. N Engl J Med. 2002;347(23):1876-1881. CT Pulmonary Angiography Goldhaber SZ. N Engl J Med. 1998;339(2):93-104. Kearon SF. CMAJ. 2003;168:183-194. Risk Factors: Virchow’s Triad • Stasis – Immobility – Congestive heart failure • Injury – Surgery (especially major orthopedic and pelvic) – Trauma • Thrombophilia – Cancer – Oral contraceptives – Hereditary states (factor V Leiden, PT mutations) VTE Epidemiology • Most common cause of preventable death in hospitalized patients • Risk of fatal perioperative PE ~0.8% International Multicentre Trial. Lancet. 1975 • 150,000 to 200,000 deaths per year; ~1/3 in perioperative patients Horlander et al. Arch Intern Med. 2003;163:1711-1717. • AHRQ: VTE prevention is number 1 priority to improve safety in hospitals Many Surgical Patients At-Risk • 2003 Nationwide Inpatient Sample • Adult surgical patients, LOS ≥2 days • 7.8 million surgical discharges • • • • 44% low risk 15% moderate risk 24% high risk 17% very high risk • 4.4 million at risk for VTE Anderson et al. Am J Hematol. 2007;82:777-782. Million Women Study • Population-based, prospective cohort study • 947,454 middle-aged women in U.K. enrolled between 1996-2001 • Mean follow-up 6.2 years • 239,614 underwent surgery – 5,419 readmitted for VTE within 12 weeks of inpatient surgery (2.25%) – 270 deaths from fatal PE Sweetland et al. BMJ. 2009;339:b4583. Additional Challenges • Numerous comparisons – LDUH, LMWH, fondaparinux, low-dose ASA, high-dose ASA, ES and IPC vs no prophy – Mechanical vs pharmacologic – Add mechanical to pharmacologic – 16 unique evidence profiles and still counting! • Numerous surgical populations – – – – Abdomen and pelvis (vascular, bariatric) Neurosurgery (craniotomy, spine) Trauma (TBI, SCI, other major trauma) Cardiac, thoracic, other… VTE Consequences • • • • • • • Leg swelling, discomfort (DVT) Dyspnea, chest pain, hemoptysis, hypoxemia (PE) Extended hospital LOS Fatal PE (RV failure) ≥3 months of anticoagulant treatment Postphlebitic syndrome Chronic thromboembolic pulmonary HTN (~4%) Pengo et al. N Engl J Med. 2004;350:2257-2264. VTE Prevention • Targets one or two legs of Virchow’s triad: – Mechanical prophylaxis (stasis) • Elastic compression stockings • Intermittent pneumatic compression devices VTE Prevention • Targets one or two legs of Virchow’s triad: – Mechanical prophylaxis (stasis) • Elastic compression stockings • Intermittent pneumatic compression devices – Pharmacological prophylaxis (hypercoagulability) • • • • Unfractionated heparin Low-molecular-weight heparins Fondaparinux Aspirin (?) Guidelines Defined “Systematically developed statements to assist practitioners and patient decisions about appropriate health care for specific circumstances.” Field MJ, Lohr KN (eds). Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine, Washington, DC: National Academy Press, 1990. Guidelines and Performance Measures • Public reporting – Cardiac surgery outcomes in New York State • Pay for performance – Reward “good” behavior – CMS: several VTE prevention P4P measures • Registries – Accreditation – Facilitate quality improvement Case Scenario • 50 year-old woman scheduled to undergo elective laparoscopic cholecystectomy – – – – PMH notable for moderate emphysema No personal or family history of VTE Medications: Spiriva®, albuterol Stopped smoking 1 year ago • What should we recommend for perioperative VTE prophylaxis in this patient? Conceptual Framework • VTE pharmacoprophylaxis involves a tradeoff between preventing thrombosis and causing bleeding • When making tradeoffs, need to compare absolute risks of thrombosis and bleeding • In order to determine absolute risks (eg, number of symptomatic DVTs prevented), need to know the following: – Baseline risk in control/comparison group – Relative risk for intervention vs control • When making tradeoffs, also need to assign values to events being compared Calculating Absolute Effects Scenario Any surgical patient Baseline Risk of sVTE (%) Baseline Risk of Major Bleeding (%) ? ? RR VTE RR Bleed Number Number (UFH vs (UFH vs of VTEs of Bleeds no no Prevented Caused Prophy) Prophy) (per 1000) (per 1000) 0.50 2.0 ? ? Calculating Absolute Effects Scenario Baseline Risk of sVTE (%) Baseline Risk of Major Bleeding (%) RR VTE (UFH vs no Prophy) Moderate VTE/ Average Bleed 2 1 10 10 Moderate VTE/ High bleed 2 2 10 20 High VTE/ average bleed 4 1 20 10 High VTE/ high bleed 4 2 20 20 0.50 RR Bleed (UFH vs no Prophy) 2.0 Number of VTEs Prevented (per 1000) Number of Bleeds Caused (per 1000) Estimating Baseline Risk • Retrospective, observational study • Large sample (n=8,216) of consecutively admitted “general” surgical inpatients • Tertiary center • Measured clinically suspected, objectively confirmed VTE over 30 days • Risk stratification according to patient-specific and procedure-specific characteristics • Prophylaxis nonuniform but reported Baseline Risk of VTE Case Scenario • 50-year-old woman scheduled to undergo elective laparoscopic cholecystectomy – – – – PMH notable for moderate COPD No personal or family history of VTE Medications: Spiriva®, albuterol Stopped smoking 1 year ago • What should we recommend for perioperative VTE prophylaxis in this patient? Baseline Risk of VTE (Caprini Score) 4 Baseline Risk of VTE Bahl et al. Ann Surg. 2010;251:344-350. Baseline Risk of VTE 52% 0.1% 10% 37% Bahl et al. Ann Surg. 2010;251:344-350. IMT Results: Bleeding Outcome LDUH N=2045 No Prophylaxis N=2076 RR 4 5 0.81 (0.21 to 3.0) Excessive intra-op 182 126 1.47 (1.18 to 1.82) Wound hematoma 158 117 1.37 (1.09 to 1.73) 202/731 202/744 1.02 (0.86 to 1.20) Fatal bleed Transfusion Calculating Absolute Effects Scenario Moderate VTE-Risk Patient Baseline Risk of sVTE RR VTE (UFH vs no Prophy) (%) Baseline Risk of Major Bleeding (%) RR Bleed (UFH vs no Prophy) 2.6 1.2 0.59 1.57 Number Number of VTEs of Bleeds Prevented Caused (per 1000) (per 1000) 11 7 Evidence Synthesis: Tradeoffs between desirable and undesirable outcomes Recommendation For general surgical patients at moderate risk for venous thromboembolism who are not at high risk for perioperative bleeding, we suggest low-dose unfractionated heparin (Grade 2B) over no prophylaxis. Recommendation For general surgical patients at high risk for venous thromboembolism who are not at high risk for perioperative bleeding, we recommend use of low-dose unfractionated heparin (Grade 1B) over no prophylaxis. Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients at very low risk for VTE (< 0.5%; Rogers score, < 7; Caprini score, 0) No specific pharmacologic (Grade 1B) or mechanical (Grade 2C) prophylaxis be used other than early ambulation. Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients at low risk for VTE (~ 1.5%; Rogers score, 7-10; Caprini score, 1-2) Suggest mechanical prophylaxis, preferably with intermittent pneumatic compression (IPC), over no prophylaxis (Grade 2C). Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients at moderate risk for VTE (~ 3.0%; Rogers score, > 10; Caprini score, 3-4) who are not at high risk for major bleeding complications: Suggest LMWH (Grade 2B), LDUH (Grade 2B), or mechanical prophylaxis, preferably with IPC (Grade 2C), over no prophylaxis. Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients at moderate risk for VTE (3.0%; Rogers score, > 10; Caprini score, 3-4) who are at high risk for major bleeding complications or those in whom the consequences of bleeding are thought to be particularly severe Suggest mechanical prophylaxis, preferably with IPC, over no prophylaxis (Grade 2C). Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients at high risk for VTE (~ 6.0%; Caprini score, ≥ 5) who are not at high risk for major bleeding complications Recommend pharmacologic prophylaxis with LMWH (Grade 1B) or LDUH (Grade 1B) over no prophylaxis. Suggest that mechanical prophylaxis with elastic stockings or IPC should be added to pharmacologic prophylaxis (Grade 2C). Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For high-VTE-risk patients undergoing abdominal or pelvic surgery for cancer who are not otherwise at high risk for major bleeding complications Recommend extended-duration pharmacologic prophylaxis (4 weeks) with LMWH over limited-duration prophylaxis (Grade 1B). Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For high-VTE-risk general and abdominal-pelvic surgery patients who are at high risk for major bleeding complications or those in whom the consequences of bleeding are thought to be particularly severe We suggest use of mechanical prophylaxis, preferably with IPC, over no prophylaxis until the risk of bleeding diminishes and pharmacologic prophylaxis may be initiated (Grade 2C). Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients at high risk for VTE (6%; Caprini score, ≥ 5) in whom both LMWH and unfractionated heparin are contraindicated or unavailable and who are not at high risk for major bleeding complications Suggest low-dose aspirin (Grade 2C), fondaparinux (Grade 2C), or mechanical prophylaxis, preferably with IPC (Grade 2C), over no prophylaxis. Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients, we suggest that an inferior vena cava (IVC) filter should not be used for primary VTE prevention (Grade 2C). Patients Undergoing General, GI, Urologic, Gynecologic, Bariatric, Vascular, Plastic, or Reconstructive Surgery For general and abdominal-pelvic surgery patients, we suggest that periodic surveillance with venous compression ultrasound (VCU) should not be performed (Grade 2C). Major Trauma For major trauma patients, we suggest use of LDUH (Grade 2C), LMWH (Grade 2C), or mechanical prophylaxis, preferably with IPC (Grade 2C), over no prophylaxis. Patients With Major Trauma: Traumatic Brain Injury, Acute Spinal Injury, and Traumatic Spine Injury For major trauma patients at high risk for VTE (including those with acute spinal cord injury, traumatic brain injury, and spinal surgery for trauma), we suggest adding mechanical prophylaxis to pharmacologic prophylaxis (Grade 2C) when not contraindicated by lower extremity injury. Patients With Major Trauma: Traumatic Brain Injury, Acute Spinal Injury, and Traumatic Spine Injury For major trauma patients, we suggest that periodic surveillance with VCU should not be performed (Grade 2C). Major Trauma For major trauma patients in whom LMWH and LDUH are contraindicated, we suggest mechanical prophylaxis, preferably with IPC, over no prophylaxis (Grade 2C) when not contraindicated by lower-extremity injury. We suggest adding pharmacologic prophylaxis with either LMWH or LDUH when the risk of bleeding diminishes or the contraindication to heparin resolves (Grade 2C). Major Trauma For major trauma patients, we suggest that an IVC filter should not be used for primary VTE prevention (Grade 2C). Patients Undergoing Cardiac Surgery For cardiac surgery patients with an uncomplicated postoperative course, we suggest use of mechanical prophylaxis, preferably with optimally applied IPC, over either no prophylaxis (Grade 2C) or pharmacologic prophylaxis (Grade 2C). Patients Undergoing Cardiac Surgery For cardiac surgery patients whose hospital course is prolonged by one or more nonhemorrhagic surgical complications, we suggest adding pharmacologic prophylaxis with LDUH or LMWH to mechanical prophylaxis (Grade 2C). Patients Undergoing Thoracic Surgery For thoracic surgery patients at moderate risk for VTE who are not at high risk for perioperative bleeding, we suggest LDUH (Grade 2B), LMWH (Grade 2B), or mechanical prophylaxis with optimally applied IPC (Grade 2C) over no prophylaxis. Remarks: Three of the seven authors favored a strong (Grade 1B) recommendation in favor of LMWH or LDUH over no prophylaxis in this group. Patients Undergoing Thoracic Surgery For thoracic surgery patients at high risk for VTE who are not at high risk for perioperative bleeding, we suggest LDUH (Grade 1B) or LMWH (Grade 1B) over no prophylaxis. In addition, we suggest that mechanical prophylaxis with ES or IPC should be added to pharmacologic prophylaxis (Grade 2C). Patients Undergoing Thoracic Surgery For thoracic surgery patients who are at high risk for major bleeding, we suggest use of mechanical prophylaxis, preferably with optimally applied IPC, over no prophylaxis until the risk of bleeding diminishes and pharmacologic prophylaxis may be initiated (Grade 2C). Patients Undergoing Craniotomy For craniotomy patients, we suggest that mechanical prophylaxis, preferably with IPC, be used over no prophylaxis (Grade 2C) or pharmacologic prophylaxis (Grade 2C). Patients Undergoing Craniotomy For craniotomy patients at very high risk for VTE (eg, those undergoing craniotomy for malignant disease), we suggest adding pharmacologic prophylaxis to mechanical prophylaxis once adequate hemostasis is established and the risk of bleeding decreases (Grade 2C). Patients Undergoing Spinal Surgery For patients undergoing spinal surgery, we suggest mechanical prophylaxis, preferably with IPC, over no prophylaxis (Grade 2C), unfractionated heparin (Grade 2C), or LMWH (Grade 2C). Patients Undergoing Spinal Surgery For patients undergoing spinal surgery at high risk for VTE (including those with malignant disease or those undergoing surgery with a combined anterior-posterior approach), we suggest adding pharmacologic prophylaxis to mechanical prophylaxis once adequate hemostasis is established and the risk of bleeding decreases (Grade 2C). Endorsing Organizations This guideline has received the endorsement of the following organizations: • • • • • American Association for Clinical Chemistry American College of Clinical Pharmacy American Society of Health-System Pharmacists American Society of Hematology International Society of Thrombosis and Hemostasis Acknowledgement of Support The ACCP appreciates the support of the following organizations for some part of the guideline development process: Bayer Schering Pharma AG National Heart, Lung, and Blood Institute (Grant No.R13 HL104758) With educational grants from Bristol-Myers Squibb and Pfizer, Inc. Canyon Pharmaceuticals, and sanofi-aventis U.S. Although these organizations supported some portion of the development of the guidelines, they did not participate in any manner with the scope, panel selection, evidence review, development, manuscript writing, recommendation drafting or grading, voting, or review. Supporters did not see the guidelines until they were published.