POSTPARTAL NURSING
advertisement

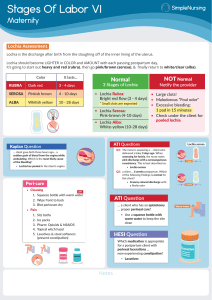
INTRODUCTION http://www.youtube.com/watch?v=qT H_-yIwevE POSTPARTAL NURSING Developed by D. Ann Currie, R.N. ,M.S.N. 2012 POSTPARTAL PERIOD PHYSICAL CHANGES PSYCHOSOCIAL CHANGES NURSING CARE OF THE POSTPARTAL CLIENT HIGH-RISK POSTPARTAL CLIENTS PHYSICAL CHANGES DURING THE POSTPARTAL PERIOD REPRODUCTIVE SYSTEM INVOLUTION-IS THE PROCESS OF THE REDUCTION IN SIZE OF THE UTERUS AFTER DELIVERY TO PREPREGNANT SIZE CAUSED BY UTERINE CONTRACTIONS THAT CONSTRICT AND OCCLUDE BLOOD VESSELS AT THE PLACENTA SITE FACTORS THAT ENHANCE INVOLUTION UNCOMPLICATED LABOR & DELIVERY BREASTFEEDING EARLY AMBULATION COMPLETE EXPLUSION OF PLACENTA AND MEMBRANES FACTORS THAT IMPEDE INVOLUTION PROLONGED LABOR & DIFFICULT DELIVERY ANESTHESIA GRAND MULTIPARITY RETAINED PLACENTAL FRAGMENTS OR MEMBRANES FULL URINARY BLADDER INFECTION CONT. OVERDISTENTION OF THE UTERUS USE OF OXYTOCIN DURING LABOR FUNDUS TOP PORTION OF THE UTERUS A PALPABLE INDICATOR OF INVOLUTION BOGGY UTERUSSOFT,RELAXED..CAN CAUSE HEMORRHAGE FUNDUS SHOULD BE FIRM Assessing Fundus FUNDUS LOCATION RIGHT AFTER DELIVERY THE FUNDUS IS MIDWAY BETWEEN SYMPHYSIS PUBIS AND UMBILICUS ONE HOUR AFTER DELIVERY THE FUNDUS RAISES TO THE UMBILICUS OR SLIGHTLY ABOVE1CM AND REMAINS THERE FOR 24 HRS. FUNDUS LOCATION- FUNDAL HEIGHT DECREASES 1CM A DAY AFTER THE FIRST 24 HR.. BY DAY 10 AFTER THE DELIVERY THE FUNDUS CAN NO LONGER BE FELT FUNDUS SHOULD BE MIDABDOMEN DEVIATIONS ARE ABNORMAL AND SHOULD BE CHECKED Deviation of Fundus Location LOCHIA IS THE DISCHARGE OF BLOOD AND DEBRIS FOLLOWING DELIVERY TYPES-RUBRA, SEROSA, AND ALBA SHOULD NOT CONTAIN LARGE CLOTS TOTAL VOLUME-240-270 ML. DAILY VOLUME GRADUALLY DECREASES LOCHIA AMOUNT MAY BE INCREASED BY EXCERTION OR BREASTFEEDING POOLING WHEN CLIENT IS RECLINING CAN OCCUR C/SECTION CLIENT MAY HAVE LESS BUT SHOULD HAVE LOCHIA UNEXPLAINED INCREASE IN AMOUNT IS ABNORMAL LOCHIA AMOUNTS LOCHIA RUBRA 1-3 DAYS AFTER DELIVERY DARK RED,BLOODY FLESHY,MUSTY ODOR CLOTS SMALLER THAN NICKEL BLOOD,MUCUS, SHREDS OF DECIDUA, EPITHELIAL CELLS LOCHIA SEROSA 4-10 DAYS AFTER DELIVERY PINK OR BROWNISH-WATERYODORLESS SERUM,ERYTHROCYTES,SHREDS OF DEGENERATING DECIDUA,LEUKOCYTES, CERVICAL MUCOUS,BACTERIA LOCHIA ALBA 11-21 DAYS AFTER DELIVERY MAY PERIST TO 6 WEEKS YELLOW TO WHITE- MAY HAVE STALE ODOR LEUKOCYTES,DECIDUA CELLS,EPITHELIAL CELLS,FAT, CERVICAL MUCUS, CHOLESTEROL, BACTERIA LOCHIA UNEXPLAINED INCREASE IN AMOUNT OR REAPPEARANCE OF LOCHIA RUBRA IS ABNORMAL.. AFTERPAINS CAUSED BY INERTMITTENT UTERINE CONTRACTIONS FOLLOWING DELIVERY OCCUR IN ALL WOMEN MORE PAINFUL IN MULTIPARIOUS AND BREASTFEEDING WOMAN ALSO IN WOMEN WHOSE UTERUS WAS OVERDISTENDED CERVIX SOFT,IRREGULAR,AND EDEMATOUS, MAYBE BRUISED AND/OR SMALL LACERATIONS CLOSES TO 2-3 CM AFTER SEVERAL DAYS..FINGERTIP AFTER 1 WEEK MUST BE SLIGHTLY DILATED TO ALLOW LOCHIA TO DRAIN AFTER FIRST DELIVERY SHAPE IS CHANGED VAGINA SMOOTH WALLS,EDEMATOUS WITH MULTIPLE SMALL LACERATIONS PERINEAL DISCOMFORT/PAIN SHOULD BE GONE BY 2 WEEKS AFTER DELIVERY LOW ESTROGEN LEVELS WILL TO DECREASED LUBRICATION FOR 610 WEEKS ABDOMINAL WALL SOFT & FLABBY WITH DECREASED MUSCLE TONE STRIAE(STRETCH MARKS) WILL FADE BUT STAY DIASTISIS RECTI-SEPERATION OF THE RECTUS MUSCLES OF THE ABDOMEN-MAY IMPROVE IN THE POSTPARTUM PERIOD CARDIOVASCULAR SYSTEM RETURNS TO PREPREGNANT STATE WITHIN 2 WEEKS THE ELIMINATION OF THE INCREASED BLOOD VOLUME DURING PREGNANCY IS DONE BY DIURESIS BLOOD PRESSURE SHOULD REMAIN STABLE CV SYSTEM -CONT. BRADYCARDIA BEGINS SECOND DAY-HR OF 50-70-CONT. FOR 6-10 DAYS TACHYCARDIA-BLOOD LOSS, TEMP.,OR OTHER PROBLEMS WBC’S ELEVATED IN POSTPARTUM PERIOD..LOOK FOR INCREASE OF OVER 30% IN 6 HRS. CV SYSTEM CONT. DECREASED HGB IS RELATED TO AMOUNT OF BLOOD LOSS 1ST 48 HRS POSTPARTUM ARE THE GREATEST RISK OF COMPLICATIONS FOR CLIENTS WITH HEART DISEASE RENAL SYSTEM INCREASED BLADDER CAPACITY AND DECREASED BLADDER TONE LEAD TO DECREASED SENSATION AND INCREASED RISK OF URINARY RETENTION AND INFECTION POSTPATAL DIURESIS-2000-3000 ML.-ACCOUNTS FOR 5 LB WEIGHT LOSS A FULL BLADDER WILL DISPLACE THE UTERUS RENAL SYSTEM FULL BLADDER CAN LEAD TO UTERINE ATONY AND PP HEMORRHAGE FLUIDS ARE ALSO LOST THROUGH DIAPHORESIS..COMMONLY SEEN AT NIGHT GASTROINTESTINAL SYSTEM HUNGER AND THRIST ARE COMMON FOLLOWING BIRTH OR IN THE 1ST PP DAY. CONSTIPATION-DECREASED PERISTALSIS, USE OF NARCOTIC ANALGESICS,DEHYDRATION, DECREASED MOBILITY DURING LABOR , AND FEAR OF PAIN GI SYSTEM CONT. HEMORRHOIDS-BECAUSE OF PRESSURE OF PUSHING DURING 2ND STAGE OF LABOR. Assessment for Hemorrhoids ENDOCRINE SYSTEM ESTROGEN AND PROGESTERONE LEVELS DROP RAPIDLY AFTER DELIVERY OF THE PLACENTA MENSTRUATION USUALLY RESUMES 7-9 WEEKS FOR NONLACTATING WOMEN- 90% BY 12 WEEKS-1ST CYCLE IS USUALLY ANOVULATORY ENDOCRINE CONT. OVULATION AND MENSTRUATION RETURN TIME IS PROLONGED WITH LACTATING WOMENDEPENDS WHETHER SHE IS SUPPLEMENTING WITH FORMULA-VARY 2 TO 18 MONTHS PLACENTAL HORMONES WHICH CAUSES INSULIN RESISTANCE WILL DECREASE BY 3-4 DAYS AFTER DELIVERY ENDOCRINE CONT. LACTATION COLOSTRUM/MILK PROLACTIN OXYTOCIN PSYCHOLOGICAL CHANGES IN THE POSTPARTAL PERIOD PHASES OF MATERNAL ADJUSTMENT PHASES OF PATERNAL ADJUSTMENT BONDING POSTPARTUM BLUES PHASES OF MATERNAL ADJUSTMENT TAKING-IN/DEPENDENT PHASETAKING-HOLD/DEPENDENTINDEPENDENT PHASELETTING-GO/INTERDEPENDENT PHASEDEVELOPMENTAL TASKMATERNAL ROLE ATTAINMENT 1ST DICUSSED BY R.RUBIN TAKING-IN DEPENDENT PHASE 1ST 1-3 DAYS..CAN BE SHORTEN PREOCCUPIED WITH OWN NEEDS PASSIVE AND DEPENDENT TOUCHES AND EXPLORES INFANT NEEDS TO DISCUSS LABOR & DELIVERY EXPERIENCE TAKING IN FOOD ,H2O,REST, AND CARE TAKING-HOLD DEPENEDENT-INDEPENDENT PHASE 3-10DAYS POSTPARTUM OBESSED WITH BODY FUNCTIONS RAPID MOOD SWINGS ANTICIPATE GUIDANCE MOST EFFECTIVE NOW…GOOD TIME TO TEACH INTERESTED IN LEARNING CARE OF BABY LETTING-GO INTERDEPENDENT PHASE 10 DAYS TO 6 WEEKS POSTPARTUM MOTHERING FUNCTIONS ESTABLISHED SEES INFANT AS A UNIQUE PERSON REESTABLISHES RELATIONSHIP WITH HUSBAND PATERNAL ROLE EXPECTATIONS REALITY TRANSITION TO MASTERY EXPECTATIONS 1ST STAGE THE FATHER HAS PRECONCEPTIONS ABOUT WHAT LIFE WILL BE LIKE AFTER THE BABY COMES HOME MAY NOT BE REALISTIC REALITY 2ND STAGE FATHER REALIZES THAT EXPECTATIONS ARE NOT ALWAYS BASED ON FACT COMMON FEELINGSSADNESS,AMBIVALENCE JEALOUSLY FRUSTATION REALITY OVERWHLMING DESIRE TO BE MORE INVOLVED SOME ARE PLEASANTLY SURPRISED AT EASE AND FUN OF PARENTING TRANSITION TO MASTERY 3RD STAGE FATHER MAKES CONSCIOUS DECISION TO TAKE CONTROL AND BECOME MORE ACTIVELY INVOLVED WITH INFANT BONDING FINGERTIPS,PALMS AND THEN ENFOLING OF INFANT EN FACE POSITION MOTHER USES A SOFT HIGHPITCHED TONE OF VOICE NURSE SHOULD ASSIST BOTH MOM AND DAD WITH BONDINGTIME/ISSUES Face to Face with Eye Contact POSTPARTUM BLUES A MATERNAL ADJUSTMENT REACTION TRANSIENT DEPRESSION USUALLY OCCURS BETWEEN 2ND-3RD PP DAY AND/OR WITHIN THE 1ST 2 WEEKS PP RELATED TO HORMONAL CHANGES,FATIGUE, AND STRESS ALL WOMEN EXPERIENCE IT PP BLUES CONT. CHARACTERIZED BY MOOD SWINGS,ANGER, TEARFULNESS, FEELINGS OF LETDOWN,ANOREXIA, AND SLEEING PROBLEMS USUALLY RESOLVES SPONTANEOUSLY IF CONT. OR WOMAN HAS DEEPENING DEPRESSION MAY HAVE PP DEPRESSION POSTPARTAL NURSING EVALUATE PRENATAL AND INTRANATAL HISTORY FOR RISK FACTORS POSTPARTUM ASSESSMENTBUBBLE-HEB-AND PREECLAMPSIA SCREENING VITAL SIGNS PP NURSING-CONT. PREVENTING PP HEMORRHAGE ASSESS FOR RISK FACTORS ASSESS FUNDUS & LOCHIA MASSAGE FUNDUS AS NEEDED KEEP BLADDER EMPTY ADMINSTER MEDICATIONS IF NEEDED-PITOCIN,METHERGINE ERGOTRATE CONT. PUT BABY TO BREAST EARLY AND FREQUENTLY `MONITOR VS COMFORT ICE TO PERINEUM 20 MINUTES ON/1O-2O MINUTES OFF-1ST 24 HRS SITZ BATHS-COOL OR WARM TID AFTER 12-24 HRS…MGSO4 CRYSTRALS PERICARE- AFTER USING BATHROOM OR PRN APPLY TOPICAL ANALGESICS- COMFORT TEACH CLIENT TO TIGHTEN BUTTOCKS THE SITTING…LAY ON SIDE ADMINSTER ANALGESICS KEGAL’S H2O,FIBER,& STOOL SOFTNERS,AMBULATE Kegal’s Exercise ELIMINATION BOWEL URINARY INFANT CARE SUCCESSFUL FEEDING BATHING SAFETY ADL’S POSITIONS FOLLOW UP VISITS SELF CARE NUTRITION REST COMFORT DISCOMFORTS ACTIVITIES F/U WARNING SIGNS CONTRACEPTION RHOGAM ASSESS RH NEG WOMAN NEG INDIRECT COOMBS RH POS BABY WITH NEG DIRECT COOMBS NO ALLERGIES TO GLOBULIN PREPARATIONS ADMINSTER 300UG IM WITHIN 72 HRS RUBELLA VACCINE RUBELLA TITER LESS THAN 1:8NONIMMUNE NO ALLERGY TO NEOMYCIN ADMINISTER O.5 ML SC PRIOR TO DISCHARGE CLIENT SHOULD NOT GET PREGNANT FOR 3-4 MONTHS NOT WITH RHOGAM PP WARNING SGNS BRIGHT RED BLEEDING MORE THAN 1 PAD/HOUR OR PASSING LARGE CLOTs TEMPERATURE GREATER THAN 100.4 F AFTER 1ST 24 HRS. CHILLS EXCESSIVE PAIN ANYWHERE REDDENED AREAS ON BREAST PP WARNING SIGNS REDDENED OR GAPING EPISIOTOMY FOUL SMELLING LOCHIA INABLE TO VOID..BURNING..ETC CALF PAIN, TENDERNESS,REDNESS, SWELLING FLU-LIKE S/S. Mastisis QUESTIONS THANK YOU http://www.youtube.com/watch?v=EE qj2BdVerg