Transfusions and the Age of Blood
advertisement

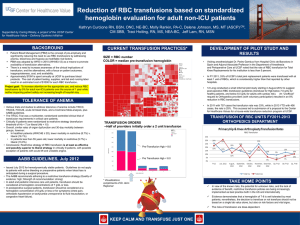
Is Fresh Blood better than Old Blood ? 1667 – Jean Baptiste Denis Early 1800’s First successful human-human transfusion 1900 – Karl Landsteiner Won the 1930 Nobel Peace Prize Isolated the A, B, & O blood types. Type AB blood was identified two years later. Recruit Transfuse blood Screen Donor Pretransfusion Testing Collect & Prepare Infections/disease tests Monitor & evaluate Medical Decision to transfuse Blood Safety Transfusion Safety Transfusion Safety in the Hospital Transfusion Sept 2003 P latelet Units T rans fus ed 300 273 Units T rans fus ed 250 200 164 167 150 100 95 50 0 2004 2005 2006 2007 Cost of Platelet Transfusions $140,000 $131,040 $120,000 $100,000 $80,000 $45,600 $60,000 $40,000 $20,000 $85,440 reduced cost $2004 2005 2006 2007 Red Blood Cells Problems with stored pRBC’s 1. Reduced ability of Hgb to release bound oxygen at tissue level (2,3 DPG) 2,3 DPG levels become undetectable after two weeks of storage. Levels are restored within 72 hours after transfusion Does red blood cell storage affect clinical outcome? When in doubt, do the experiment. Transfusion Vol 49 July 2009 Problems with stored pRBC’s 1. Reduced ability of Hgb to release bound oxygen at tissue level (2,3 DPG). 2. Reduced RBC deformability = potential to block capillary beds RBC squeezing through a capillary bed Problems with stored pRBC’s 1. Reduced ability of Hgb to release bound oxygen at tissue level (2,3 DPG).. 2. Reduced RBC deformability = potential to block capillary beds 3. Storage lesion (age dependent defect) = potential to block capillary beds MoreIsKnownAbout theRisksof BloodTransfusionThanthe Benefits! Problems with stored pRBC’s 1. Reduced ability of Hgb to release bound oxygen at tissue level (2,3 DPG) 2. Reduced RBC deformability = potential to block capillary beds 3. Storage lesion (age dependent defect) = potential to block capillary beds 4. Activation of recipients immune system Transfusions & Infection Each unit of blood increases the risk of a nosocomial infection by up to 50%! Transfusion increases the risk of postoperative infections after cardiovascular surgery J Am Coll Surg 2006 Jan;202 An alternative scoring system to predict risk for surgical site infection complicaating coronary artery bypass graft surgery Infect Control Hosp Epidemiol 2007 Oct; Transfusion of red cells is associated with increased incidence of bacterial infection after colorectal surgery; a prospective study Transfusion Feb 2003 Impact of allogenic packed red blood cell transfusion on nosocomial infection rates in the critically ill patient Crit Care Med 2002 Vol 30 #10 Transfusion Practice and Blood Stream Infections in Critically Ill Patients Chest 2005:127 Blood transfusions correlate with infections in trauma patients in a dose-dependant manner Am Surg 2002:68 838 ICU patients randomi zed into one of the following strategies: 1.Restrictive (transfusion for Hgb < 7g/dl) 2.Liberal (transfusion for Hgb < 10 g/dl) TRICC Trial Results Complication Restrictive Incidence Liberal Incidence All Cardiac morbidities 13.2% 21% Myocardial Infarction 0.7% 2.9% ARDS 7.7% 11.4% Pulmonary Edema 5.3% 10.7% 30 day Mortality 18.7% 23.3% A Multicenter, Randomized, Controlled Clinical Trial of Transfusion Requirements in Critical Care – Hebert et al New England Journal of Medicine 1999 Blood Transfusion Morbidity Study of 12,000 CAB patients at Cleveland Clinic Post-Op Complication Non-Transfused patients Transfused patients New onset of renal failure requiring dialysis 0% 1.81% Post-op ventilator support > 72 hours .44% 9.14% Serious post-op infection .24% 5.03% .05% 3.03% .37% 2.41% (includes sepsis and mediastinitis) Cardiac Morbidity (Includes Low Cardiac Index (< 1.8), high dose inotropic support > 4 hrs, post-op MI with IABP or VAD) Neurologic Morbidity Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting – Koch, et al. ,Critical Care Medicine 2006 Blood Transfusion Morbidity Study of 12,000 CAB patients at Cleveland Clinic “Transfusion is the single factor most reliably associated with increased postoperative morbid events. Each unit of red cells transfused is associated with incrementally increased risk for adverse outcome.” Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting – Koch, et al. ,Critical Care Medicine 2006 How low can we go? 10/30 Rule* First proposed in 1942 and based on studies that defined “peak” oxygen delivery in animals *Keep Hgb at 10gm and Hct at 30% 10/30 Rule* *Keep Hgb at 10gm and Hct at 30% How low can we go? • In animal studies, ECG ST segment changes are observed once Hgb falls below 5 g/dL • Both human and animal studies have demonstrated that Hgb’s < 3 g/dL are “maximally life-threatening.” Time course and etiology of death in patients with severe anemia Transfusion Vol 49 July 2009 Is Fresh Blood better than Old Blood ? 6,000 patients – 20,000 units of blood Compared “newer blood” (14 days or less of storage to “older blood” (>14 days of storage) HIGHER RATES OF: 1. Mortality 2. Prolonged ventilation 3. Renal Failure 4. Sepsis Duration of Red-Cell Storage and Complications after Cardiac Surgery 2008 The New England Journal of Medicine FDA Requirements 1.Hemolysis must be no greater than 1% at the end of storage, and 2.RBC recovery rates must be greater than 75% one day after transfusion Does the storage duration of blood products affect outcomes in critically ill patients Spinella et al, Transfusion August 2011 Altered parameters in Stored RBC Biochemical Metabolic Biomechanical Oxidative SNO-Hb ↓ RBC Storage Lesions Tatsuro Yoshida PhD Presentation to AABB Byproducts of Stored RBC’s 1.Released heme and iron from ruptured cells 2.Shed microvesicles 3.Loss of lipid and protein products from damaged RBC’s 4.Activated RBC adhesins Properties of stored red blood cells: understanding immune and vascular reactivity Spinella et.al Transfusion 2011 FDA Requirements Membrane fragments (lipids) shed from almost all cell types. They have been implicated in immune suppression. Byproducts of Stored RBC’s “All of these materials and activities are normal parts of the RBC life cycle, but they are concentrated in space and time by the RBC storage and transfusion process.” Properties of stored red blood cells: understanding immune and vascular reactivity Spinella et.al Transfusion 2011 “TWO-INSULT” Model Insult # 1 = Patient’s underlying inflammatory condition which “primes” the patient’s immune cells Insult # 2 = Full-on inflammatory activation triggered by a potential second insult, such as an allogeneic blood transfusion Properties of stored red blood cells: understanding immune and vascular reactivity Spinella et.al Transfusion 2011 Age of Blood Evaluation (ABLE) Trial 1.Canadian multicenter, randomized, controlled trial in the resuscitation of critically ill patients 2.Opened in 2008 – Anticipated end 2013 3.2,500 patients 4.Outcome measurements = 90 day mortality, MODS, infections, length of stay, Red Cell Storage Duration Study (RECESS) 1.NHLBI multicenter, randomized, controlled trial in cardiac surgery patients. Comparing blood stored <10 and >21 days. 2.Opened in 2010 – Anticipated end 2013 3.1,800 patients 4.Outcome measurements = 90 day mortality, MODS, major cardiac events, ventilation time, renal function, liver function. Age of Blood in Children in Pediatric Intensive Care Units (ABC - PICU) 1.Randomizing children to either a) blood less than 7 days old, or b) standard – issue RBC’s. 2.Opened in 2010 – Anticipated end 2013 3.1,500 patients 4.Outcome measurements = 28 day MODS, major cardiac events, ventilation time, renal function, liver function. So what do we do with all of this? Byproducts of Stored RBC’s 1.Released heme and iron from ruptured cells 2.Shed microvesicles 3.Loss of lipid and protein products from damaged RBC’s 4.Activated RBC adhesins Properties of stored red blood cells: understanding immune and vascular reactivity Spinella et.al Transfusion 2011 Transfusion. 2005 Aug;45(8):1295-301. Extracellular potassium concentrations in red blood cell suspensions after irradiation and washing. Weiskopf RB, Schnapp S, Rouine-Rapp K, Bostrom A, Toy P. J Trauma. 2006 Apr;60(4):851-8. Pulmonary endothelial permeability is increased by fluid from packed red blood cell units but not by fluid from clinically-available washed units. Rao RS, Howard CA, Teague TK. Transfus Apher Sci. 2008 Apr;38(2):141-7. Epub 2008 Mar 17. Stored packed red blood cells contain a procoagulant phospholipid reducible by leukodepletion filters and washing. Cardo LJ, Hmel P, Wilder D. Transfus Med. 2007 Apr;17(2):89-95. Processing of stored packed red blood cells using autotransfusion devices decreases potassium and microaggregates: a prospective, randomized, single-blinded in vitro study. Westphal-Varghese B, Erren M, Westphal M, Van Aken H, Ertmer C, Lange M, Booke M. Anesth Analg. 2002 Aug;95(2):324-5, table of contents. Intraoperative washing of long-stored packed red blood cells by using an autotransfusion device prevents hyperkalemia. Knichwitz G, Zahl M, Van Aken H, Semjonow A, Booke M. ASAIO J. 2007 Nov-Dec;53(6):680-3. The effect of preprocessing stored red blood cells on neonates undergoing corrective cardiac surgery. Liu J, Ji B, Feng Z, Zhao J, Li C, Li B, Long C. “Washing is associated with the loss of 10% to 20% of the red cells.” Blood Transfusion Therapy – A Physicians Handbook AABB 2005 REGULATORY ISSUES 1 Write a procedure 2. Get it signed by your doctors 3. Pick a QC marker 4. Measure (validate) what you are doing 5. Record your results. So what does this mean? So what does this mean? 1.Understand that transfusions may lead to worse outcomes. So what does this mean? 1.Understand that transfusions may lead to worse outcomes. 2. It is reasonable to infer that older stored blood may lead to worse outcomes! So what does this mean? 1.Understand that transfusions may lead to worse outcomes. 2. It is reasonable to infer that older stored blood may lead to worse outcomes! 3. Washing older stored blood may reduce morbidity.