HFH Management Recommendations BEFORE Brain Death
advertisement

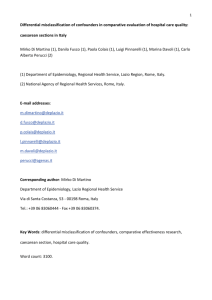
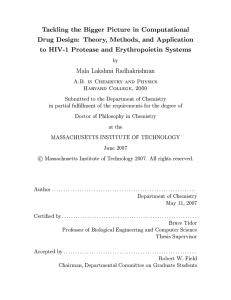
How to perform a BD exam and improve donor management Panayiotis N. Varelas, MD, PhD Director Neuro-ICU Senior Staff Neurology / Neurosurgery Henry Ford Hospital Associate Professor of Neurology Wayne State University Detroit, MI Topics for discussion • • • • Management before BD is declared How BD exam is performed How to approach the family Management after BD is declared I have received speaker honoraria and hold stock options Potential conflicts: from The Medicines Company, which has sponsored my research. I also receive royalties from the publication of the book Seizures in the ICU, I am an editorial board member of Neurocritical Care and serving in the advisory board of Gift of Life of Michigan. I have received speaker honoraria and holds stock options from The Medicines Company. The same company has sponsored research for which he served as primary investigator. He also receives royalties from the publication of the book Seizures in the ICU, is an editorial board member of Neurocritical Care and is serving in the advisory board of Gift of Life of Michigan. HFH Management Recommendations BEFORE BD Declaration HFH Management Recommendations BEFORE BD Declaration • These recommendations are to be discussed, agreed upon and ordered by the ICU Primary Team (Senior Staff) and collaboratively implemented by the ICU Primary team, Gift of Life representative, and ICU nursing. • These recommendations are not orders and should not be used as such. If a decision is made to utilize one or more of these recommendations, an order must be written by the physician. • Methods for attaining goals are just recommendations – they should not be used if they are contraindicated to the patient’s condition or contrary to patient’s /family’s advance directives HFH Management Recommendations BEFORE Brain Death Declaration • • MAP maintained ≥ 60 mmHg – Prevent Hypotension Keep CPP > 70, if an ICP monitor is in place – – – – – Maintenance IV Fluid: 0.9% NS with 20 mEq KCl @ 100-150ml/hr. (Saline may need to be adjusted for Na+ greater than 160, see below.) For hypovolemia: Bolus with 500mL 0.9% NS until MAP sustains ≥60 mmHg. Start Dopamine and titrate to maintain MAP ≥ 60 mmHg (max 20 mcg/kg/min). Always notify the physician when starting pressors or inotropes or transfusing blood products. If Dopamine is at 20 mcg/kg/min, CVP greater than 10, and MAP/CPP remains less than 60 mmHg, consider norepinephrine infusion. Titrate to clinical effect (max 20 mcg/min) If Hct ≤ 25%, recommend 1 unit of PRBC’s over 1 hour, repeat as necessary to maintain HCT ≥ 25% or hemoglobin > 7.0. HFH Management Recommendations BEFORE Brain Death Declaration • Hypertension – • Use IV Hydralazine prn. Avoid beta-blockers. Hypothermia – • Warming blanket to maintain core body temp between 36.5° – 37.2° C, except for pts with induced-hypothermia. Diabetes Insipidus (DI) – For urinary output greater than 4 mL/kg/hr X 2 hrs AND Na+ > 155 and rising, recommend Vasopressin drip or replace urine output mL/mL: If Na+ > 160, use Half NS (0.45%) for replacement If Na+ ≤ 160, use NS 0.9% for replacement Always notify the physician if pt hypotensive (CPP < 70, MAP < 60) or tachycardic (HR > 90) HFH Management Recommendations BEFORE Brain Death Declaration • Hypoxemia – – – – – – – Titrate FiO2 to maintain SaO2 greater than 98% or PaO2 > 300 on FiO2 1.00 Tidal Volume at 6 mL/kg Add PEEP of 5-8 cmH2o Rate adjusted to maintain normal pH (7.35-7.45) Suction and turn patient q 1-2 hrs Initiate Chest Percussion and Vibration q 1-2 hrs Albuterol Nebulizers: 2.5mg q 4 hrs. How to perform a BD exam? Current BD criteria in the US • Responsibility left to individual institutions: Each hospital has to develop its own criteria, based on • State laws criteria based on “accepted medical standards”, based on • President’s Commission (1981), Uniform Determination of Death Act (UDDA, 1993), AAN (2010) or other Societies recommendations, which are “advisory” and carrying the weight of “guidelines” rather than standards HFH: determination of brain death • Determination of “death by brain criteria” in accordance with MI law • Two different physicians, licensed in MI: 1) The primary senior staff physician 2) Senior staff from Neurology or NS or designated physician under direct supervision, i.e resident, fellow Determination of brain death - Process • GCS ≤ 5 GOL notified within 1 hour • If All prerequisites are met • Clinical evaluation: Cerebral unresponsiveness: deep, irreversible coma Absence of brainstem reflexes Absence of respiration (Apnea test) • ± Confirmatory testing Determination of brain death - Prerequisites • Established & sufficient cause of irreversible coma • Age 7 days • Exclusion of any complicating condition confounding clinical assessment: Absence of deep sedation or peripheral nerve or muscle dysfunction, i.e., (+) TOF, if NM blockade ToxScreen: ETOH < 80mg%, < 10g/ml, drugs? Temp-core 32.2oC (90oF) SBP 90 mmHg or MAP > 60 mm Hg or age-specific normotensive range in children Severe electrolyte, acid-base or endocrine disturbances Suspicion of drugs – toxins? • Administer antidotes • • • • Narcotics naloxone Benzodiazepines flumazenil Carbon monoxide oxygen Carbon disulfide, cyanide, hydrogen sulfide amyl nitrite • Declare brain death if traces of drug are found below therapeutic level • Unable to quantify drug/poison observe for x 5 half lives • Unknown, but high suspicion 48 hrs observation, if no confirmatory study Wijdicks Brain Death 2001 Pitfall: Effect of hypothermia on sedative metabolism Figure A shows the time course changes in concentration of Midazolam in brain-injured patients undergoing hypothermic therapy As shown in (A) concentration of the agent increased linearly until Body Temp reached 35 °C, after which the levels decrease profoundly when Body Temp rose to 36 °C, even during continuous administration of Midazolam. (B) Depicts the time course changes in concentration of Midazolam in brain-injured patients with normothermic therapy. In the figure, the concentration of the agent increased at 24 h after administration, then plateaued from 72 h, lasting until 216 h, during continuous infusion. Fukuoka et al, Resuscitation 2004 Clinical Examination - Coma • Lack of responsiveness to supraorbital nerve, nail-bed or TMJ pressure • Pitfalls: Uncoordinated, non-integrated into posturing responses = i.e. 2o to spinal cord reflexes Partial eye opening in response to ipsilateral nipple twisting 5 sec later (sympathetic fibers to Muller’s muscle?) (Santamaria et al., 1999) Clinical Examination - Reflexes • Mid-position (4-6 mm) or dilated pupils • Pitfalls: Drugs that influence pupils: Topical application of mydriatics Atropine in IV doses 0.03 mg/kg slight mydriasis, but (+) reaction to light (Goetting et al., 1991) Escalating doses of non-depolarizing paralytics lead from reversible to non-reversible mydriasis (Schmidt et al., 2000) Clinical Examination - Reflexes • Oculocephalic reflex (Cervico-occular, COR) • Cold calorics (VOR) • Pitfalls: or absent if: Toxic levels of aminoglycosides, tricyclics, anticholinergics, antiepileptics Orbital edema Battle’s sign (ipsilaterally) Clinical Examination - Reflexes • Corneal, blinking to threat • Grimacing to pain, jaw reflex Pitfall: facial myokymia/fibrillation from muscle denervation may mimic facial movements • Nasal tickle (V2 - XI) • Gag, cough • Over-breathing • Atropine test: tachycardia (↑ HR > 3%) to 2-3mg IV atropine (Huttemann et al., ICM 2000) Apnea test • • • • • Pre-admission or “normal” level for the pt Always with the second BD exam Pre-oxygenation 100% FiO2 PaCO2 target: 60 mmHg or [baseline + 20] PaCO2 by 3-6 mm Hg/min Hypothermia ( CO2 production, left shift O2 dissociation curve) normothermia • Hypotension SBP goal 90 mm Hg Apnea test - Solutions • Unable to complete the test?? CO2 augmentation (1 L/min) – PaCO2 > 60 mmHg within 2 min (Lang, 1995) Bulk diffusion (set rate = 0, CPAP = 0, 100% FiO2, 40-60 L/min continuous flow) - 22/24 pts completed the test repeat after correcting the problem clinical exam + confirmatory test use tricks: (al Jumah et al., 1992) T-piece (12 L/min) with CPAP valve (10 cm H2O) – less desaturation with T-piece compared to cannula inside ETT or T-piece alone (Levesque et al., CCM 2006) ADVICE: perform apnea test even if pt on high FiO2 and draw ABGs as O2 Sat reaches 90%! HFH: determination of brain death - Observation period between 2 clinical exams • Structural brain lesions: 2 Clinical exams 6 hours + apnea optional ConfTest • Catastrophic structural brain lesion: 1 exam + ConfTest (CBF test) + apnea • Ischemic/anoxic injury: 2 Clinical exams 24 hours + apnea optional ConfTest (for ex. if neuroimaging inconclusive) HFH: determination of brain death Observation period between 2 clinical exams (continue) • Children 1 year – 18 years: 2 Clinical exams 12 hours + apnea ( optional ConfTest) • Children 2 months – 1 year: 2 Clinical exams 24 hours + apnea + ConfTest • Neonates 7 days – 2 months: 2 Clinical exams 48 hours + apnea + ConfTest (2 EEGs 48 hours apart or CBF study, if equivocal) • Pregnant women: no BD exam or test, until confirmation of viability of fetus Confirmatory tests may be required • Confirmatory Tests “are recommended”: 1. Normal or inconclusive CTOH/MRI 2. COPD or sleep apnea- ? chronic PaCO2 3. Inconclusive or indeterminable apnea test 4. Children 5. Inability to perform full clinical exam 6. Severe facial trauma (ex. Racoon eyes) Relevant racoon eyes And NOT… Confirmatory tests may be required (continue) 7. 8. 9. 10. 11. 12. Preexistent abnormal/surgical pupil Severe cranial neuropathies Toxic/therapeutic level of CNS depressants, neuromuscular blocking agents, aminoglycosides, anticholinergics (?) complex/integrated motor activity Injury as a result of crime (not at HF!) If only one brain death exam is required (as @ Henry Ford!!) Electroretinogram 99mTc scintigraphy SPECT with 99mTc-HMPAO Clinical Questions 1. 2. 3. 4. 5. Are there patients who fulfill the clinical criteria of brain death who recover brain function? What is an adequate observation period to ensure that cessation of neurologic function is permanent? Are complex motor movements that falsely suggest retained brain function sometimes observed in brain death? What is the comparative safety of techniques for determining apnea? Are there new ancillary tests that accurately identify patients with brain death? BRAIN DEATH Approaching the family AND NOT DISCUSSING ABOUT DONATION!!! Consent rates • Average national consent rate 45-50% • Early referral when BD is imminent • Suitability for donation relies on OPO (Franz et al., 1997, DeJong et al., 1998) Consent rates • Factors improving donation rates: 1. Discussion in a quite environment 2. Trained requester (i.e., OPO) 3. Decoupling = family understands & accepts BD before any donation mentioned (Gortmaker et al., 1998) 4. Within 30 min after BD notification (because if simultaneous donation rate by 20-40% !) (Niles & Mattice, 1996) NICU Brain Death and Organ Donation Request Policy (Helms et al. Neurology 2004) • Donation was not discussed prior to brain death • Brain death declared according to hospital and AAN policies • Family informed and brain death process explained by treating attending physician • Physician does not bring up donation to family and leaves the room • Procurement coordinator (OPO) makes the request Organ and tissue donation consent rates 21 months before and 21 months after the institution of policy change (Helms et al. Neurology 2004) Before % After % Odds ratio, 95% CI p value Eye 17.1 30.8 1.5, 0.6-3.6 0.5 Bone & Tissue 10.4 37.3 5.1, 1.7-15.9 0.002* Solid organs 45.6 52.6 1.3, 0.5-3.1 0.7 Total 23.1 36.5 1.9, 1.15-3.15 0.01* Eye 16.5 14.2 0.8, 0.5-1.4 0.5 Bone & Tissue 27.1 29.3 1.1, 0.6-2.0 0.8 Solid organs 45.0 61.5 1.9, 0.6-6.4 0.4 Total 19.7 22.4 1.2, 0.9-1.7 0.3 NICU Other units Approaching the family 1. Let family know that the 1st BD is done and a 2nd will be performed at X time. 2. No mention about donation ! 3. If family asks about it, refer them to GOL 4. After the 2nd exam (or after the only BD exam), discuss again with family and explain the results and that the pt is irreversibly and legally dead. 5. Allow time for them to absorb the info, introduce GOL to them and then leave the room Approaching the family 6. If the family decides for donation and consent is signed GOL takes over Help GOL with tests, procedures 7. If the family decides against donation pt is disconnected from vent within 1 hour Time from declaration to VF- asystole Time (hours) to asystole No of patients <24 Jorgensen 1973 63 62% Mohandas and Chou 1971 25 56% Hicks and Torda 1979 25 80% 20% Narimazie 1980 10 60% 40% Jennett et al 1981 476 36% Ouaknine 1975 40 “Generally between 1 and 7 days” Kaste et al 1979 12 “On average 24 hours” Nishimura 1984 12 “On average six days” Goulon 1984 23 “Up to 128 hours” Study Kenneth Wood, DO, University of Wisconsin, 24-48 48-72 >72 25% 20% 31% 13% 16% 11% 8% 23% Pallis ABC of Brain Stem Death 1996 Medical management after BD • Integrative, multi-disciplinary and collaborative approach between OPO and Critical Care Team • Pre-BD management, aiming at brain function preservation, may compromise other organs and contradict the post-BD/donor management • Aggressive donor management may allow up to 84% of initially unsuitable donors to yield transplantable organs (Wheeldon et al., J Heart Lung Transpl 1995) Kenneth Wood, DO, University of Wisconsin Kenneth Wood, DO, University of Wisconsin Hemodynamic Effects of Sympathomimetics MAP PCWP CO SVR HR Dobutamine Dopamine – moderate 5-10 mcg/kg/min Dopamine – high > 10 mcg/kg/min Isoproterenol Norepinephrine Epinephrine CO – cardiac output; HR – heart rate; MAP – mean arterial pressure; PCWP – pulmonary capillary wedge pressure; SVR – systemic vascular resistance. Organ Donor - Heart Myocardial Dysfunction Sympathetic Surge Hormone Depletion • Myocardial necrosis secondary to catecholamines • Low circulating levels thyroid and cortisol impair function Subendo Ischemia • Decreased coronary perfusion pressure precipitates ischemia impairing myocardial function Kenneth Wood, DO, University of Wisconsin Changes in Ejection Fraction with Serial Echocardiograms (16) 100 90 Ejection Fraction 80 70 60 50 40 30 20 10 0 0 5 15 10 Time (hours) 20 25 30 Zaroff J Heart Lung Txp 2003; 22:383-388 Donor Management Assessment Brain dead patient (< 65 years old) Assess ventricular function by echocardiogram Ejection function 45% Norm al Pulmonary artery catheter placement Patient age Repeat echocardiography within 12 hours < 40 years > 40 years Normal Cardiac catheterization Normal Proceed to transplant Abnormal** Persistently abnormal* Consider dobutamine echocardiography (viability study) Reversible dysfunction No reversible dysfunction Not a donor Palac Prog Transplant 2003; 13:42-46 h Wood, DO, University of Wisconsin Hormonal Therapy (BD Animal Models) Pre- Treatment MYOCARDIAL Function ATP Creatine Phosphate Glycogen Lactate SYSTEMIC UTILIZATION Glucose Pyruvate Palmitate Lactate Free fatty acids Post Treatment Aerobic Anaerobic Anaerobic Aerobic Insulin Cortisol T3 Novitzky Cryobiology 1987; 24: 1-10 Novitzky Transplantation 1988; 45:32-36 Rescue Hormone Therapy If 10g/kg/min Vasoactive Support • 1 ampule 50% dextrose – 20 u insulin • 2 grams methylprednisolone • 20 g levothyroxine infusion 10 g/h PRE POST Vasopressor ug/kg/min 11.1 6.4 Heart rate beats/min 120 113 Oxygen consumption ml/min/m2 107 123 Oxygen extraction % 16 18 Salim Arch Surg 2001; 136:1377-80 Aggressive Pharmacologic – Hormonal Replacement Rosendale Transplantation 2003;75:482-487 Pulmonary Edema Ware & Matthay, NEJM 2005 Role of Brain Death in Donor Lung Injury Alvonitis Trasnaplantation 2003; 75:1928-1933 Neurogenic Pulmonary Edema • “Blast Injury Theory” → Hemodynamic mechanism Left • Sympathetic surge ↑ SVR ↓CO ↑LAP Right ↑ Pvc ↑ VR ↑PAP ↑Pul Volume • Transient massive ↑ of hydrostatic pressure with structural damage to pulmonary capillary endothelium • Sympathetic alteration of capillary permeability Inflammatory Response • Cytokines → TNF, IL-1 activate endothelial cells to express ICAM-1 and neutrophil migration to interstitium/alveolar spaces → release ROS and proteolytic enzymes Infection – atelectasis - hemo/pneumothorax • ALI/ARDS in 15-20% of severely brain-injured pts Neurogenic Pulmonary Edema in 11 chacma baboons ICP Autonomic Storm Catecholamine Excess Intense Vasoconstriction Right Circuit Left Circuit • Redistribution blood to RA/RV • SVR 537% • Adjustment to VR by COR • MAP 196% • PA flow 25% • Aortic flow 42% LV failure • mPAP (14 34mmHg) Exceeds for 1 minute • LAP (8-52mmHg) • Capillary blood flow arrest • Blood pooling -72% of total circ. volume in lungs • Blast injury-disruption of anatomic integrity of pulm capillaries Kenneth Wood, DO, University of Wisconsin Novitzky Ann Thorac Surg 1987; 43:288-294 Kenneth Wood, DO, University of Wisconsin Management of Respiratory Function in the Organ Donor Goals of mechanical ventilation FiO2: 0.40 PaO2 > 100 mmHg; or PaO2 > 300 on 100% FiO2 PaCO2: 30-35 mmHg Arterial pH, 7.35-7.45 Tidal volume: 10-12 ml/kg of predicted body weight PEEP: 5 cm of water Peak airway pressure: < 30 - 35 mm Hg CVP 6-8 mm Hg or PAWP 8-12 mm Hg Recruitment maneuver: prone or CPAP 40 cm H2O x 30 sec, repeated q 20 min x3 Kirschbaum & Hudson, Prog Transpl 2010 Management of Respiratory Function in the Organ Donor Goals of bronchoscopy Evaluate anatomy; Assess for foreign body and assist in removal Define and locate aspirated material or apparent infection; Clearance of secretions Goals of pulmonary hygiene Prevent atelectasis with the use of q 2-4 hr ETT & supraglottic suction, percussion, postural drainage and lung-expansion techniques; Bronchodilators; Paralytics Use of anti-infective & anti-inflammatory therapy Use of antibiotics based on results of Gram’s staining of aspirated secretions Methyl-prednisolone 15 mg/kg IV plus 15 mg/kg IV q 6 hrs Naloxone 8 mg IV to minimize Neurogenic Pulmonary Edema (?) Kirschbaum & Hudson, Prog Transpl 2010 • Retrospective, all potential donors within a 5-year period • 20 pts on ACV & 25 pts on APRV • ACV: RR 10-12 breaths/min, TV 5-10ml/kg, 40%, PEEP 5 • APRV: 6-10 breaths/min, inspir pressure 20-25 cm H2O and 40% Donated lungs: 7/40 (18%) in ACV vs 42/50 (84%) in APRV (p < 0.001) Partial pressure of arterial oxygen (PaO2)/fraction of inspired oxygen (FIO2) ratios on admission to the intensive care unit and following 100% oxygen challenge Hanna, K. et al. Arch Surg 2011;146:325-328. Management of Liver donors Increased recipient death or re-transplantation: • ABO incompatibility • High Na+ levels (> 155 mEq/L) • Long cold ischemia time • Large platelet transfusions • Prolonged recipient PTT Ploeg et al., Transplant 1993; Figueras et al., Transplant 1996; Kutsogiannis et al., Can J Anaesth 2006 Management of Kidney donors • + Immunomodulatory effects of catecholamines Low dose dopamine (< 10 g/kg/min) or epinephrine or vasopressin (< 0.04 U/min) • Colloids can be used (hydroxyethyl starch) • Avoid SBP < 80-90 mm Hg • Keep urine output > 1 ml/kg/hr • Avoid nephrotoxic drugs Deman at al., Nephrol Dial Transplant 1999; Dictus et al., Clin Transplant 2009 Intensivist-Led Management of Brain-Dead Donors Is Associated with an Increase in Organ Recovery for Transplantation In the before period, 66 out of 210 (33%) potentially available organs vs. 113 out of 258 (44%) potentially available organs in the after period, p = 0.008 Singbartl et al, Am J Transpl 2011 Island of KEA, Greece