PowerPoint プレゼンテーション
advertisement

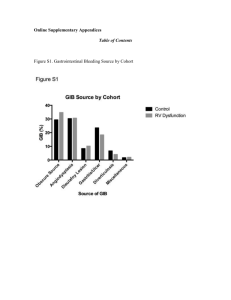
COMBINED USE OF TRANSPULMONARY THERMODILUTION (TPTD) TECHNIQUE IN FLUID MANAGEMENT FOR SEPSIS PATIENTS K. Morisawa1, M. Yanai1, Y. Takamatsu1, M. Takita1, S. Fujiwara1 B. Lohman1, J. Matsumoto1, S. Fujitani2, Y. Taira1 1 St. Marianna University School of Medicine, Kanagawa, Japan Department of Emergency and Critical Care Medicine 2 Tokyobay UrayasuIchikawa Medical Center, Chiba, Japan INTRODUCTION Treatment for sepsis requires proper fluid transfusion and monitoring of hemodynamic changes. The mainstay guidelines recommend CVP for fluid management. Fluid management with CVP monitoring may lead to excessive transfusion resulting in the following adverse reactions. TPTD is a technique that can estimate the global end-diastolic volume (GEDV) from the thermodilution curve. TPTD monitoring GEDV = Blood volume in the 4 chambers of the heart CV catheter Pulmonary circulation Blood temperature Thermodilution curve Bolus cold saline Bolus cold saline TPTD catheter measures the downstream temperature changes. TPTD catheter Systemic circulation at femoral artery Time CVP, central vein pressure; MV, mechanical ventilation; TPTD, transpulmonary thermodilution; GEDV, global end-diastolic volume PROTOCOL We assessed and compared the clinical outcome and total fluid balance between 2 groups of sepsis patients that were managed with TPTD and CVP respectively within 72 hours of admission to the ICU. TPTD group : using GEDI and SVV GEDI, global end-diastolic volume index calculated by the body surface area (mL/㎡) CVP group : based on the original EGDT Primary outcome : 28-day mortality Secondary outcome : ICU stay days : Mechanical ventilation days : Total volume balance YES NO Intubation and oxygenation for SpO2 ≥ 92 % Adequate volume resuscitation ? TPTD group CVP group GEDI 650 – 850 ? SVV < 15 % ? CVP 12 – 15 mmHg ? MAP 65 - 90 mmHg ? Volume infusion or reduction Norepinephrine or Nitroglycerin Hct > 30 % ? RBC transfusion ScvO2 ≥ 70 % ? Dobutamine Goal ? Adequate volume resuscitation Hct > 30 % ScvO2 ≥ 70 % Lactate < 4 mmol/L SpO2 ≥ 92 % MAP 65 - 90 mmHg Further treatment TPTD, transpulmonary thermodilution; CVP, central vein pressure; EGDT, early-goal directed therapy; GEDV, global end-diastolic volume; SVV, stroke volume variation PARTICIPANTS 23 severe sepsis and septic shock patients in the ICU Vasopressors and Mechanical ventilation September 2012 to August 2013 TPTD group (n = 11) CVP group (n = 12) P value Age 73 (10) 74 (9) ns Male [n(%)] 8 (73%) 6 (50%) ns SAPS II 53 (13) 56 (16) ns SOFA 11 (3) 10 (4) ns Pneumonia 4 5 Peritonitis 3 2 UTI 2 2 Others 2 3 Lactate 3.5 (2.9) 2.5 (1.8) Flow diagram 43 sepsis patients in study 20 patients excluded No vasopressors (n=3) Protocol deviation (n=9) No infection (n=4) Data deficiency (n=3) DNAR order (n=1) TPTD group (n = 11) CVP group (n = 12) [mmol/L] ns (Mean ± SD) TPTD, transpulmonary thermodilution; CVP, central vein pressure; SAPS II, simplified acute physiology score II SOFA, sequential organ assessment score; UTI, urinary tract infection RESULTS TPTD group (n = 11) CVP group (n = 12) P value 28-day mortality [n(%)] 2 (18) 4 (33) ns ICU stay days 6.3 (5.3) 8.8 (3.4) 0.01 MV days 4.2 (2.3) 5.6 (2.3) ns 0-24hr 2666 (1798) 5014 (3351) 0.02 24-48hr 69 (1095) 1889 (2120) 0.01 48-72hr 59 (648) 171 (1446) ns Total in 3 days 2885 (2678) 7074 (5248) 0.01 Volume balance[ml] TPTD, transpulmonary thermodilution; CVP, central vein pressure; MV, mechanical ventilation (Mean ± SD) CONCLUSIONS TPTD monitoring may help reduce any excess fluid transfusion. TPTD monitoring method may help shorten ICU hospitalization in patients with severe sepsis and septic shock. RCT is needing to validate our result. Multicenter RCT for this question is in process. (UMIN000011493)