In the name of god
First Trimester Screening
Dr.M.Moradi
First Trimester Screening
A method to identify women at risk for having an aneuploid fetus from the general population
Also can identify other birth defects such as congenital heart defects and diaphragmatic hernia
Performed during 11-14 weeks gestation
Patient Preferences and earlier diagnosis/ reassurance
All patients have a 2% to 3% risk of birth defects, regardless of their prior history, family history, maternal age, or lifestyle.
Chromosome abnormalities account for approximately 10% of birth defects.
A detailed fetal anatomic survey performed at 18 to 22 weeks remains the primary means for detecting the majority of serious ‘‘structural’’ birth defects.
first-trimester screening at 11 to 14 weeks has developed into the initial screening test for many patients.
The primary advantage of first trimester screening is earlier diagnosis of abnormalities (or early reassurance of the anxious patient), with the option of an earlier and safer pregnancy termination.
Advantages of 1st Trimester Screening
Information earlier, more options
Reduce number of invasive procedures
May identify other severe anomalies (or risk for) at time of scan and increased risk of adverse pregnancy outcome—referral for
2 nd Δ evals.
Good time to date pregnancy accurately
NT good for multiple gestation
First Trimester Screening
GOALS of this screen:
To increase sensitivity, decrease false-positive rates
To decrease number of
“unnecessary” invasive prenatal diagnosis tests.
NOT to increase number of elective abortions.
U/S measurements (NT) and free B-hCG, PAPP-A
Use of the guidelines proposed by the
Fetal Medicine Foundation have resulted in a high consistency in results
Nuchal translusency
History
◦ Dr.langdon Down 1866
◦ 1980s
◦ 1992…..prof Nicolaid….
Normal range?
Mechanism?
Normal Karyotype with increased NT
The mechanism for increased NT may vary with the underlying condition. The most likely causes include heart strain or
failure and abnormalities of lymphatic drainage . Evidence for heart strain includes the finding of increased levels of atrial and brain natriuretic peptide mRNA in fetal hearts among trisomic fetuses
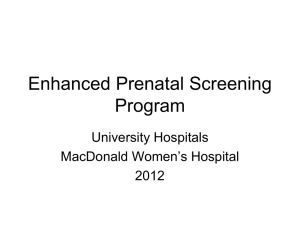
Nuchal Translucency
Measurements must be performed by certified individual!
True sagital
Position
Caliper
Separation of amnion magnification
The normal range for NT measurements is gestational age dependent. the median NT increases from 1.3
mm at a crown-rump length (CRL) of
38 mm to 1.9 mm at a CRL of 84 mm.
The 95th percentile increases from 2.2 mm at a crown rump length of 38 mm to 2.8 mm at a CRL of 84 mm.
The ability to measure NT and obtain reproduciblen results improves with training; good results are achieved after
80 and 100 scans for the transabdominal and the transvaginal routes, respectively
screening
Basic
◦ NT
◦ BIOCHEMISTRY
Advanced
The two most effective maternal serum markers currently used in the first trimester are pregnancyassociated plasma protein A (PAPPA) and free B-human chorionic gonadotrophin
(B-hCG).
Maternal serum free b-human chorionic gonadotropin (b-hCG) normally decreases with gestation after 10 weeks and maternal serum
PAPP-A levels normally increase.
Levels of these two proteins tend to be increased and decreased, respectively, in pregnancies affected by trisomy 21.
PAPP-A and Free BhCG
On average, baby with trisomy 21 will have 2.0 Mom for B-hCG and 0.4 MoM
PAPP-A
Basic screening
High risk 1/50
Moderate risk
Low risk 1/1ooo
Advanced
◦ Nasal bone
◦ Facial angle
◦ Ductus venosus
◦ Tricuspid regurgitation
Professor
Kypros
Nicolaides.
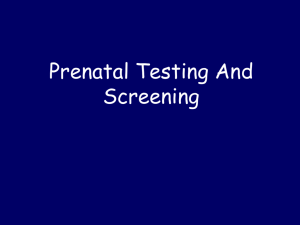
The fetal nasal bone can be visualized by sonography at
11–13+6 weeks of gestation
(Cicero et al 2001). Several studies have demonstrated a high association between absent nasal bone at 11–13+6 weeks and trisomy 21, as well as other chromosomal abnormalities.
Three line
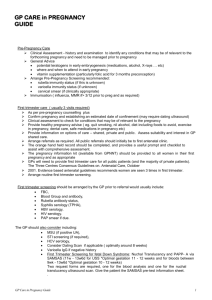
Fronto maxillary angle
GA dependent
CRL=45mm, 84’
CRL=84mm, 76’
Above 95% for age=increased risk of trisomy
Ductus venosus
Sample size
Angle
Filter sweep speed
Tricuspid regurgitation
Fetal heart rate
In normal pregnancy, the fetal heart rate
(FHR) increases from about 100 bpm at
5 weeks of gestation to 170 bpm at 10 weeks and then decreases to 155 bpm by
14 weeks. At 10–13+6 weeks, trisomy 13 and Turner syndrome are associated with tachycardia, whereas in trisomy 18 and triploidy there is fetal bradycardia (Figure
5; Liao et al 2001). In trisomy 21, there is a mild increase in FHR.
Urinary bladder
In first trimester
◦ >7mm=megacystitis
◦ 7-15 mm…..
◦ >15mm……
 0
0