Document
advertisement

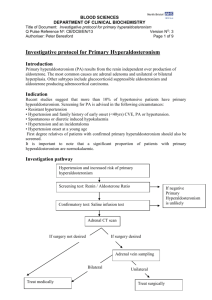
A Case From The Clinic Paul J. Scheel, Jr., MD Director Of Nephrology The Johns Hopkins University School of Medicine Patient W.T. • 56 year old AA male • Hypertension x 28 years • Hypokalemia past 2 years during annual physical. ( 2.8,3.1, 3.0) • Past Medical History : Negative • Past Surgical History: Absent Patient W.T. • Current Meds: – – – – Procardia XL 90 mg twice daily Amiloride 10 mg orally each day Metoprolol 100 mg twice daily Clonidine 0.2 three times daily Patient W.T. • Family History: Mother and Father both deceased ( 64,59) both with hypertension, One of 7 children all with hypertension • Social History: Recently retired from Federal Government. No Tob or Alcohol, No history of recreational drug use. • Review of Systems: Occasional fatigue and erectile dysfunction. Patient W.T. Physical Exam • • • • • • General: Appeared Well Vitals: BP 160/92, P 62, R 12 Wt 175 # HEENT: Normal Fundi Neck: No Bruits Back: No Buffalo Humping CV: Displaced PMI, S4, All peripheral pulses strong without bruits. • Abdomen: No masses No striae, No Bruits • Skin: No Echymoses Patient W.T. Labs 143 108 3.2 25 26 0.9 U/A: Dip negative , No Cells Hypertension and Hypokalemia Differential Diagnosis • Mineralocorticoid Excess – Hyperaldosteronism – Excess deoxycorticosterone • • • • Renal Vascular Disease Cushing’s Congenital Adrenal Hyperplasia Renin Secreting tumors When to Evaluate • Unexplained Hypokalemia ? • Severe, Resistant Hypertension or a Change in BP Pattern ? • Adrenal Incidentaloma • Physical Exam Suggestive of Excess Cortisol. • Hypertension Alone ? Incidence Of Hyperaldosteronism PAC/PRA > 30 Study Incidence N Gordon 9% 199 Lim 9.2% 465 Fardella 9.5% 305 Loh 18% 359 Comments Normal K + Primary Hyperaldosternoism Prevalence by JNC VI • I: BP 140-159/90-99 • II: BP 160-179/100109 • III BP > 180/>110 14 12 10 8 % PA 6 4 2 0 Normal Stage 2 Pathophysiology Na, K Circulating Blood Volume Renal Perfusion Pressure Aldosterone Release Angiotensin II Angiotensinogen Angiotensin I Renin Release Tubular Lumen Pathophysiology Na Peritubular Capillary 3Na 2K Aldosterone Receptor K Aldosterone Diagnosis • • • • Plasma Renin Activity Plasma Aldosterone Plasma Aldosterone: Renin Ratio 24 Hour Urine ( For What ?) Plasma Aldosterone: Renin • 8 am paired plasma Aldosterone + Renin • For Diagnosis of Hyperaldosteronism Plasma Aldosterone > 20 • Patients must be off Aldactone for 6 weeks • Calcium Channel Blockers, Alpha Blockers, Beta Blockers OK • ACEI : May falsely elevate renin Plasma Aldosterone : Renin • Interpretation of Results: – Normal - 4-10 – Hyperaldosteronism – 30-50 Must know lower limit of lab for plasma renin. Is is 0.6 or 0.1 ? May significantly affect ratios PAC/PRA • PAC > 20 and PAC/PRA > 30 – Sensitivity and Specificity of 90% for diagnosis of aldosterone producing adenoma 24 Hour Urine Collection • Historically used to document K+ Wasting • Now more useful to document other potential etiologies for low K + • 24 hour Urine should be sent for: – – – – K+ Na + Creatinine Aldosterone 24 Hour Urine Collection Results • In setting of hypokalemia – – – – – Inappropriate K + Wasting > 30 meq/day < 30 meq /day suggest extra renal losses Aldosterone > 14μg/day ( 39nmol/day) 24 hour urine sodium must be > 200 meq/day Must be accurate 24 hour collection (creatinine) • Woman 10-12 mg/kg body wt/24 hrs • Men: 12-15 mg/kg/body wt/24 hrs Hypertension and Hypokalemia Plasma Renin and Plasma Aldosterone PRA PRA PRA PAC PAC PAC Secondary Hyperaldosteronism Renovasular Disease Diuretic Use Renin Tumor Hyperaldosteronism Work Up CAH DOC-Tumor Cushings Syndrome Hyperaldosteronism Confirmatory Evaluation • Increased PAC:PRA • Confirmatory Testing Requires – High Sodium Diet followed by 24 hr urine OR – Saline Suppression Test with repeat of PAC:PRA OR – Fludrocortisone Suppression ( 0.2 mg b.i.d. x 2 days) Aldosterone level on day 3 > 5 confirmatory Hyperaldosteronism Classification • • • • Adrenal Hyperplasia Adrenal Adenoma Adrenal Carcinoma Familial Hyperaldosteronism I + II Radiologic Testing • CT or MRI – Unilateral Adrenal Mass > 5 cm Carcinoma – Can Identify Adenomas > 1 cm – Bilateral Abnormal Glands or Normal Bilateral Glands Suggest Hyperplasia Radiologic Testing • Adrenal Vein Sampling: – Selective Catheterization of Adrenal Veins – > 5x PAC From One Side Unilateral Disease – Must Also Measure After ACTH Stimulation Measuring both Aldosterone and Cortisol. – Cortisol Should be 10x Cortisol From Peripheral Vein Patient W.T • Plasma Aldosterone 25, PRA 0.63 Ratio 40 • Saline Suppression PAC 21, PRA 0.4 Ratio 52.5 • CT Scan: No abnormality • Dexamethasone Suppression PAC 17, PRA 0.4 , Ratio 42.5 Confirmed Hyperaldosteronism Negative CT Empiric Treatment Aldactone 100 mg- 200mg Adrenal Vein Sampling Medical Therapy • Aldactone: Usual therapeutic dose is 100200mg in divided doses per day. • Amiloride or Triamtene, ? Eplerenone • Lifestyle Modification – – – – – Ideal Body Wt Exercise Smoking Cessation Moderation of Alcohol Consumption Sodium Restriction ( < 100 mEq/day) Negative CT • Adenomas < 1 cm will be missed • Sensitivity compared to adrenal vein sampling with subsequent surgery and histologic confirmation of adenoma as low as 53 % . Confirmed Hyperaldosteronism Negative CT Empiric Treatment Aldactone 100 mg- 200mg Adrenal Vein Sampling Adrenalectomy Adrenal Vein Sampling Patient W.T. Aldosterone 39 ng/dl Aldosterone 3229 ng/dl Cortisol Cortisol 1062 mcg/dl 598 mcg/dl Confirmed Hyperaldosteronism Adrenal Adenoma Laparoscopic Adrenalectomy Adrenal Vein Sampling Medical Therapy Patient W.T. Patient W.T. • Patient Now 3 months S/p Adrenalectomy • Bp 127/71 on Atenolol 50 mg once daily Conclusions: • Hyperaldosteronism suspected in a patient with hypertension and unexplained hypokalemia or Severe Hypertension alone • Screen with PAC:PRA • Confirmatory Testing with Saline Suppression Test or Salt loading followed by 24 hr Urine. Conclusions: • CT or MRI can detect lesions > 1 cm • Normal CT or MRI does not rule out microadenoma • Adrenal Vein sampling is difficult to perform but is crucial to differentiating unilateral vs bilateral disease • Surgical Therapy = Adrenalectomy • Medical Therapy = Aldactone, ? Eplerenone