Case Presentation A 9 year old girl was brought with complaints of 1
advertisement

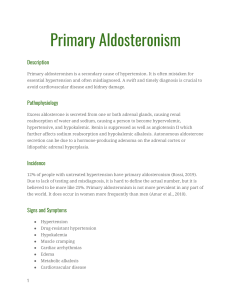
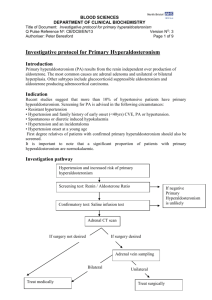
Case Presentation A 9 year old girl was brought with complaints of 1. Headache off & on- 1yr Dull ache, fixed, no photo or phonophobia, mainly in frontoparietal region. 2. Vomiting off & on- 1yr There was no h/o excessive sweating / palpitations / flushing/ heat intolerance/ blurring of vision/ altered sensorium/ seizures/ weakness in any limbs No h/o fever/ decreased urine output/ hematuria/ recurrent UTI/ polyuria/ polydypsia/ excessive weight gain/loss. Past history was suggestive of one episode of UTI and frequent coughs and colds. Family history of Hypertension was positive in paternal grandmother (at age of 55) and maternal uncle (at age of 35). There was no history of coronary artery disease, stroke or unexplained sudden deaths in the family. The anthropometry of the child was as follows: Weight: 30kg (50th %ile) Height : 136cm (75th %ile) BMI : 16.6 Vitals: HR: 110/m, good volume, regular BP measurement: RUL-156/100 LUL-161/99 (mm Hg) RLL- 161/99 LLL- 167/108 percentile BP 50th 90Th 95Th 99Th SBP 102 114 118 125 DBP 60 74 78 85 General exam- pallor +ve No skin pigmentation SMR- Stage 1 Fundus- generalized collateral arterioles, no retinal hemorrhage, optic disc normal Systemic examination was within normal limits. On the basis of history and examination, the patient was diagnosed as a case of Hypertensive urgency (Stage 2 HTN without target organ damage). Now, the cause of Hypertension needed to be worked up. The common Differential diagnosis for Persistent Hypertension like - Renal Parenchymal disease - Renovascular disease - Cardiovascular disease - Endocrine disorders were considered and work up begun on these lines. Following is a summary of the Investigations done: CBC/ESR/CRP : wnl Renal causes: • KFT with electrolyte- Persistent Hypokalemia • Blood gas done multiple times- WNL • Urine R/M- WNL • Urine culture- NG • USG KUB- Obscured corticomedullary differentiation S/O medico renal disease • Urine spot protein/creatinine ratio s/o Microalbuminuria (111mg albumin/gm of creatinine) • Xray chest- normal • DMSA scan– WNL • S/O aberrant artery to right lower pole rest with Renal doppler followed by CT angiography of abdomen- in normal limit. Cardiovascular causes: • Echocardiography normal • Lipid profile normal Others: • • cANCA / pANCA /ANA/ complement C3/C4 /DsDNA Negative Thyroid functions normal Meanwhile we were faced with the problem of persistent hypertension and hypokalemia that was difficult to manage and refractory to treatment despite iv and oral potassium supplementation and 3 antihypertensive drugs (Metoproplol, Amlodepine and Enalapril). Next step was the evaluation of endocrine causes of persistent hypertension and determination of the urinary potassium losses. The results were as follows: Endocrine: • • • • • Plasma Renin activity- 0.11ng/ml/hr (low) (supine- 0.5-1.9, upright- 1.9-6) Plasma Aldosterone- 868.1pg/ml (12-340pg/ml) =8.68ng/dl (High) Cortisol - WNL Aldosterone /Renin ration(ARR)- 80 (20) (High) CECT abdomen: wnl Urinary Potassium losses were evaluated by using the Transtubular Potassium Gradient (TTKG) TTKG- K(U)/K(S) x( pl osmolality/U Osmolality) (27.8/2.6) x (284/307)= 9.74 (Renal loss is indicated when TTKG >4 in cases of hypokalemia) The patient was then started on Aldactone, following which the BP fell below the 99th %ile (120/80) and gradually all other antihypertensives were discontinued except Aldactone (37.5mg B.D) and Amlodepine (5mg BD). Her serum potassium also improved but were still low (3.0 mg/dl). At this stage, a diagnosis of Stage II Hypertension secondary to Primary Hyperaldosteronism was made. She was investigated further for the type of primary hyperaldosteronism using the Dexamethasone Suppression Test to rule out Glucorticoid remediable Hypertension (GRA). The results of the test are as follows: PRA- 0.15ng/ml/hr, Aldosterone -0.056ng/dl Genetic testing for GRA was also sent. The patient’s management was now modified with addition of Prednisolone (5mg) to the ongoing Aldactone and Amlodepine. With this, her BP fell below the 90th %ile (110/76mm Hg) and serum potassium increased to 4.0 mg/dl. DISCUSSION: Hypokalemia is a common clinical problem.The kidney is responsible for long term potassium homoeostasis, as well as the serum potassium concentration.The main nephron site where K secretion is regulated is the cortical collecting duct, mainly via the effects of aldosterone. Aldosterone interacts with the mineralocorticoid receptor to increase sodium reabsorption and potassium secretion. The cause of hypokalemia can usually be determined from the history. If there is no apparent cause, the initial step is to see if hypokalemia is associated with systemic hypertension or not. In normotensive patients, hypokalaemia could be secondary to overt or occult gastrointestinal loss or due to renal potassium wasting. Hypertension and Hypokalemia Plasma Renin and Plasma Aldosterone PRA PRA PRA PAC PAC PAC Secondary Hyperaldosteronism Renovasular Disease Diuretic Use Renin Tumor Hyperaldosteronism Work Up CAH DOC-Tumor Cushings Syndrome Primary hyperaldosteronism, should be suspected as a cause of hypertension in the following conditions: 1. Hypertension and unexplained persistent hypokalemia or diuretic-induced hypokalemia 2. Severe hypertension, stage 2 hypertension. 3. Patients with difficult to- control hypertension requiring three or more drugs 4. When hypertension manifests at a young age (<20 years) 5. When adrenal incidentaloma is present 6. Whenever an evaluation for secondary hypertension is considered 7. Hypertensive relatives of patients with PA. Primary aldosteronism occurs in at least 5-9% of the cases of essential hypertension and is the most frequent cause of secondary hypertension in adults. Also patients with primary aldosteronism display an increased prevalence of cardiovascular events as compared to essential hypertensives. Familial forms of PA include – Familial hyperaldosteronism type 1 (FH-1) or Glucocorticoid-Remediable Aldosteronism (GRA) – FH-2 (familial occurrence of bilateral adrenal hyperplasia, adrenal adenoma or both). The aldosterone renin ratio (ARR) has become the most widespread method of screening. Cut-off values of the ARR 20 ng/dL per ng/mL per hour(554 pmol/L per ng/mL per hour) in combination with a plasma aldosterone level 15ng/dL (416 pmol/L) in a morning blood sample from an ambulant patient with normokalemia is indicative of primary aldosteronism. Once an abnormal ARR is seen then confirmatory test should be performed. Confirmatory tests include Intravenous saline loading, Oral sodium loading, Fludrocortisone suppression test (FST) and Captopril suppression test (CST). HRCT/ MRI of adrenal is recommended in biochemically confirmed case. Glucocorticoid Remediable Hypertension (GRA) It is an autosomally dominantly inherited codition caused by a chimeric gene resulting from cross – over of promoter sequences between the CYP11B1 and CYP11B2 genes that are involved in glucocorticoid and mineral corticoid synthesis, respectively. This rearrangement brings CYP11B2 under the control of ACTH receptor signaling; consequently, aldosterone production is regulated by ACTH rather than by renin. This is a rare example of a hormone – over producing, syndrome without an increase in the number of cells making the hormone. Normally, angiotensin II stimulates aldosterone production by the adrenal zona glomerulosa, whereas ACTH stimulates cortisol production in the zona fasciculate. Owing to chimeric gene on chromosome 8, mineralocorticoid production is regulated by corticotropin instead of by the normal secretagogue, angiotensin II in these patients. Therefore, aldosterone secretion can be suppressed by glucocorticoid therapy. In the absence of glucocorticoid therapy, this mutation results in overproduction of aldosterone and the hybrid steroids 18 – hydroxycorticsol and 18- oxycortisol, which can be measured in the urine (20-30 times normal in these patients) to make the diagnosis. Clinically GRA presents with early onset HT, with the mean age of onset being 13 years. HT is moderate to severe in most cases but can be mild or normal depending on the hereditary factors controlling HT and dietary salt intake. Hence, a positive family history is always not forthcoming. Patients with GRA are more prone to develop cerebrovascular accidents, especially fatal cerebral hemorrhage from rupture of intracranial aneurysms. Left ventricular wall changes are also common, indicating excess of aldosterone in the blood and may be independent of the degree of HT. Growth is typically not affected in children with GRA unlike Apparent Mineralcorticoid excess (AME) and congenital Adrenal hyperplasia (CAH). The Dexamethasone suppression test (DST) should be used in patients with biochemical primary hyperaldosteronism, who have a suggestive clinical history, and negative CT imaging of the adrenals. This must always be followed by specific genetic testing. FH type II is also autosomal dominant and may be monogenic. The hyperaldosteronism in FH type II does not suppress with dexamethasone, and GRA mutation testing is negative. FH type II is more common that FH type I, but it still accounts for fewer than 2% of all patients with primary aldosteronism. Patients with GRA are managed with low doses of glucocorticoids to suppress the pituitary ACTH secretion. The steroid dose should be titrated against the blood pressure and maintained as low as possible to achieve adequate control. Addition of aldosterone antagonists like spironoactone is sometimes required when prednisolone alone is not effective in reducing BP. Screening with MR angiography, beginning at puberty and then every five years, has been recommended to detect asymptomatic intra-cranial aneurysms in these patients. What we hope to learn from this case is: • Take BP…in all chronic headache . • Family history to be asked in detail esp age of onset. • Limited diagnosis of hypokalemia with hypertension. • Knowing the values in unit and method of collection of sample is important. • Send sample before starting AHT. • Whenever using more than 3 antihypertensives, revise and dig deep for etiology. • .Investigate for possible diagnosis of primary hyperaldosteronism..as treatment options are variable. • To use the Plasma ARR (Aldosterone Renin Ration) in possible cases of primary aldosteronism • Get all young hypertensives checked for primary hyperaldosteronism before labeling them as essential hypertension.