Advanced Practice Nursing in Acute and Critical Care Environments
advertisement

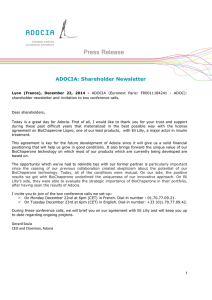
New Paradigms, Guidelines, and Evolving Strategies Achieving A1C and Glycemic Targets with Insulin What to Do When Oral Agents Fail JUAN P. FRIAS, M.D., FACE Assistant Clinical Professor of Medicine University of California San Diego San Diego, CA ADA/EASD: Managing Hyperglycemia in Type 2 Diabetes Initial Monotherapy Healthy Eating, Increased Physical Activity, Weight Control Metformin Efficacy (A1C) Hypoglycemia Weight Side effects Cost High Low risk Neutral/loss GI/lactic acidosis Low Two Drug Combo. A1C target not achieved after 3 months, proceed to 2-drug combo. Metformin + (order does not denote specific preference) SFU TZD DPP-4 Inhib. GLP-1 RA Insulin (usually basal) Efficacy (A1C) Hypoglycemia Weight Side effects Cost Three Drug Combo. High Mod. risk Gain Hypo. Low High Low risk Gain Edema, HF, fx High Intermediate Low risk Neutral Rare High High Low risk Loss GI High Highest High risk Gain Hypo. Variable A1C target not met after 3 months, proceed to 3-drug combo. (order does not denote specific preference) Adapted from, Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] ADA/EASD: Managing Hyperglycemia in Type 2 Diabetes Three Drug Combo. A1C target not met after 3 months, proceed to 3-drug combo. (order does not denote specific preference) MET + SFU + MET + MET + TZD + DPP-4 Inh. + MET + GLP-1 RA + MET + Insulin (usually basal) • TZD, or • DPP-4-I, or • GLP-1 RA, or • Insulin • SFU or • DPP-4-I, or • GLP-1 RA, or • Insulin • SFU, or • TZD, or • Insulin • SFU, or • TZD, or • Insulin + • TZD or • DPP-4-I, or • GLP-1 RA If combination therapy that includes basal insulin has failed to achieve A1C target after 3-6 months, proceed to a more complex insulin strategy, usually in combination with 1-2 non-insulin agents More Complex Insulin Strategies Insulin Multiple daily doses Adapted from, Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] Case #1 ► 55 year old woman with 8-year history of type 2 diabetes ► For last 2 years, has taken metformin 1000 mg bid, pioglitazone 45 mg qd, and glimepiride 4 mg qd ● Seen 4 months ago: A1C 8.0%, BP 130/80, and LDL Cholesterol 125 mg/dL ● Added atorvastatin 20 mg qd, told to intensify diet and exercise ► Weight 215 lbs (6 lb gain since last visit), height 5’ 5”, BMI 36 kg/m2 ► Fasting plasma glucose in the office = 196 mg/dL ► Current A1C = 8.8% Question #1 What do you do now? 1) Start a GLP-1 receptor agonist 2) Start a DPP-4 inhibitor 3) Add insulin 4) Reinforce efforts at better nutrition and increased physical activity Idealized Profiles of Human Insulin and Insulin Analogs Rapid-acting: lispro, aspart, glulisine Regular insulin NPH Insulin detemir Plasma Insulin Concentration Insulin glargine 0:00 2:00 4:00 6:00 8:00 10:00 12:00 14:00 16:00 18:00 20:00 22:00 24:00 Time Rosenstock J. Goldstein BJ et al, eds. Textbook of Type 2 Diabetes. Martin Dunitz;2003:131-154. Plank J et al. Diabetes Care. 2005;28:1107-1112. Consistent Results Using the Treat-to-Target Method with Glargine as Basal Insulin Baseline Study end 9.5 9.0 8.6 8.8 8.7 8.6 8.7 8.5 A1C % 8.0 ∆ -1.6 ∆ -1.6 ∆ -1.7 ∆ -2.0 ∆ -1.7 7.5 7.0 7.0 7.0 7.0 6.8 7.0 6.5 6.0 5.5 T-T-T1 INSIGHT2 APOLLO3 INITIATE4 Schreiber5 n = 367 n = 206 n = 174 n = 58 n = 12,216 1. Riddle M et al. Diabetes Care 2003;26:3080 2. Gerstein HC et al. Diabetes Med 2006;23:736 3. Bretzel RG et al. Lancet 2008;371:1073 4. Yki-Järvinen H et al. Diabetes Care 2007;30:1364 5. Schreiber SA et al. Diabetes Obes Metab 2007;9:31 Insulin Dosage and FPG During Study 50 40 206 36 30 31 28 175 37 39 44 43 41 200 33 25 20 153 16 150 142 10 135 135 128 125 10 121 118 117 116 0 100 0* 2 4 6 8 10 12 14 Weeks in Study Mean insulin dose 0.45 U/kg *Week 0 based on a starting dose of 10 units Riddle M, Rosenstock J, and Gerich, J. Diabetes Care. 2003;26(11)3080-3086. 16 24 Mean FPG mg/dL (± SE) Total Daily Dose, Units (± SE) (Both Treatment Groups) Events per patient exposure–year Symptomatic Hypoglycemic Events 1.4 * * 1.2 NPH Insulin glargine * * 1.0 * * Basal insulin 0.8 * 0.6 0.4 0.2 Breakfast Lunch Dinner 0 20 22 24 2 4 6 8 10 12 Time of day (h) Hypoglycaemia defined as plasma glucose 72 mg/dL *P<0.05 vs insulin glargine Adapted from Riddle M, et al. Diabetes Care. 2003;26:3080-3086. Used with permission. 14 16 18 Detemir vs NPH Insulin in Type 2 Diabetes (n=476) Detemir NPH 10.0 Detemir NPH 9.0 8.0 7.0 6.0 Hypoglycemia Events* 400 A1C (%) 350 300 250 200 150 100 50 0 -2 0 4 8 12 16 20 24 Study Week 024 8 12 16 20 24 Study Week *All reported events, including symptoms only. Hermansen K et al. Diabetes Care. 2006;29:1269-1274. Percentage of Patients Reaching Target A1C at Week 24 by Baseline A1C Baseline A1C Group n Mean Baseline A1C 581 436 360 327 608 7.6 8.2 8.7 9.2 10.2 Riddle M et al. ADA abstract 468-P. Diabetes. 2009;58(suppl 1):A125. Exenatide QW Resulted in Superior A1C Reduction vs. Insulin Glargine Exenatide QW, N=233; baseline A1C=8.3% Insulin glargine, N=223; baseline A1C=8.3% 0.0 Change in A1C (%) -0.2 -0.4 -0.6 -0.8 -1.0 * -1.2 -1.3% -1.4 -1.6 * * * 14 18 22 * -1.8 0 8 Time (weeks) ITT Population, N=456. *p<0.05 Diamant M, et al. Lancet. 2010;375:2234-43. 26 -1.5% Exenatide QW Resulted in Superior Body Weight Reduction vs. Insulin Glargine Exenatide QW, N=233; baseline weight=91 kg Insulin glargine, N=223; baseline weight=91 kg Change in Body Weight (kg) 2 +1.4 kg 1 0 * -1 * -2 * * -3 012 4 8 14 18 Time (weeks) ITT Population, N=456. *p<0.05 Diamant M, et al. Lancet. 2010;375:2234-43. * 22 -2.6 kg * 26 Case #1 (cont.) ► 20 U insulin glargine (~0.2 U/kg) is added to her oral agents ► Sent home with instructions to increase dose by 2U every 3 days until FBG in 100-120 mg/dL range ► Call if any hypoglycemia and follow-up by phone or in clinic in 1 week Should you reduce or stop one of the oral agents? Riddle MC et al. Diabetes Care. 2003;26:3080-3086. Hermansen K et al. Diabetes Care. 2006;29:1259-1271. Nathan DM, et al. Diabetes Care 2009;32:193–203. Case #1 (cont.) ► Patient is up to 52 U with fasting blood glucose controlled (100-110 mg/dL range) since her last visit 4 months ago ► A1C = 6.7%, monitoring occasional postprandial blood glucose ► Patient finds insulin injections painless and after working with diabetes educator, feels that she is now a partner in her own therapy “Fix the Fasting First” ► Even if you are not certain basal insulin alone will achieve target A1C (e.g. patient with A1C >10%), it is generally preferable to begin with it & add a rapid-acting analog with the largest meal, if needed. ► It is easier for the HCP & patient to see which insulin needs to be adjusted Basal Insulin Therapy ► Usual first step in beginning insulin therapy ► Continue oral agents and add basal insulin to optimize FPG ► A1C of up to 9.0% usually brought to goal (7%) by addition of basal insulin therapy to oral agents ► Easy and generally safe: patient-directed treatment algorithms with small risk of serious hypoglycemia ► ADA and EASD: ”If triple combination therapy exclusive of insulin is tried, the patient should be monitored closely, with the approach promptly reconsidered if it proves unsuccessful” ADA=American Diabetes Association; EASD=European Association for the Study of Diabetes. ADA/EASD Management of hyperglycemia in type 2 diabetes: A patient-centered approach. 19 April 2012 [Epub ahead of print] New Paradigms, Guidelines, and Evolving Strategies Case Presentation #2: Strategies for Advancing to Postprandial Glucose Control ADA/EASD: Managing Hyperglycemia in Type 2 Diabetes Three Drug Combo. A1C target not met after 3 months, proceed to 3-drug combo. (order does not denote specific preference) MET + SFU + MET + MET + TZD + DPP-4 Inh. + MET + GLP-1 RA + MET + Insulin (usually basal) • TZD, or • DPP-4-I, or • GLP-1 RA, or • Insulin • SFU or • DPP-4-I, or • GLP-1 RA, or • Insulin • SFU, or • TZD, or • Insulin • SFU, or • TZD, or • Insulin + • TZD or • DPP-4-I, or • GLP-1 RA If combination therapy that includes basal insulin has failed to achieve A1C target after 3-6 months, proceed to a more complex insulin strategy, usually in combination with 1-2 non-insulin agents More Complex Insulin Strategies Insulin Multiple daily doses Adapted from, Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] Sequential Insulin Strategies in Type 2 Diabetes Non-Insulin Regimen Number Complexity of of injections regimen Basal Insulin only 1 Low 2 Mod 3+ High (usually with oral agents) Basal insulin + 1 (mealtime) rapid-acting insulin injection Pre-mixed insulin twice daily Basal insulin + ≥2 (mealtime) rapid-acting insulin injection More Flexible Less Flexible Adapted from, Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] Case #2 ► 50-year-old man with 6-year history of type 2 diabetes ► 295 lb, 6’ 1”, BMI 39 kg/m2 ► For last 2 years, has taken metformin 1000 mg bid and glimepiride 8 mg qd ► 3 months ago, A1C 9.2% ► Started a twice-daily premixed analog insulin (70/30); current dose 40 U bid Case #2 (cont.) ► Current A1C 7.5% and random plasma glucose in the office 185 mg/dL ► Patient experiencing nighttime hypoglycemia (reports middle-of-night sweating) ► SMBG diary focused on fasting glucose ► Patient instructed to measure glucose before meals, at bedtime, and during night for a week Case #2 (cont.) Question #2 Patient’s A1C is 7.5% and SMBG diary reveals high fasting and post-dinner glucose, and nocturnal hypoglycemia. The next step for this patient to gain control is to: 1) Continue with the twice-daily premix and increase dose 2) Continue with premixed and discontinue glimepiride 3) Switch to a long-acting insulin analog alone 4) Basal insulin + GLP-1 receptor agonist 5) Switch to a basal-bolus insulin regimen Basal/Bolus Treatment Program With Rapid-acting and Long-acting Analogs Breakfast Lunch Aspart Aspart Aspart Lispro Lispro Lispro or or or Plasma Insulin Dinner Glulisine or Glulisine or or Glulisine Glargine or Detemir 4:00 8:00 12:00 16:00 Time 20:00 24:00 4:00 8:00 “All to Target” Trial Insulin Glargine + Glulisine on to Background Orals ► ► 572 patients with type 2 diabetes uncontrolled on oral agents ● PREMIX: n=192 ● GLARG+1: n=189 ● GLARG+0-3: n=191 Mean baseline parameters: ● A1C 9.4% ● Age 54 years ● Diabetes duration 9 years ● BMI 33 kg/m2 “All to Target” study, Diabetes. 2011;60(suppl 1), 409-P, 073-OR Insulin Glargine + Glulisine: A1C and Hypoglycemia a b c a p < 0.025 versus PREMIX b p < 0.05 versus PREMI d c p < 0.05 versus PREMIX p < 0.01 versus PREMIX “All to Target” study, Diabetes. 2011;60(suppl 1), 409-P, 073-OR d Case #2 (cont.) ► Patient to switch to basal-bolus insulin therapy: ● ► After 3 months, patient remains on metformin + glimepiride, and is using 62 U glargine daily ● ► First step, patient starts with 40 U insulin glargine A1C now 7.2% Asked to repeat SMBG profiles prior to next visit Case #2 (cont) Question #3 Patient’s A1C is approaching target, but not fully there. What is next for this patient? 1) Continue basal insulin and increase dose 2) Continue basal insulin and initiate prandial insulin 3) Add GLP-1 receptor agonist to basal insulin 4) Return to twice-daily premix at lower dose 5) Continue basal insulin and recommend diabetes education to advise on controlling diet Mealtime Insulin: Rapid-Acting Analogs (Lispro, Aspart, Glulisine) vs Regular Analog insulin Insulin Activity 10 8 6 4 Human regular Timing of food absorbed 2 0 0 1 2 3 4 5 6 Hours Adapted with permission from Howey DC et al. Diabetes. 1994;43:396-402. 7 8 9 10 11 12 Insulin Glargine + Exenatide Buse,JB Ann Int Med 154:103, 2011 Question #4 How do you start dosing a short-acting analog at dinner? 1) Up to 4-6 U pre-meal 2) Use sliding scale 3) By body weight: 0.1 U/kg 4) By carbohydrate counting Case #2 (cont.) ► At 6-month follow-up patient is doing well with 56 U glargine and 14-18 U glulisine at dinner ► Mealtime dose occasionally adjusted based on: ● ● Meal carbohydrate content Activity ► A1C = 6.3% ► He feels well, has infrequent “hypos”, and is pleased with his BG control Case #2 (cont.) ► Continue follow-up with patient ► Over time, if postprandial glucose becomes elevated at meals other than dinner, add premeal insulin at that meal Basal-Bolus Insulin Replacement: Summary ► An effective insulin treatment strategy provides both basal and prandial insulin coverage ► Initially, prandial insulin may be needed only at the largest meal of the day, with coverage at other meals added based on postprandial glucose concentrations ► Rapid-acting insulin analogs more closely match post-meal carbohydrate absorption Insulin Therapy in Type 2 Diabetes: Conclusions ► Most patients will ultimately need insulin therapy alone or in combination with other agents to maintain glycemic control ► The most convenient strategy for initiating insulin is starting with a single dose of basal insulin ► Addition of prandial insulin should be considered when significant postprandial glucose excursions occur (e.g., >180 mg/dL), staring with the meal with the largest postprandial glucose excursion ► Side effects (risk of hypoglycemia and weight gain) must be addressed with patient, and appropriate follow-up scheduled New Paradigms, Guidelines, and Evolving Strategies Case Studies, Clinical Dilemmas, and 2012 ADA/EASD Guidelines for Diabetes Management Focus On Insulin-based Approaches Workshop Interactive, ARS Session VIVIAN A. FONSECA, MD, FRCP Program Chairman Professor of Medicine and Pharmacology | Tulis-Tulane Alumni Chair in Diabetes | Chief, Section of Endocrinology | Tulane University Health Sciences Center Case Studies and Clinical Dilemmas 1. Less stringent A1c goals may be appropriate for which of the following patients? 1) Patients with advanced microvascular complications 2) Patients with advanced macrovascular complications 3) Patients with extensive comorbid conditions 4) All of the above patients may qualify for less stringent A1c goals 5) None of the above patients qualify for less stringent A1c goals Case Studies and Clinical Dilemmas 2. With respect to recommendations contained in the new ADA/EASD Guidelines issued on April 19, 2012, all of the following are true for managing older patients with T2D, EXCEPT: 1) The focus should be on achieving specific glycemic targets 2) The focus should be on drug safety 3) The patient should be invited to participate in the treatment decisions 4) Less ambitious glycemic targets can be considered in the older patient 5) Glycemic targets less than 7.5%-8.0% can be considered if tighter control is not easily achieved ADA-EASD Position Statement: Management of Hyperglycemia in T2DM OTHER CONSIDERATIONS Age: Older adults Reduced life expectancy Higher CVD burden Reduced GFR At risk for adverse events from polypharmacy More likely to be compromised from hypoglycemia Less ambitious targets HbA1c <7.5–8.0% if tighter targets not easily achieved Focus on drug safety Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] Case Studies and Clinical Dilemmas 3. Which of the following statements regarding key considerations in the management of type 2 diabetes is FALSE? 1) The mechanisms driving hyperglycemia change with duration of the disease 2) The loss of beta cell function drives the full expression of the disease 3) Clinical inertia often results in prolonged exposure to hyperglycemia, thereby leading to increased risk of complications 4) Maximizing doses of first- and second-line agents before introducing additional therapies will always improve adherence and clinical outcomes Case Studies and Clinical Dilemmas 4. AJ is a 58-year old man with a recent history of type 2 diabetes. After being well controlled on metformin (2000 mg per day) treatment alone for 1 year, his latest A1c is 8.2%. Which of the following treatment options would be LEAST appropriate for AJ? 1) Increase his dose of metformin 2) Add a sulfonylurea to his treatment regimen 3) Add basal insulin to his treatment regimen 4) Add a GLP-1 agonist to his treatment regimen Diabetes Care, Diabetologia. 19 April 201 T2DM Antihyperglycemic Therapy: General Recommendations[Epub ahead of print] Progressive Platform Approach (PPA) to Glycemic Control A Practice-Oriented Analysis of 2012 ADA/EASD 2012 Guidelines Platform 1: Lifestyle Changes Plus Oral Foundation Agents Most patients will be started on the oral agent metformin, and if individualized target goals are not met promptly, an additional oral agent may be tried; or alternatively, a basal insulin is "usually" employed as the starting insulin. As a general rule, the use of more than two oral agents may not be optimal, and consideration to insulin or a GLP-1 agonist should be given if target goals are not reached with intensification of oral therapy. Treatment choices, at least in part, will depend on how far from goal the patient is. Inadequate Treatment Response Progress to Next Platform Progressive Platform Approach (PPA) to Glycemic Control A Practice-Oriented Analysis of 2012 ADA/EASD 2012 Guidelines Platform 2: Oral Foundation Agents Plus Basal Insulin If individualized target goal attainment fails with one or two oral agents, typically the management plan will focus on a combined oral-insulin based regimen, or the addition of a GLP-1 agonist. Usually, the foundation insulin for beginning therapy for platform 2 will be a basal insulin. Glycemic control with oral agents individualized to patient's needs plus a basal insulin will frequently be a sustainable regimen for many patients with T2D. Treatment choices, at least in part, will depend on how far from goal the patient is. Inadequate Treatment Response Progress to Next Platform Progressive Platform Approach (PPA) to Glycemic Control A Practice-Oriented Analysis of 2012 ADA/EASD 2012 Guidelines Platform 3: Multi-Insulin Regimen If individualized glycemic targets cannot be maintained on the combination of oral agents plus basal insulin or GLP-1 agonist, shorter-acting insulin formulations may need to be added to basal insulin to address post-prandial glycemic control. Insulin sensitizers may need to be continued. Platform 3 therapy will generally require titration of multi-insulin regimens to achieve glycemic control in patients who have progressive T2D and have failed a combined oral agent-basal insulin +/- GLP-1 agonist regimen. Bariatric surgery may be considered as an option, particularly when medical therapy is clearly failing in obese patients. Case Studies and Clinical Dilemmas 5. Which of the following statements about recent clinical trial findings related to the use of insulin in patients with type 2 diabetes is FALSE? 1) In a substudy of the UKPDS, patients with newly diagnosed type 2 diabetes demonstrated that early addition of insulin to oral agent monotherapy maintained glucose levels below target for 6 years 2) In the Treat-to-Target trial, glargine and NPH insulin demonstrated equivalent efficacy when added to 1 or 2 oral agents in type 2 diabetes 3) In the Treat-to-Target trial, rates of hypoglycemia were significantly lower with glargine than with NPH 4) In a recent study that examined the strategy of adding basal insulin versus a third oral agent to oral combination therapy with metformin and sulfonylurea, it was demonstrated that overall A1c reductions were significantly better with a maximal dose of rosiglitazone than with a low dose of insulin glargine Case Studies and Clinical Dilemmas 6. BP is a 42-year old man who was diagnosed with diabetes and started on metformin therapy 4 months ago. His current HbA1c is 8.2%. According to the ADA/EASD consensus algorithm, which of the following would be the LEAST appropriate next step in therapy for BP? 1) Add a sulfonylurea 2) Add basal insulin glargine 3) Add a glitazone 4) Add postprandial insulin Case Studies and Clinical Dilemmas 7. Which of the following statements about the pharmacokinetic characteristics of insulin glargine is FALSE? 1) Peak action occurs at approximately 5-7 hours from administration 2) Duration of action is approximately 24 hours 3) Glargine produces a flat action profile similar to that if continuous subcutaneous insulin infusion 4) Onset of action is approximately 2 hours Case Studies and Clinical Dilemmas 8. When the goal is to “minimize costs,” the new ADA/EASD Guidelines issued on April 19, 2012 for management of T2D suggest: 1) The combination of metformin plus a DPP-4 inhibitor 2) The combination of metformin plus a GLP-1 receptor agonist 3) The combination of metformin plus a insulin (usually basal) 4) The combination of metformin plus a thiazolidine-dione 5) All of the above 6) None of the above Case Studies and Clinical Dilemmas 9. Which of the following statements regarding insulin glargine in type 2 diabetes is TRUE? 1) Clinical trials have demonstrated significant intra-patient variability 2) Studies demonstrate that once-daily insulin glargine was less effective than NPH insulin given once or twice daily in reducing A1c levels 3) Clinical trials have demonstrated that nocturnal hypoglycemia was less frequent when using insulin glargine than with NPH insulin 4) Studies show that when compared to NPH insulin, insulin glargine use resulted in more weight gain ADA-EASD Position Statement: Management of Hyperglycemia in T2DM ANTI-HYPERGLYCEMIC THERAPY Therapeutic options: Insulin Neutral protamine Hagedorn (NPH) Regular Basal analogues (glargine, detemir) Rapid analogues (lispro, aspart, glulisine) Pre-mixed varieties Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] ADA-EASD Position Statement: Management of Hyperglycemia in T2DM ANTI-HYPERGLYCEMIC THERAPY Therapeutic options: Insulin Insulin level Rapid (Lispro, Aspart, Glulisine) Short (Regular) Intermediate (NPH) Long (Detemir) Long (Glargine) 0 2 4 6 8 10 12 14 Hours after injection 16 18 20 22 24 Case Studies and Clinical Dilemmas 10. The new ADA/EASD Guidelines issued on April 19, 2012 for management of T2D recommend or indicate all of the following EXCEPT: 1) Unless it is contraindicated, metformin is the optimal first-line drug 2) Comprehensive CV risk reduction is a major focus of therapy 3) The combination of metformin, plus the addition of at least two other appropriately selected oral agents, should precede use of insulin 4) The combination of metformin plus insulin (usually basal) is an appropriate second step in patients not achieving targets on 5) None of the above is correct Case Studies and Clinical Dilemmas 11. Which of the following options is the LEAST appropriate way to initiate basal insulin in a patient with type 2 diabetes? 1) Start with 10 units of bedtime insulin glargine 2) Start with 10 units of morning NPH insulin 3) Start with 10 units of morning insulin glargine 4) Start with 10 units of bedtime insulin detemir Case Studies and Clinical Dilemmas 12. Which of the following statements regarding the early initiation, addition, or intensification of insulin therapy in type 2 diabetes is FALSE? 1) Early insulin therapy has been shown to have beneficial effects on short-term glycemic control but little effect on long-term control 2) Short-term positive effects of early insulin initiation is explained by rapid reduction of glucotoxicity 3) Early initiation of insulin therapy may lead to immediate improvement in beta-cell function 4) Initiation of insulin therapy, after failure of lifestyle modification and an oral agent, is one option recommended in the ADA guidelines Sequential Insulin Strategies in T2DM Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of prin Case Studies and Clinical Dilemmas 13. All of the following are potential barriers associated with insulin initiation in diabetes, EXCEPT: 1) Potential for hypoglycemia 2) Weight gain 3) Potential for unpredictable action of long-acting formulations 4) Improved cognitive function with oral agents Case Studies and Clinical Dilemmas 14. When initiating insulin therapy in patients with type 2 diabetes, patients should be advised to maintain regular eating habits and exercise schedules, centered around their insulin treatment regimen. 1) True 2) False Case Studies and Clinical Dilemmas 15. TK is a 64-year old woman with a 3-year history of type 2 diabetes. Despite losing 10 pounds in the past year, her most recent A1c is 7.9%. Her current medication regimen includes metformin and a sulfonylurea. You decide to add insulin treatment to her regimen. Which of the following is the MOST appropriate next step in therapy for TK? Case Studies and Clinical Dilemmas 1) Start with bedtime intermediate-acting insulin; check fasting glucose weekly and increase dose until fasting levels are in target range; check A1c in 6 months 2) Start with morning basal insulin; check fasting glucose daily and increase dose until fasting levels are in target range; check A1c in 6 months 3) Start with bedtime basal insulin; check fasting glucose daily and increase dose slowly until fasting levels are in target range; check A1c in 3 months 4) Start with morning intermediate-acting insulin; check fasting glucose daily until fasting levels are in target range; check A1c in 3 months Case Studies and Clinical Dilemmas 16. Rapid-acting insulin analogues control postprandial glucose levels better than regular insulin, but cause more hypoglycemia. 1) True 2) False Case Studies and Clinical Dilemmas 17. In which of the following patients with type 2 diabetes would it be MOST appropriate to initiate insulin therapy? 1) A newly diagnosed 80-year old patient who is treatment naïve 2) A patient who has been on metformin monotherapy for 6 months with an A1c of 7%, who is prone to hypoglycemic episodes 3) A newly diagnosed 58-year old patient with severe hyperglycemia at diagnosis 4) All of the above would be good candidates for insulin therapy 5) None of the above would be good candidates for insulin therapy Case Studies and Clinical Dilemmas 18. GG is a 68-year old woman with a 3-year history of type 2 diabetes. Her A1c is 8.1% and she is currently on metformin, a sulfonylurea, and bedtime basal insulin. Her fasting plasma glucose levels are consistently around 110 mg/dL and her postprandial levels are around 180 mg/dL. Which of the following is the MOST appropriate next step in therapy for GG? 1) Increase her dose of basal insulin by 4 units and continue to monitor her fasting glucose daily 2) Discontinue her basal insulin and initiate treatment with a GLP-1 receptor agonist 3) Increase her dose of basal insulin by 2 units and add a pre-meal rapid-acting insulin 4) Add a rapid acting insulin before the largest meal with or without discontinuing her sulfonylurea ADA-EASD Position Statement: Management of Hyperglycemia in T2DM KEY POINTS Glycemic targets & BG-lowering therapies must be individualized. Diet, exercise, & education: foundation of any T2DM therapy program Unless contraindicated, metformin = optimal 1st-line drug. After metformin, data are limited. Combination therapy with 1-2 other oral / injectable agents is reasonable; minimize side effects. Ultimately, many patients will require insulin therapy alone / in combination with other agents to maintain BG control. All treatment decisions should be made in conjunction with the patient (focus on preferences, needs & values). Comprehensive CV risk reduction - a major focus of therapy. Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]