HPV and cervical screening
Test of cure
Dr Matt Hewitt
Cervical cancer in Ireland – key statistics
9th most frequently diagnosed cancer in women (278)
12th most common cause of cancer death in women (103)
Average age diagnosis - 46 years
Average age death - 56 years
Survival in Ireland is slightly lower than the European average.
The trends in mortality since 1978 show an increase of 1.5% per year.
• Ref: National Cancer Registry Ireland
• Cervical
cytology
• CervicalCheck
screening
programme
Early Diagnosis
• Vaccination
Secondary prevention
Primary prevention
Key points – prevention of deaths from cervical cancer
• Down staging
of cancers at
diagnosis
• Agreed
assessment
and referral
for women
with
symptoms
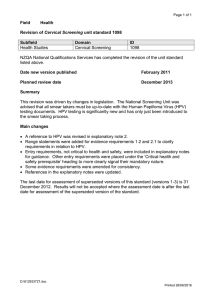
CERVIX
SQ
COL
SQ
COL
SQ – squamous epithelium
COL – Columnar epithelium
Acidic vagina
Metaplasia
External os
Glandular epithelium
(Ectropion)
New Sq Col Jun
Transformation zone
Area of metaplasia
Native Sq Col Jun
HPV
Acidic vagina
Metaplasia
Acidic vagina
Dysplasia
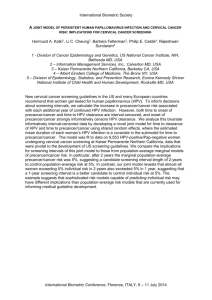
Natural history of HPV infection
•Transmission by sex
•Lifetime risk 80% most within 18
months
Exposure
Infection
•Transient
•Most resolve within
18 months
•Less than 20%
persist
•No antibodies
detectable
Persistence
Malignant
Transformation
•Virus integrates into
host DNA
•Loss of tumour
suppressor gene E2
•Uncontrolled cells
division
CIN
Natural history of CIN
Observe
Treat
(LLETZ)
Metaplasia
CIN I
CIN II
CIN III
Cancer
Use of HPV in screening
•In the management of women with low
grade sears
•In the follow up of women who have had
treatment
•Future use of HPV in screening
Low grade smears
•Very common
•Fill the colposcopy clinic with patients
•Majority of low grade CIN will resolve spontaneously
•Low grade CIN natural response to HPV infection
•Patient anxiety
•Cost
•How to overcome these problems?
• Use of HPV in low grade disease in colposcopy
• Use of HPV in primary care
Future screening protocols
•Incorporate HPV in primary care screening
•If Low grade smear and negative HPV avoid colp referral
•Advantages
• Cost saving
• Reduced anxiety in colposcopy referral
• Avoid unnecessary treatment
•Disadvantage
• Counselling women about HPV infection
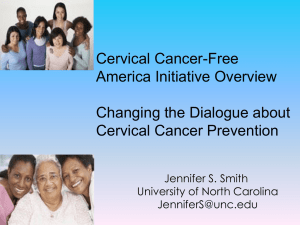
Options for follow-up after treatment
Cumulative incidence of CIN3+
Sensitivity of cytology
is low with high false
negatives
Traditional schedules
Compensate by
repeated smears –
annual for ten years
HPV test with cytology
has negative predictive
value of> 90%
Dillner, J. et al. BMJ 2008
Follow-up after treatment
Traditional
strategy
New strategy
6 month smear
at Colposcopy
12 month
smear
24 month
smear
36 month
smear
48 month
smear
60 month
smear
72 month
smear
84 month
smear
96 month
smear
120 month
smear
Routine Recall
6 Months
HPV and
Smear
18 months
HPV and
Smear
Discharge
to routine
screening
if double
negative
HPV 16 and 18
Advantages of
introducing the vaccine
•Reduced incidence of cervical cancer (adeno and
squamous)
•Reduced incidence of genital warts
•Reduce the incidence of genital cancer
•Reduced incidence of some head and neck cancers
•Potential to stop the cervical cancer screening
programme
•Greater impact in developing countries where there
is no cervical screening
Disadvantages of
introducing the vaccine
•Cost
•Only covers 70 – 75% of cervical cancers
•?Increased promiscuity
•Ethical issues of vaccination of teenage girls
•Delivery to young girls – counselling issues
•Decreased uptake of smears in screening programme
•Future role of colposcopy services
•Long term efficacy
•Side effects
•Bad publicity
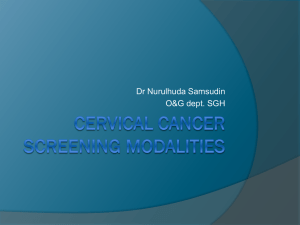
MORTALITY FROM CERVICAL
CANCER DEATHS (PER 100,000
PER YEAR)
5
IMPACT OF VACCINE AND DURATION OF
PROTECTION
4
10 year protection
& no screening
3
Screening
& no vaccination
10 year protection
& screening
Lifelong
& no screening
Lifelong protection
& screening
2
1
0
0
10
20
30
40
50
TIME SINCE START OF VACCINATION PROGRAM
Thank You