Surgical Options in Rectal Cancer

Colorectal Cancer Surgery
MR ZEEV DUIEB
GP DINNER PRESENTATION
06 AU GUST 2013 @6.30PM
CLOVER COTTAGE
D uieb
C olorectal
Suite 9, 1 st Floor, 50 Kangan Drive Berwick Ph 9709 6666
St J of G Suite 4 Gibb St Berwick 3806 Ph 9768 9331
Colorectal Surgeon Monash Health
Objectives in Colorectal cancer surgery
Prevention of surgical morbidity/ mortality
Optimal oncological clearance
Cancer and Lymph Node clearance > 12 LN
Prevention of local recurrence – TME, radioRx
Quality of life
Laparoscopic Surgery still needs to uphold these objectives.
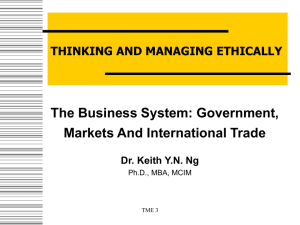
Colorectal Major Resections
B
C
A-B right hemicolectomy
A-C extd right hemicolectomy
A
E
F
D
B-C transverse colectomy
C-E left hemicolectomy
D-E sigmoid colectomy
D-F anterior rection
D-G (ultra) low anterior resection
32025 Anastomosis <10cm from anal verge
32026 Anastomosis <6cm from anal verge
D-H abdomino-perineal resection
A-D subtotal colectomy
A-E total colectomy
A-H total procto-colectomy
G
H
© CCrISP Australasia 3rd Edition
Historical vignettes
1826: Lisfranc 1st report of local excision
1884: Czerny
1886: Kraske
1907: Miles
1917: Bevan
1970: York-Mason
1979: Heald introduces TME
Total Mesorectal Excision
1984: Buess introduces TEM
Transanal Endoscopic Microsurgery
Rectal Ca Local excision -
Patient selection
Patient factors:
Elderly, frail and high anesthetic risk
Patient refusal of a stoma/ radical treatment
Rectal Ca Local excision -
Tumour factors
Location: <10 cm from the anal verge
Size & circumference of lesion:
No evidence to predict local recurrence
<4cm & <40% of circumference
Mobility: -Fixed tumours not appropriate
T staging:
LN involvement: T1(6-12%) T2(17-22%) T3(66%)
Local recurrence: T1(5%) T2(18%) T3(22%)
Tumour grade:
LN mets: well-mod diff(11%) poor diff(33%)
Local recurrence: well-mod diff(14%) poor diff(30%)
Rectal Ca Local excision -
Tumour factors
Lymphovascular & perineural invasion:
Greater likelihood of LN mets and local recurrence
LN mets: 33% vs 14-17%
Mucinour tumours:
Greater likelihood of LN mets and local recurrence
Nodal status:
Not appropriate for local excision
Rectal Ca Local excision -
Patient evaluation
PR/ sigmoidoscopy
Tissue biopsy: May miss area of poor differentiation
ERUS
Quoted accuracy T staging(67-93%) N staging(61-88%)
Recent study found the accuracy in picking T1(50.8%) and
T2(58.6%), understaging tumours(12.8%)
Marusch et al., Endoscopy 2002
MRI
Best for evaluating nodal status, accuracy at 82%
Colonoscopy, CT AP, PET-CT
Rectal Ca Local excision -
Patient evaluation
Recommended criteria:
<10 cm from anal verge
Tumour < 4cm and <40% of circumference
Favourable T1 stage
Well- moderate differentiation
No lymphovascular or perineural invasion
Non-mucinous tumours
No nodal disease
Rectal Ca Local excision – Old Fashioned Posterior approaches
Trans-sacral resection
Kraske procedure
Coccyx and lower 2 segments of sacrum excised
Sphincter complex preserved
Mid-rectal lesions
Cx: faecal fistula
Trans-sphincteric resection
York-Mason procedure
Similar approach to Kraske, however the sphincter complex is completely divided and sacrectomy not performed
Lower and mid rectal lesions
Cx: Incontinence and faecal fistula
Kraske posterior proctotomy
Rectal Ca Local excision – New Fashion Transanal approaches
Transanal excision
Full thickness excision with 1cm margin
Rectal defect closed transversely
Varying results in the lit, small retrospective series
Local recurrence high
T1(18%) T2(47%)
Survival
T1(72-90%) T2(55-78%)
Rectal Ca Local excision – Latest Fashion Transanal approaches
Transanal Endoscopic Microsurgery (TEM)
Developed for lesions out of reach from transanal approach
Can be used for benign lesions above the peritoneal reflection
Favourable T1 lesions have equivalent local recurrence and 5yr survival cf radical surgery
Unfavourable T1 lesions have higher local recurrence (10-15%)
TEM + XRT on T2 have local recurrence (25-46%)
Rectal Ca Local excision -
Ablative procedures
Electrocoagulation
Used as palliative & curative Rx
Disadv: no tissue spec, 1/3 conversion to radical surgery, 20% secondary haemorrhage
Poor outcomes
Endocavitatory radiation
Direct contact radiation 10-12000 cGy
Useful in palliative setting
In select pts 5yr survival & local control of 76-90%
Rectal Ca Radical excision Left colon mobilization
Splenic flexure mobilization
Sigmoid colon resected
Quality of circulation is poor
Functional outcomes as neo-rectum poor
High ligation of IMA
Allows mobilization of descending colon
Ligation of main trunk of left colic
Left colon mobilization
Left colon mobilization
Left colon mobilization
Radical excision-
Total Mesorectal
Excision(TME)
Introduced by RJ Heald in 1979
Use of sharp dissection under vision to mobilize the rectum rather than the conventional blunt finger dissection
First series of 112 pts: 5yr LR 2.9% and survival 87.5%
Local recurrence:
Conventional surgery: 11.7 - 37.4%
TME surgery: 1.6 - 17.8%
Higher leaks rates reported possibly due to:
Devascularisation of distal rectal stump
Lower anastamosis
Other factors: stomas, drains
TME -
Trials
Multi-institutional r/w of conventional to TME surgery found large difference in LR (4-9 vs 32-35%) and 5yr survival (62-75 vs 42-44%)
Havenga et al., Eur J Surg Oncol 25, 1999
Norwegian Rectal Cancer Grp:
Experiencing LR 25+%
1794 pts enrolled (1395 TME vs 229 conventional)
LR of 6 vs 12% (30m) and 4yr survival of 73 vs 60%
No difference in anastamotic leak rate (10%) & mortality (3%)
Dutch trial the largest prospective trial of 1861 pts demonstrated 2yr LR of 5.3% (TME 8.2% vs TME+XRT 2.4%)
Operative mortality (3.5 vs 2.6%) and anastamotic leak (11 vs 12%)
TME -
Technique
Peritoneal incision around rectum
Rectosigmoid reflected ant and posterior avascular plane developed using sharp scissor or diathermy dissection under vision
Blobbed lipoma should be demonstrated
Posterior dissection first, then lateral and finally anterior dissection
Do not ‘finger hook’ or clamp the lateral ‘ligaments’
Partial TME to a distance 5cm distal to tumour
Anterior dissection incorporates Denonvilliars fascia?
TME -
Technique
TME -
Nerve injury
Preaortic sympathetics during high ligation
Sympathetics at the pelvic brim during rectal mobilization
Parasymp(nervi erigentes) and sympathetics during posterolateral dissection
No clear lateral ligaments
Do not hook or clamp these tissues, avoid excessive traction
Higher rates exp by Japanese with extended lateral LN dissection
Anterior lateral dissection off the prostatic capsule
The most likely area of damage, reflected by higher rates of sexual dysfunction in APR(14-51%) vs AR(9-29%)
The role of denonvilliars fascia
TME -
Denonvilliars fascia
Charles Denonvillier described in
1836
Fusion of rectovesical cul-de-sac
Glistening white trapezoid apron
Anterior mesorectal envelope
Laterally close to neurovasc bundle
Visible on MRI
Heald et al recommend dissection in front
TME -
Fascial envelope
TME -
Denonvilliars fascia
Mortensen et al., recommends dissection behind the fascia as it is the natural continuation of lateral dissection
Also notes that there is a theoretical higher risk of nerve damage
Notes that there may be a role for dissection anterior to the fascia for anterior tumours
TME -
Distal resection margin
Not clear in the literature
5cm preop will expand to 7-8cm on rectal mobilization
This will shrink to 2-3cm with specimen removal and formalin fixation
Rare for tumour to spread beyond
1.5cm
Rare reports of poorly diff tumours having spread 4.5cm distally
Recommend: 5cm ideally however
2cm is adequate
Reconstruction of Neorectum
Hand sewn sutured anastamosis
1982: Parks and Percy performed the coloanal sutured anastamosis
‘Pulled through’ coloanal anastamosis (Turnbull & Cuthbertson)
Stapled anastamosis
Circular stapled technique
Double staple technique
For low and coloanal anastamosis
Reconstruction of Neorectum
Straight end to end
Low AR or Coloanal end-to-end anastamosis cause tenesmus, urgency and incontinence (Anterior resection syndrome)
Colonic J Pouch
Increases volume of neorectum
5 vs 10cm pouches have smaller reservoirs but better evacuation (Hida et al., Ds Colon Rectum 1996)
Size is critical to functional outcome, recommend 5-8 cm
Sigmoid colon should not be used
Better short term functional results and possible lower anastamotic leaks compared to end-to-end anastamosis
Coloplasty
New technique introduced in 1999 (Z’graggen et al., Dig Surgery 1999)
Better in narrow pelvis and limited length of colon
Long incision closed transversely
Randomized trial underway comparing to J-pouch
Abdominoperineal Resection
Described by Sir Ernest Miles 1908
1-2 surgeons
TME rectal dissection
Anus sutured closed
Wide perineal dissection, starting from posterior to lateral then anterior
Anterior dissection can proceed cranio-caudal or vice versa
SB exclusion - omentum or absorbable mesh
Drain the pelvic space
Reduced rates of APR
Coloanal anastamosis
Acceptance of smaller margins
Downsizing by chemoradiotherapy
Abdominoperineal Resection
Complications of Colorectal
Surgery
A N A S T O M O T I C L E A K
I N T R A A B D O M I N A L A B S C E S S , S T O M A
R E T R A C T I O N , H A E M O R R H A G E ,
D V T , W O U N D I N F E C T I O N , & O T H E R G E N E R A L
Principals - Locally advanced tumours
T3 and/or N1 Rectal lesions should have neoadjuvant
(preoperative) chemoradiotherapy
Select T4 lesions could be down staged prior to pelvic exenteration
Role of CRT downsizing and rates of sphincter preservation.
Rouanet et al., performed sphincter preservation in 21/27 pts after CRT downsizing. At 2 yrs only 2 LR
(Ann Surg 1995)
Grann et al., performed sphincter preservation in 17/20 T3 lesions
(Ds Colon Rectum 1997)
Factors Of Possible Prognostic Significance
(Surgeon Related)
1) Extent of margins of resection
- Intraluminally (2cms)
- Extraluminally (M.E. 5cms)
- Contiguous Organs
2) Extent of lymphatic resection
3) Timing and level of vascular ligation
4)
5)
Anastomotic technique
Intraluminal cytotoxic solutions
Conclusions
Beaware of the inaccuracies of preop staging
Local excision in favourable T1 lesions
TME should be standard practice in rectal dissection
Nerve preservation surgery
Role of distal margins
Neoadjuvant chemoradiotherapy
Laparoscopic Resection
Sacro-coccygectomy with APR
Colorectal Cancer Surgery Questions?
Dr Zeev Duieb
Dr Zeev Duieb is a Colorectal Surgeon. Melbourne born Dr Duieb studied at Monash
University and completed his Medical and Surgical training in Melbourne (FRACS).
Prior to establishing his own private practice in Berwick & Knox, Dr Duieb completed a Colorectal Fellowship with Southern Healthcare Network (Monash Health) where he has current Clinical Appointments to Dandenong (Colorectal Unit) and
Casey Hospital (General Surgery Dept).
D uieb
C olorectal
Suite 9, 1 st Floor, 50 Kangan Drive Berwick Ph 9709 6666
St J of G Suite 4 Gibb St Berwick 3806 Ph 9768 9331
Colorectal Surgeon Monash Health