The advantages of robotic low anterior resection
advertisement

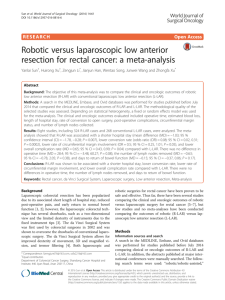
Slawomir Marecik, MD, FACS Advocate Lutheran General Hospital, Park Ridge, IL Clinical Assistant Professor University of Illinois, Chicago, USA Are here to stay One of the available tools in our armamentarium Powerful tool Massive potential Technically challenging Tumor location Anatomic structures Difficult retraction Unstable camera Poor ergonomics for surgeon UK MRC CLASICC Advanced lesion Obese, low (male) APR 1 Quality Of Dissection 2 Minimally Invasive 3 Comfort For Surgeon Quality Of Dissection Quality Of Dissection Robotic n=56 Laparoscopic n=57 Mesorectal grade Complete Mesorectal Grade 52 p=0.033 Complete 43 12 Nearly complete 4 Nearly complete Incomplete 0 Incomplete Baik SH. Robotic versus laparoscopic low anterior resection of rectal cancer: short-term outcome of prospective comparative study. Ann Surg Oncol. 2009 2 Pigazzi, Baek Kim Prasad, Marecik ROLLAR ACOSOG O.7 % CRM 1.6 % CRM 1 % CRM 143 pts 59 pts 82 pts Randomized Studies To Compare Laparoscopic vs. Robotic Resection Can we reduce preoperative radiation? Improved urogenital function? The robot is more useful in certain areas Laparoscopy is more useful in other areas A Hybrid Approach Is The Most Practical Solution At This Time Laparoscopic TME challenging Difficulties with advanced disease An increase in obese patient population Obesity Trends* Among U.S. Adults BRFSS, 1990, 2000, 2010 (*BMI 30, or about 30 lbs. overweight for 5’4” person) 2000 1990 2010 No Data <10% 10%–14% 15%–19% 20%–24% Source: Behavioral Risk Factor Surveillance System, CDC. 25%–29% ≥30% randomized data is lacking ACOSOG, ROLARR pending difficulties in adoption of Korean experience BMI height splenic flexure mobilization radiation DCR 2010 Open/HALS (=46) Robotic (n= 36) P value Mid and low rectal tumors 47.8% 80.5% .006 OR time (min) 273.8 337.9 .003 EBL (mL) 273.8 187.5 .036 Postoperative complications, n (%) 15 (32.6) 11 (30.6) .84 Length of stay (days) 7.3 7.0 .74 Distal margin positive, n (%) 0 (0) 1 (2.8) .44 Radial margin positive, n (%) 3 (6.5) 0 NS Lymph nodes 16.8 15 .26 deSouza AL, Prasad LM , Marecik SJ et al. Comparison of Open and Robotic Total Mesorectal Excision for Rectal Adenocarcinoma; Dis Colon Rectum, 2011 Robotic TME Laparoscopy for rectal cancer – conversion rates Author No. of Pts Conversion rate Mean BMI Laparoscopic Mean BMI Converted P value Yamamoto S Japan (2009) 1073 (Lap) 7.3% 22.7 (13.7-36.7) 24.6 (16.6-34.8) <0.0001 Agha A Germany (2008) 300 (Lap) 8.6% 26.2 (16.7-37.5) 29.0 (22.6-43.9) 0.002 Rottoli M Italy (2009) 173 (Lap) 15% 24.9 ±3.2 27.3±2.9 <0.001 deSouza 2010* 44 (Robotic) 4.5% 28.2 (17.6-43) 41.5 - MRC CLASSIC trial conversion rate – 34% (2005) Colorectal Dis 2011 APR (abdomino-perineal resections) cylindrical intraabdominal levator transection Robotic Cylindrical Abdominoperineal Resection with Intraabdominal LevatorTransection Marecik SJ, Zawadzki M, deSouza AL, Park JJ, Abcarian H, Prasad L Dis Colon Rectum, Oct 2011 Prasad LM, deSouza AL, Marecik SJ, Park JJ, Abcarian H. Robotic pursestring technique in low anterior resection. Dis Colon Rectum. 2010 Feb;53(2):230-4. upper rectum easy, thin patient Laparoscopic TME Mini-laparotomy lower rectum difficult, obese patient Robotic Robotic assistance in low anterior resection decreases conversion rates when compared to laparoscopy Mesorectal quality grade is higher in robotic technique, which may translate into better oncological outcomes Robotic system allows for a very precise work in deep pelvis making intersphincteric dissection easier, distal pursestring application possible and transanal specimen extraction more common Robotic assistance has potential to improve outcomes in obese patients and in patients with advanced disease