Pharmacologic Treatment of Chronic Systolic Heart Failure

Pharmacologic
Treatment of Chronic
Systolic Heart Failure
John N. Hamaty D.O. FACC,
FACOI
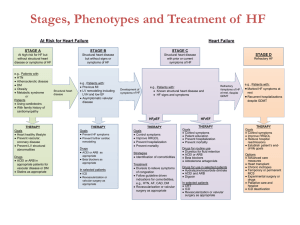
Heart Failure
Final common pathway in most heart diseases
550,000 new cases each year
20.1/100,000 mortality rate
No change in mortality
Diastolic Heart Failure
Impaired ability to accept blood and relax during diastole
Both types increase with age, African
Americans
40-70% incidence more often female, obese, older HTN and less likely to have
CAD
Less symptomatic and lower morbidity and mortality
B-Adrenergic Receptor Blockers
Improve survival
Improve ejection fraction
Remodeling
Quality of life
Reduce SCD
Inhibiting adverse effects of the sympathetic nervous system
Diminish RAAS activation
Angiotensin-Converting Inhibitors
Decrease conversion of angiotensin I-II
Improve survival
Decrease rate of hospitalization
Improve symptoms
Inhibit neurohormonal activation
Reverse remodeling
Decrease incidence of SCD?
Angiotensin Receptor Blockers
Efficacy similar to ACE inhibitors
Alternative to ACEI in patients not tolerant of ACEI
VAL-HeFT- ACEI +B-BL+ARB increase morality
CHARM- improve mortality
Competitive Aldosterone
Antagonists
Aldosterone stimulates renal sodium retention and myocardial hypertrophy
Spironolactone decreases mortality and morbidity in NYH class III and IV
Selective Aldosterone Blockers
Eplerenone (EPHESUS Trial)-post acute myocardial infarction trial
When added to optimal medical therapy excluding spirnolactone
Reduced morbidity and mortality in patients with acute MI with left ventricular dysfunction and heart failure
Future: New Insights
Tissue doppler-decreased flow velocities predict LVH before it occurs
Ultrasonic tissue character-tissue edema, fibrosis and calcification. Can predict tissue damage before it occurs in HTN
Myocyte enhancer factor 2-developmental gene for CAD/nonischemic HF
Pharmacogenetics
Alpha-adducin gene-found it 2/3 HTN patients. Diuretics will not reduce risk
Adrenergic receptors- 2 variants in African
Americans. 10 fold risk of developing HTN and candidates for early tx with b-blockers
Conclusions
Antagonizing this neurohormonal cascade has been the focus of recent clinical trials.
Further directions in HF therapy are likely to focus on limiting or preventing activation of the neurohormonal cascade through earlier recognition and treatment of patients at risk for HF.