Chronic Heart Failure
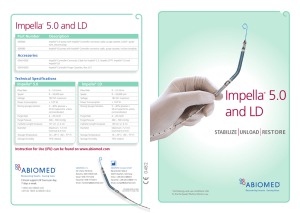
advertisement

Healing the Heart: When Failure is Not an Option September 12, 2013 GoToWebinar Housekeeping: attendee participation Your Participation Open and hide your control panel Join audio: •Choose “Mic & Speakers” to use VoIP •Choose “Telephone” and dial using the information provided Submit questions and comments via the Questions panel Note: Today’s presentation is being recorded and will be provided within 48 hours. Our Panelists Nazanin Moghbeli, MD, MPH, Cardiologist Salil Shah, MD, Cardiothoracic Surgeon Heart Failure Nazanin Moghbeli, MD, MPH, FACC September 10, 2013 Overview • • • • • • What is heart failure? Why should I know about it? What are the causes of heart failure? What are the signs and symptoms? How do you treat this disease? What can I do to prevent worsening heart failure? Definition of Heart Failure • Heart failure: is caused by damage to the heart and can be caused by many different reasons. i.e. heart attack or uncontrolled high blood pressure. • • Heart failure in this case - does not mean the heart has fully stopped. The heart is pumping with less strength than usual Understanding what is going on with the heart… • • • Blood moves through the body at a slower rate. As a result, the heart cannot pump enough oxygen and nutrients to meet the body's needs. As a result, the kidneys may respond by causing the body to retain fluid (water) and salt. Often fluid builds up in the arms, legs, ankles, feet, lungs, or other organs, the body becomes congested (full of fluid); hence the term congestive heart failure to describe the condition. How common is Heart Failure? • • Heart failure affects nearly 5.7 million Americans. Roughly 670,000 people are diagnosed with heart failure each year. • It is the leading cause of hospitalization in people older than 65. • 1 in every 5 people will develop heart failure in the US. Mortality Data * • • • 80% of men and 70% of women with less than 65 years of age and HF will die within 8 years Up to 42% of patients die of HF within 5 years of hospitalization of HF. Sudden cardiac death is 6 to 9 times more likely in a HF patient as compared to the general population. What causes Heart Failure (HF)? • • • HF is caused by conditions that damage the heart: Coronary artery disease (CAD)= a disease of the arteries of the heart. If arteries of the heart become blocked or narrowed, the heart can be damaged by lack of oxygen and nutrients. Heart attack= occurs when the heart arteries become suddenly blocked, stopping the flow of blood to the heart muscle. This damages the heart muscle, resulting in a scarred area that no longer functions well. Other causes of HF: • • • • • • • Alcohol High blood pressure Valve disease Thyroid disease Heart defects present at birth can all cause heart failure Preeclampsia Symptoms associated with CHF: • • Congested lungs: Shortness of breath: at rest, with exercise, or if lying flat Lung congestion can cause a dry hacking cough/wheezing Fluid and water retention. Less blood released by kidneys causes fluid and water retention, resulting in swollen ankles, legs, abdomen (called edema), and weight gain. May cause an increased need to urinate during the night. Stomach bloating may cause a loss of appetite or nausea. Symptoms often found in HF: • • Dizziness, fatigue, and weakness. Less blood to major organs and muscles can cause fatigue/weakness Less blood to the brain can cause dizziness or confusion. Rapid or irregular heartbeats. The heart beats faster to pump enough blood to the body. This can cause a rapid or irregular heartbeat. How do we treat heart failure • Medications that lower blood pressure and heart rate, thereby decreasing the strain on the heart • Restriction of water and salt • Treating diabetes, high blood pressure, coronary artery disease • Exercise • Smoking cessation Advanced treatment options for HF • • Mechanical Devices Heart transplantation (completely replacing the current nonfunctioning heart with a better functioning heart). Left Ventricular Assist Device (LVAD) Heart Transplantation * • • • Heart transplant patients can live a near-normal quality of life and functional capacity. 50% of all patients will live at least 9-10 years. Gold standard for appropriately selected patients with advancedstage HF Heart Transplantation • • • Only 2000 people a year receive transplants in the U.S Over 10% of people on the waiting list die each year waiting on a heart to become available. Hence additional options must be sought to improve outcomes and avoid deaths for these patients. What can I do? • • • • • Exercise Cholesterol control Weight management Medications as needed Avoid over the counter medications such as Motrin, decongestants • Avoid alcohol excess Einstein Heart Failure Services • • Diagnosis and workup of heart failure: Treatment, including careful monitoring of heart failure medications • Education • Team approach: PCP, patient, heart failure team • Mechanical support, transplant evaluation and referral Surgical Treatment of Heart Failure September 12, 2013 Objectives •Differentiate between acute and chronic heart failure •Surgical management of acute heart failure •Device options and efficacy •Surgical Management of Chronic Heart Failure •Ventricular Remodeling •Device placement and management •The Future Acute vs Chronic Heart Failure • Acute – A sudden change in heart function related to some new event that has caused damage to the heart. • Chronic – A gradual decline of heart function over a period of time. (Often the body compensates slowly for the loss of heart function). Causes of Acute Heart Failure: • Myocardial Infarction (aka Heart attack) • Pulmonary Embolism (Blood clot in the lungs) • Myocarditis (Inflammation) • Post-partum Cardiomyopathy (Enlarged heart after pregnancy) • Chronic heart failure with acute (new) flare • Trauma (i.e. direct injury to the heart) • Acute Heart Transplant Rejection Management • Most importantly, treatment is to prevent or stop the failure of other organs that are dependent on blood flow from the heart. • This can be done medically or with mechanical devices. Intra-Aortic Balloon pump • Device placed via the femoral artery (in the leg) to increase heart blood flow. • Pros: – Can be placed and removed by a catheter. – Will allow increased heart and brain blood flow • Cons: – Does not increase the amount of blood pumped by the heart – Has never been shown to improve survival. Tandem Heart • Centrifugal flow pump placed percutaneously • Designed to augment left ventricular output and rest left ventricle • Can augment cardiac output up to 5 LPM Pros: Can fully augment left ventricular cardiac output Placed and removed percutaneously Cons: Must have skilled person to place the cannula trans-septal Cannula position is difficult to control and cannula can migrate Tandem Heart • Many case studies and retrospective reviews to show efficacy, but no PRCT to show efficacy versus convertional therapy. • Theoretical advantage to allowing the left ventricle to rest and provide the body with support. • No mechanism to deal with right ventricular failure. • Trial starting now to determine efficacy versus other devices Impella • Axial flow device • 2.5- 5.0 L/min Active forward flow • Single Vascular access • 5 Minute setup\ • Percutaneous or surgical cut-down for placement • Multiple configurations possible • Operation independent of cardiac function or rhythm Console Impella New Technology Impella LD/LP 5.0 Impella CP Impella CP Pumps Impella LP2.5 Implantation Impella RP Investigational 31 Physiology of Impella Myocardial Protection Hemodynamic Support Inflow (ventricle) Outflow (aortic root) EDV, EDP O2 Demand Myocardial Protection AOP O2 Supply Flow Cardiac Power Output Systemic Hemodynamic Support Impella Unloading Effect ECMO • Extracorporeal Membraneous Oxygenation • Blood is removed from the venous system either peripherally via cannulation of a femoral vein or centrally via cannulation of the right atrium, – Oxygenate – Extract carbon dioxide • Blood is then returned back to the body either peripherally via a femoral artery or centrally via the ascending aorta. ECMO • Cadillac of mechanical support • Full cardiopulmonary bypass • Provides body with oxygenated blood • Provides body with full cardiac output • Allows heart and lungs to rest as body recovers from injury and insult ECMO Pros: Can be placed percutaneously anywhere Provides full heart and lung support Allows for bridge to decision Cons: Must be removed surgically Need trained staff to monitor and adjust 24 hrs/day while on support Have increased bleeding and vascular complications Bottomline • All therapies have their place • If chosen and used correctly will take an almost uniformly deadly situation and provide a chance for recovery • There are indications for each device and all devices are approved to be used in acute cardiogenic shock situations. Chronic Heart Failure • Decline of heart function over a period of time where the body compensates slowly for the decrement in heart function. • Treatment: – Medication-Ionotropes, afterload reduction – Ventricular Remodeling – Mechanical Support-LVAD/RVAD – Heart Transplantation Heartmate II • Continuous axial flow pump • Connects LV apex to Aorta • Bypasses blood flow from the left ventricle • Only has exteriorized driveline connected to external monitor and power source • Must be placed surgically • Can be used as bridge to transplant or as destination therapy Heartmate II • Pros: – Excellent flow device – Very durable – Easily implantable – Has excellent long term efficacy and data • Cons: – Difficult to explant – Need chronic anticoagulation – Device does have defined lifespan – Patient must be of a certain size to accommodate device The Future •Heartware •Impella RP outflow inflow Heartware • Continuous axial flow pump • Connects LV apex to Aorta • Bypasses blood flow from the left ventricle • Only has exteriorized driveline connected to external monitor and power source • Must be placed surgically • Can be used as bridge to transplant or as destination therapy • Small device can be placed in any body habitus • Can be used for biventricular long-term support • Currently on trial Impella RP • Catheter-based percutaneous VAD (22 Fr pump mounted on a 11 Fr catheter) • Treatment: Right ventricular dysfunction • Flow: > 4 L/min • Duration of support: up to 14 days • Pump Inflow: Inferior Vena Cava (IVC) Pump Outflow: Pulmonary Artery (PA) outflow inflow Thank You!! Contact Information Dr. Moghbeli Einstein Advance Heart Failure Program Location 5501 Old York Road Philadelphia, PA 19141 To talk to one of our team, call the Heart Failure Hotline at 215-292-1958 Dr. Shah Salil G. Shah 215-456-8543 5501 Old York Road Klein 409 Philadelphia, PA