228_eposter - Stanley Radiology
advertisement

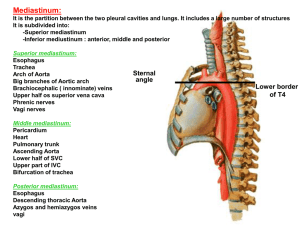
Imaging spectrum of Immunoglobulin G4-related disease (IgG4-RD) - a pictorial review Abstract number: IRIA - 1209 Introduction • Immunoglobulin G4-related disease (IgG4-RD) is an increasingly recognized immune-mediated condition • Swelling of involved organs, lymphoplasmacytic infiltrate with IgG4-positive plasma cells, fibrosis with “storiform” pattern and elevated serum IgG4 are seen • Different organs in varying combinations can be involved Aims & objectives • This pictorial essay is aimed to depict the spectrum of imaging findings in patients with proven IgG4related sclerosing disease • Materials & methods • Proven cases of IgG4-related disease were reviewed and the spectrum of imaging findings are depicted • Diagnostic criteria include: (i) Increased serum IgG4 (> 135 mg/dL) (ii) >45 IgG4-positive cells per high-power field (iii) IgG4/IgG ratio >30% in involved tissues Salivary glands CECT Axial: Bilateral swelling of the parotid glands with multiple hypodense lesions CECT Coronal: Bilateral swelling of the parotid glands Low-attenuation lesion incidentally noted in the thyroid gland Orbit Bilateral symmetric thickening of the extraocular muscles and lacrimal glands with proptosis (blue arrows) Case 1 Sino-nasal Cavity 15 year old girl with recurrent epistaxis T2-hypointense soft tissue thickening involving the nasal septum and right lateral nasal wall Extension into the right maxillary sinus T1W GADO Heterogeneous enhancement of lesion with central hypoenhancing regions Case 2 Sino-nasal cavity 15 year old girl with recurrent right sided nasal bleed T2 - soft tissue thickening involving the nasal septum and sphenoid sinus T1W GADO Heterogeneous enhancement of lesion Case 3 Sino-nasal Cavity Patient with history of left pre-auricular pain, difficulty in mouth opening a intermittent headache in the left temporal region Ill-defined poorly enhancing soft tissue lesion filling the maxillary sinus and extending into the masticator space Thinning and erosion inferior wall of orbit with thickening and sclerosis of anterior wall and floor of maxillary sinus Sino-nasal cavity and palate Case 4 Patient with inability to open mouth for the past 6 months Lytic lesion involving the left hard palate and adjacent alveolar process of maxilla Enhancing soft tissue extending into the left nasal cavity with destruction of medial wall of maxillary sinus Multiple patchy parenchymal and subpleural opacities in the lungs Central nervous system Enhancing dural thickening with intense FDG uptake T1 post Gado IAC IAC Dural thickening with abnormal enhancement, also extending along cranial nerves Lung Intense FDG uptake with SUV of 15 in the right apical lung parenchymal lesion (white arrow) A B Biopsy from lung lesion shows Dense lymphocytic infiltration on Hand E staining(A) special staining showing IgG4plasma cells (B) Significant reduction in size of lung lesion post treatment A B Lung Lung Case 1 Cardiovascular Isointense sheet like soft tissue seen surrounding • Anterior mitral leaflet and IAS • LVOT, Aortic root, Ascending and Arch of aorta • Distal thoracic aorta • Pericardial effusion Cardiovascular CT of PET Homogenous soft tissue density is seen surrounding • Anterior mitral leaflet(black arrow) • LVOT, Aortic root, Ascending and Arch of aorta (white arrows) and • Distal thoracic aorta (blue arrow) • Also note the extension into root of left subclavian artery(green arrow) • Minimal pericardial effusion (red arrow ) No significant mediastinal adenopathy Left main LAD encasement (yellow arrows) Cardiovascular F-18 FDG PET-CT PET-CT shows significant FDG uptake (SUV-Upto 5 ) in the homogenous eccentric periaortic soft tissue Descending thoracic aorta Ascending aorta LVOT Post steroid therapy with marked resolution Cardiovascular Case 2 19 years old girl with high blood pressure Plasma IgG4-1827mg/L Eccentric periaortic soft tissue with luminal narrowing of distal thoracic and proximal abdominal aorta 19/05/2014 24/09/2014 Cardiovascular 55 years old lady with polyneuritis cranialis, elevated serum IgG4-2778 mg/L Periaortitis involving ascending, arch and great vessels showing good response to high dose steroids and mycophenolate Case 3 Para-vertebral 41years old gentleman with fever, chest pain for 8 months, IgG4 levels-1384mg/L Right posterolateral thoracotomy and open biopsy confirmed IgG4 related disease • • Eccentric homogenous lower thoracic para-vertebral soft tissue with FDG uptake (SUV-5) (red arrows) Minimal pericardial thickening and effusion(blue arrow) Pancreas Patients with IgG4 related autoimmune pancreatitis Enlarged sausage shaped pancreas • Bulky featureless pancreas with hypodense rim suggesting autoimmune pancreatitis • Lobulated presarcal soft tissue Retroperitoneal Homogenously enhancing soft tissue encasing aorta, IVC and bilateral iliac arteries Aorta Iliac arteries Left moderate hydroureteronephrosis with reduced parenchymal enhancement What should make us suspect IgG4 disease on imaging? • • • • • Multi-organ involvement Sheet like infiltrative soft tissue thickening Hypo to iso-intense on T2W images Homogeneous sheet like intense enhancement Peri-aortitis with eccentric wall and peri-aortic soft tissue thickening • Excellent response to glucocorticoids SUMMARY Patients with IgG4 related disease usually respond well to corticosteroid therapy; therefore, It is important that radiologists recognize the condition to establish an early diagnosis and avoid unnecessary invasive procedures