Why Bother! Pre-op Testing - The New York Academy of Medicine
advertisement

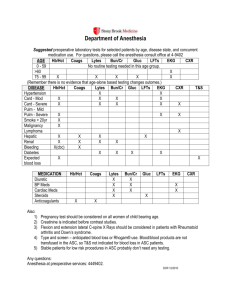
Elizabeth A. M. Frost MD Dept of Anesthesiology Icahn Medical Center at Mount Sinai “On feeling the pulse of a 21 y/o…I found it to be small, weak, and intermitting. I told the patient he had nothing to apprehend. His pulse improved. He inhaled the chloroform, His teeth were extracted. He woke up. Now, if the inhalation had commenced without inquiry, the syncope would have had the appearance of being caused by the chloroform” pp 77-8 John Snow. And so, physical examination before anesthesia was born! Surgeon at Flower Fifth 1898 Canvassed patients for surgeons so he could anesthetize them..his total training in anesthesia Became 1st anesthetist at Flower, 1899 Later Professor of Anesthesia, NY Medical College. (the start of fee splitting ???) Huge hospitals…lots of beds…all inpatients. Surgeons depended on internists for patient referrals. Patients sent back to internists for work up. Many tests recommended 1990’s…Questions…do these tests make any difference in outcome? Answer: But we ALWAYS did it that way. Cost >$60 billion annually >60% not indicated 0.22% reveal pertinent abnormalities Abnormalities mostly ignored No adverse consequences False positives potentially harmful (Roizen, Can J Anaesth 1989) Chest X-ray=$128 EKG=$216 CBC=$156 Electrolytes=$626 Urinalysis=$85 Stress test=$2300 ?? Bundling?? Total= $3511 Choosing wisely: educational initiative, under the auspices of Amer Board of Internal Medicine, Consumer Reports, 9 specialty boards. $750b spent on unnecessary tests and hospitalizations (1/3rd all health costs) Should perform fewer tests; patients should question need for tests. Proceedings of the 4th Annual Perioperative Medicine Summit: Cleveland Clinic 2009: suppl 4 Vol 76.The role of testing in the preoperative evaluation Practice Advisory for Preanesthesia Evaluation: ASA Oct 2011; Anesthesiology 2012 (with 173 references) American College of Cardiology/American Heart Association, European Society of Cardiology. Updated guidelines (Schiefermueller J et al Angiology 2012: May 3rd) Preanesthesia Evaluation for ambulatory surgery; Hofer J. Curr Opin Anaesthesiol 2013; 26(6): 669-76 Emphasis on preoperative clinical risk stratification EKG: older (age not specified), cardiorespiratory disease Stress test :Cardiovascular compromise Chest X ray: Recent URI , smoking, COPD, cardiac disease PFTs :Reactive disease, COPD, scoliosis Hb/Hct :Anemia, bleeding disorders Coagulation studies: Bleeding, renal dysfunction, liver disease, anticoagulants Chemistries: Endocrine, renal disease, medications Pregnancy: Women of child bearing age OSA suspected: Sleep study (ASA 2013) Thailand: Use institution’s preop guidelines: decrease unnecessary testing and financial burden(1) UK: No evidence of clinical and cost effectiveness of routine preop tests (2) Germany: Implementation of guidelines in 2010 to decrease testing allowed more reasonable approach to preop risk evaluation(3) Canada: Pregnancy testing indicated (4) AND THEN THERE IS A SURGICAL OPINION Texas: Recommendations from the ASA not specific to ambulatory surgery, not based on strongly designed and adequately powered studies. Unclear. Need studies involving surgeons and others (5) 1. Siriussawakul A et al Biomed Res Int 2013: 2013:835426, 2. Czoski-Murray C Health Technol Assess 2012; 16(50): i-xvi, 1-159, 3. Bohmer AB Anaesthetist 2014; 63(3): 198-208, 4. Maher JL Can J Plast Surg 2012; 20(3): e32-4, 5. Benarroch-Gampel J Adv Surg 2013; 47; 81-98 My administrator (secretary, wife) orders them Patient expects to give blood and be tested Anesthesia will cancel the case if there are no tests There is medicolegal liability without testing It makes me feel comfortable I have to support the hospital and labs Must follow history and physical Diabetic and blood sugar day of surgery Renal failure and potassium Chest X-ray only if H and P dictates (no age limit) EKG? Age limit? Probably not. Tests; ONLY per H and P EKG if older and not minor surgery (EKG valid for 6 months if no interval change) Chest X ray not mandatory at any age Pregnancy urine test on day of surgery Blood sugar for all diabetics Potassium in ESRD CBC and electrolytes as indicated by H and P only Let’s (Not) Get Physicals We cling to the ritual of the annual exam, despite evidence that it isn’t needed. Jettison EKG, chest X-ray, blood work for healthy people. E Rosenthal Preop lab and EKG testing should be driven by history, physical and surgical risk Test indicated only if it can correctly identify abnormalities, change diagnosis, management plan or outcome (includes radiology) Needless tests cause expense,delays, complications Improved standardization needed One size does not fit all.