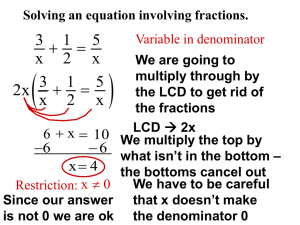
Stage 2 Meaningful Use
E L I G I B L E H O S P I TA L S ( E H )
&
C R I T I C A L A C C E S S H O S P I TA L S ( C A H )
Conflict of Interest Disclosures
None
Changes to Stage 1 Objectives
•
CPOE
•
•
Vital Signs
•
•
Denominator: More than 30% of medication orders created by the EP or authorized providers of the EH
or CAH’s inpatient or emergency dept (POS 21 or 23) during the EHR reporting period are recorded using
CPOE
Denominator: More than 50% of all unique patient seen admitted to the EH or CAH’s inpatient or
emergency dept (POS 21 or 23) during the EHR reporting period have blood pressure (for ages 3+ only)
and height and weight (for all ages) recorded as structured data
Clinical Quality Measures
•
•
•
Objective removed
Hospitals are still required to report on CQMs
Now follow 2014 CQM requirements
Where Are We At?
Stage 2
Stage 1
•
Capture
Information
• Reporting
• Exchanging
Information
• Patient
Engagement
Stage 3 and
Beyond…
• Leveraging
Information for
Improved
Patient Care
Understanding the Timing of Stage 2
Stage 2 Meaningful Use
•
Report on total of 19 Objectives
•
•
Plus Clinical Quality Measures (CQM)
16 Core Objectives
•
•
•
All Required
Many Stage 1 combined
6 Menu Objectives
•
•
Choose 3
Clinical Quality Measures (CQM)
•
•
•
Report on 16 of 29 approved CQMs
Selected CQMs must cover at least 3 of 6 National Quality Strategy Domains
Electronically repot to CMS
MU in 2014
For 2014 only:
•
All EHs and CAHs regardless of their stage of meaningful use are only
required to demonstrate meaningful use for a 3-month EHR reporting
period.
•
CMS is permitting this one-time 3-month reporting period in 2014 only
so that all hospitals who must upgrade to 2014 Certified EHR Technology
will have adequate time to implement their new Certified EHR systems.
MU in 2014
•
Reporting Period = 3 month quarter (2014 Only)
Must be a fixed calendar quarter
•
•
January – March
•
April – June
•
July – September
•
October – December
Must be completed by December 31st
•
•
•
Start no later than October 1
Payment Adjustments begin in 2015
Avoiding Payment Adjustments
•
If you’re beginning in 2014
•
Must demonstrate 90 days before 4th quarter
•
Must attest NO LATER than October 1, 2014
•
Avoiding Medicare payment adjustments in the future
•
Must continue to demonstrate every year
•
If eligible for Medicare and Medicaid, must demonstrate every year
•
If eligible for Medicaid ONLY, you are not subject to adjustments
Computer Provider Order Entry (CPOE)
Objective
Use CPOE for medication, laboratory, and radiology orders directly
entered by any licensed healthcare professional who can enter orders
into the medical record per state, local and professional guidelines.
Denominator
Medications: Number of medication orders created by the EH
or CAH’s inpatient or emergency department (POS 21 or 23)
during the EHR reporting period.
Radiology: Number of radiology orders created by the EH or
CAH’s inpatient or emergency department (POS 21 or 23) during
the reporting period.
Laboratory: Number of lab orders created by the EH or CAH’s
inpatient or emergency department (POS 21 or 23) during the
reporting period.
Numerator
The number of orders in the denominator recorded using CPOE
Threshold:
Medications: > 60%
Labs: > 30%
Radiology: > 30%
Increased medication
threshold 30% to 60%
30% radiology and 30%
lab orders added to
objective
Denominator changes to
number of orders
Record Demographics
Objective
Record all of the following demographics:
Preferred Language
Sex
Race
Ethnicity
Date of Birth
Date & Preliminary Cause of Death (in the event of mortality in
the EH or CAH)
Threshold increased
from 50% to 80%
Denominator
Number of unique patients admitted to the EH or CAH’s inpatient or
emergency department (POS 21 or 23) during the EHR reporting
period.
Numerator
Number of patients in the denominator who have all the elements of
demographics (or a specific notation if the patient declined to
provide one or more of the elements) recorded as structured data.
Threshold: > 80%
Terminology change:
“Gender” replaced with
“Sex”
Record Vital Signs
Objective
Record and chart changes in the following vital signs:
Height/Length & Weight (no age limit)
Blood Pressure (ages 3 and over)
Calculate & Display BMI
Plot & Display Growth Charts for Patients 0 – 20 yrs (including
BMI)
Denominator
Number of unique patients admitted to the EH or CAH’s inpatient or
emergency department (POS 21 or 23) during the EHR reporting
period.
Threshold increased from
50% to 80%
Blood pressure on
patients aged 2 yr olds no
longer required
Numerator
Number of patients in the denominator who have at least one entry
of their height and weight (all ages) and/or blood pressure (ages 3
and over) recorded as structured data.
Threshold: > 80%
Patients aged 0-2 yrs old now
included in Growth Charts
Record Smoking Status
Objective
Record smoking status for patients 13 yrs old and older
Denominator
Number of unique patients aged 13 or older admitted to the EH or
CAH’s inpatient or emergency department (POS 21 or 23) during the
EHR reporting period.
Threshold increased from
50% to 80%
Numerator
Number of patients in the denominator with smoking status recorded
as structured data.
SNOMED Codes required
Threshold: > 80%
8 smoking status selections
to include cigar & pipe
smokers
Clinical Decision Support (CDS)
Objective
Implement 5 Clinical Decision Support interventions related to 4 or
more clinical quality measures at a relevant point in patient care for
the entire EHR reporting period
AND
Increased from 1 to 5 CDS
Rules
Implement drug-drug and drug-allergy checks for the entire reporting
period
Attestation Requirement: Yes/No
CDS must relate to clinical
quality measures
Incorporates DrugDrug/Drug-Allergy
Interaction Checks
Patient Electronic Access
Objective
Provide patients the ability to view online, download, and transmit
information about hospital admission.
Denominator
Replaces Stage 1 eCopy of
PHI objective
Number of unique patients discharged from the EH or CAH’s
inpatient or emergency department (POS 21 or 23) during the
reporting period.
Numerator
Access: Number of patients in the denominator whose information is
available online within 36 hours of discharge
Engagement: Number of patients in the denominator who have
viewed online, downloaded, or transmitted to a third party the
discharge information provided by the EH or CAH.
Threshold:
Access: > 50%
Engagement: > 5%
Requires 5% patient
engagement
Denominator is now 50% of
all discharged patients rather
than those requesting
What Must be Available Online?
The EH or CAH can make additional information available, however, the following
information must be available to satisfy the objective and measure:
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Patient Name
Admit and discharge date & location
Reason for hospitalization
Care team including the attending of record as well as other providers of care
Procedures performed during admission
Current and past problem list
Current medication list and medication history
Current medication allergy list and medication allergy history
Vital signs at discharge
Laboratory test results (available at time of discharge)
Summary of care record for transitions of care or referrals to another provider
Care plan field(s), including goals and instructions
Discharge instructions for patient
Demographics maintained by hospital
Smoking status
Patient Portals & Minors
Parents as Personal Representatives
• Personal representative has the right of the individual
• Rights should be cut off at age of majority
• Parent may not be personal representative for certain information, such as
when a minor can consent under state law
• Personal representatives and minors can pose significant challenges to the
organization
• Will the organization require authorization before establishing proxy rights to the portal
• How will the organization handle revocation of authorizations? Restriction requests?
• How will the organization ensure parent’s access is revoked once patient reaches age of
majority?
Patient Portals & Minors
What can the organization do?
•
•
•
Ensure compliance with applicable Federal & State laws regarding minors
Consult internal HIPAA privacy liaison to ensure portal access/rights are consistent with
Federal & State laws and other organizational practices
Approaches by other Healthcare Providers:
•
•
For patients under the age of 14, parents are able to access the portal with parental signed request
For patients aged 14-18,
•
•
•
•
Providers can withhold information if they believe it would jeopardize the health of their
patient in accordance with HIPAA privacy regulations
•
•
Require the child to sign a release form
Restrict parental access to certain sensitive data as required by applicable laws
Restrict portal access for minors ages 14-18
Consult internal HIPAA privacy liaison
Also note that there are differences for minors who are emancipated
Protect Electronic Health Information
Objective
Conduct or review a security risk analysis in accordance with the
requirements under 45 CFR 164.308(a)(1), including addressing the
encryption/security of data stored in CEHRT in accordance with
requirements under 45 CFR 164.312 (a)(2)(iv) and 45 CFR
164.306(d)(3), and implement security updates as necessary and
correct identified security deficiencies as part of the provider’s risk
management process for eligible hospitals.
Attestation Requirement: Yes/No
Update risk management
processes to address any newly
identified risks since last SRA
Risk analysis function required to
place emphasis on encryption of
PHI stored in CEHRT
Objective not meant to replace,
change, or supersede HIPAA
Privacy & Security Rule
Clinical Lab Test Results
Objective
Incorporate clinical lab test results into Certified EHR Technology
(CEHRT) as structured data.
Denominator
Number of lab tests ordered during the EHR reporting period by the
EH or CAH’s inpatient or emergency department (POS 21 or 23)
whose results are expressed in either a positive/negative or numeric
format.
Moved from Menu to
Core Set
Numerator
Number of lab test results which are expressed in a positive/negative
or numeric result are incorporated into CEHRT as structured data.
Threshold: > 55%
Threshold increased
from 40% to 55%
Patient Lists
Objective
Generate at least one list of patients by specific condition to use for
quality improvement, reduction of disparities, research, or outreach.
Attestation Requirement: Yes/No
Moved from Menu to
Core Set
Must be based on information
contained within the following
fields: problems, medications,
medication allergies,
demographics, labs
Patient-Specific Education Resources
Objective
Use clinically relevant information from CEHRT to identify patientspecific education resources and provide those resources to the
patient.
Denominator
Number of unique patients admitted to the EH or CAH’s inpatient or
emergency department (POS 21 or 23) during the EHR reporting
period.
Numerator
Number of patients in the denominator who are subsequently
provided patient-specific education resources identified by CEHRT.
Threshold: > 10%
CEHRT is certified to use problem
list, medication list, or lab results
to identify educational resources
Education resources do not
have to be stored within or
generated by CEHRT
Utilize CEHRT in a manner where the
technology suggests patient-specific
educational resources based on
information stored within CEHRT
Medication Reconciliation
Objective
The EH or CAH who receives a patient from another setting of care or
provider of care or believes an encounter is relevant should perform
medication reconciliation.
Denominator
Number of transitions of care during the EHR reporting period for
which the EH or CAH’s inpatient or emergency department (POS 21
or 23) was the receiving party of the transition.
Moved from Menu to Core
Set
Numerator
Number of transitions of care in the denominator where medication
reconciliation was performed.
Threshold: > 50%
Information included in the
process of medication
reconciliation is determined
by the provider & patient
Summary of Care
Measure 1
Objective
The EH or CAH who transitions their patient to another setting of care
or provider of care or refers their patient to another provider of care
provides a summary of care record for each transition of care or
referral.
Moved from Menu to Core Set
Denominator
Number of transitions of care and referrals during the EHR reporting
period for which the EH or CAH’s inpatient or emergency department
(POS 21 or 23) was the transferring or referring provider.
Numerator
Must verify current problem list,
current medication list, and current
medication allergy list includes the
most recent information known at
the time
Number of transitions of care and referrals in the denominator where
a summary of care record was provided.
Threshold: > 50%
Can send paper or electronic copy of
summary care record directly to next
provider, or can provide it to patient to
deliver to next provider (if patient can be
reasonably expected to do so)
Summary of Care
Measure 2
Objective
The EH or CAH who transitions their patient to another setting of care
or provider of care or refers their patient to another provider of care
provides a summary of care record for each transition of care or
referral.
Requires electronic
transmission
Denominator
Number of transitions of care and referrals during the EHR reporting
period for which the EH or CAH’s inpatient or emergency department
(POS 21 or 23) was the transferring or referring provider.
Numerator
Number of transitions of care and referrals in the denominator where
a summary of care record was:
Electronically transmitted using CEHRT to a recipient
OR
Where the recipient receives the summary of care record via
exchange facilitated by an organization that is a NwHIN Exchange
participant or in a manner that is consistent with the governance
mechanism ONC establishes for the nationwide health
information network. The organization can be a third-party or
the sender’s own organization.
Threshold: > 10%
The summary of care record
must be received by the
provider to whom the
sending provider is referring
or transmitting the patient
Summary of Care
Measure 3
Objective
The EH or CAH who transitions their patient to another setting of care
or provider of care or refers their patient to another provider of care
provides a summary of care record for each transition of care or
referral.
Attestation Requirement: Yes/No
The EH or CAH must satisfy one of the two following criteria:
Conducts one or more successful electronic exchanges of a
summary of care document, which is counted in Measure 2 with
a recipient who has EHR technology that was designed by a
different EHR technology developer than the sender’s CEHRT
Incorporates Stage 1 Electronic
Exchange of Key Clinical
Information objective
“EHR Randomizer” will randomly
match EH or CAH with a designated
test EHR that is designed by a
different EHR technology developer
than theirs
OR
Conducts one or more successful tests with the CMS designated
test EHR during the EHR reporting period.
Current Designated Test EHRs:
McKesson, Meditech,
iPatientCare
What Must be Available on the
Care Summary?
A summary of care record must include the following:
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Patient Name
Procedures
Encounter diagnosis
Immunizations
Laboratory test results
Vitals signs
Smoking status
Functional status, including activities of daily living, cognitive and disability status
Demographic information
Care plan field, including goals and instructions
Care team including the primary care provider of record and any additional known care team
members beyond the referring or transitioning provider and the receiving provider
Discharge instructions
Current problem list
Current medication list
Current medication allergy list
Immunization Registry Data Submission
Objective
Capability to submit electronic data to immunization registries or
immunization information systems except where prohibited, and in
accordance with applicable law and practice.
Attestation Requirement: Yes/No
Moved from Menu to Core
Set
Successful ongoing
submission is required
Electronic Reportable Lab Results
Objective
Capability to submit electronic reportable laboratory results to public
health agencies, except where prohibited, and in accordance with
applicable law and practice.
Attestation Requirement: Yes/No
Moved from Menu to Core
Set
Successful ongoing
submission is required
Syndromic Surveillance Data Submission
Objective
Capability to submit syndromic surveillance data to public health
agencies, except where prohibited, and in accordance with applicable
law and practice.
Attestation Requirement: Yes/No
Moved from Menu to Core
Set
Successful ongoing
submission is required
Electronic Medication Administration
Record (eMAR)
Objective
Automatically track medications from order to administration using
assistive technologies in conjunction with an electronic medication
administration record (eMAR).
Denominator
New objective
Number of medication orders created by authorized providers in the
EH or CAH’s inpatient or emergency department (POS 21 or 23)
during the EHR reporting period.
Numerator
Number of orders in the denominator for which all doses are tracked
using eMAR.
Threshold: > 10%
If a medication is ordered but
not all doses of the medication
are tracked using eMAR, then
that order may not be included
in the numerator
Advance Directives
Objective
Record whether a patient 65 years or older has an advance directive.
Denominator
No changes from Stage 1
Number of unique patients age 65 or older admitted to the EH or
CAH’s inpatient department (POS 21) during the EHR reporting
period.
Numerator
Number of patients in the denominator who have an indication of an
advance directive status entered using structured data.
Patients admitted to the
emergency department are
not included in this objective
Threshold: > 50%
Providers need only to record the
indication that an advance
directive exists
Electronic Notes
Objective
Record electronic notes in patient records.
Denominator
New objective
Number of unique patients admitted to the EH or CAH’s inpatient or
emergency department (POS 21 or 23) during the EHR reporting
period.
Numerator
Number of patients in the denominator who have at least one
electronic progress note from an authorized provider of the EH or
CAH’s inpatient or emergency department (POS 21 or 23) recorded as
text searchable data.
Threshold: > 30%
Text must be searchable
Drawings and other content can
be included with searchable text
notes
Imaging Results
Objective
Imaging results consisting of the image itself and any explanation or
other accompanying information are accessible through CEHRT.
Denominator
New objective
Number of tests whose result is one or more images ordered by an
authorized provider on behalf of the EH or CAH for patients admitted
to its inpatient or emergency department (POS 21 or 23) during the
EHR reporting period.
Numerator
No limitations on the
resolution of the image
Number of results in the denominator that are accessible through
CEHRT.
Threshold: > 10%
Native storage of the image is not
required; images can be scanned
into CEHRT
Family Health History
Objective
Record patient family health history as structured data.
Denominator
New objective
Number of unique patients admitted to the EH or CAH’s inpatient or
emergency department (POS 21 or 23) during the EHR reporting
period.
Numerator
Number of patients in the denominator with a structured data entry
for one or more first-degree relatives.
First-degree relatives include
parents, siblings, and
offspring
Threshold: > 20%
When applicable, structured data
entry of “Unknown” is acceptable
ePrescribing (eRX)
Objective
Generate and transmit permissible discharge prescriptions
electronically (eRX).
Denominator
Number new, changed, or refill prescriptions written for drugs
requiring a prescription in order to be dispensed other than
controlled substances for patients discharged during the EHR
reporting period.
New objective
Numerator
Number of prescriptions in the denominator generated, queried for a
drug formulary and transmitted electronically.
Threshold: > 10%
Electronic transmissions
within and outside the
organization should be
included
Lab Results to Ambulatory Providers
Objective
Provide structured electronic lab results to ambulatory providers.
Denominator
New objective
Number of electronic lab orders received.
Numerator
Number of structured clinical lab test results sent to the ordering
provider.
Threshold: > 20%
Methods that have no potential
for automatic incorporation, such
as “Portal View” do not count
Order must be sent electronically from
the ordering provider in such a way
that the hospital lab does not have to
print a hard copy of the order to view it
Clinical Quality Measures (CQM)
Requirement
EHs & CAHs must report on 16 of 29 approved CQMs. Selected CQMs
must cover at least 3 of the 6 National Quality Strategy domains:
Patient & Family Engagement
Patient Safety
Care Coordination
Population & Public Health
Efficient Use of Healthcare Resources
Clinical Processes/Effectiveness
Must report on 16 of 29
approved measures
Reporting
All CQMs will be submitted electronically to CMS
Electronic submission is
required beginning in 2014
To Review…
•
Stage 2 Objectives
•
16 Core
•
3 of 6 Menu
•
Clinical Quality Measures
•
3 Month Reporting Period in 2014
Must be completed by September 30th
•
•
•
Can begin no later than July 1
Payment Adjustments begin in 2015
•
Start no later than April 1 to avoid adjustments
To Review…
Core Objectives
CPOE for Med, Lab, Rad Orders
Demographics
Vital Signs
Smoking Status
Menu Objectives
Advance Directives
Electronic Notes
Imaging Results
Clinical Decision Support Rules
Family History
Patient Electronic Access
eRX
Privacy & Security
Lab Results to Ambulatory Providers
Clinical Lab Test Results
Patient List
Educational Resources
Medication Reconciliation
Summary of Care
Immunization Registries
Reportable Lab Test Results
Syndromic Surveillance
eMAR
Clinical Quality Measures
Report on 16 of 29
Speaker Information
Natalie Stewart, MBA
Managing Advisor, Meaningful Use
Purdue Healthcare Advisors
nmstewart@purdue.edu
(765) 496-1265 (phone)
(765) 496-6990 (fax)
www.pha.purdue.edu
healthcareadvisors@purdue.edu
Visit us on
@ Purdue Healthcare Advisors