hyperparathyroidism in chronic kidney disease
advertisement

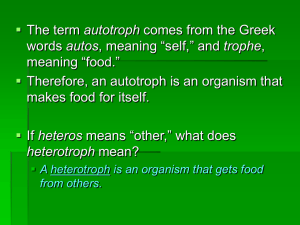
Hyperparathyroidism in Chronic Kidney Disease 醫五 李政霆 Three major possible targets regulate parathyroid gland function • G-protein-coupled calcium-sensing receptor (CaSR) • Vitamin D receptor (VDR) • Putative extracellular phosphate sensor Kidney failure 1. Decreased renal excretion of phosphate and diminished renal hydroxylation of 25hydroxyvitamin D to calcitriol (1,25dihydroxyvitamin D). 2. Disrupts systemic calcium and phosphate homeostasis and affects the bone, gut, and parathyroid glands. Hypocalcemia and the calciumsensing receptor 1. CaSR: Which is highly expressed in the parathyroid glands 2. The fall in serum calcium concentration with renal failure, as sensed by the CaSR, is a potent stimulus to the release of PTH Decreased vitamin D levels 1. Vitamin D stimulates intestinal phosphate absorption 2. Decrease in active vitamin D production may be viewed as an adaptive response to minimize hyperphosphatemia Hyperphosphatemia 1. A novel phosphaturic factor, FGF23, may be regulated by phosphate and vitamin D 2. Lowers the levels of ionized calcium, interferes production of 1,25dihydroxyvitamin D, resulting in increased PTH levels Renal osteodystrophy 1. Osteitis fibrosa cystica (a) Increased bone turnover activity (b) Bone pain and increased risk of fracture 2. Adynamic bone disease (a) Decreased bone turnover activity (b) Excess suppression of parathyroid gland therapies, particularly Ca-containing phosphate binders and vitamin D analogues Calciphylaxis eMedicine Calciphylaxis eMedicine Figure 1. The factors involved in the pathogenesis of secondary hyperparathyroidism Martin, K. J. et al. J Am Soc Nephrol 2007;18:875-885 Copyright ©2007 American Society of Nephrology K/DOQI Recommendation Plasma PTH Serum Ca Serum P Ca*P Stage3 35 to 70 pg/mL 8.4 to 10.4 2.7 to 4.6 <55 mg/dL mg/dL mg2/dL2 Stage4 70 to 110 pg/mL 8.4 to 10.4 2.7 to 4.6 <55 mg/dL mg/dL mg2/dL2 Stage5 150 to 300 8.4 to 9.5 pg/mL mg/dL 3.5 to 5.5 <55 mg/dL mg2/dL2 Management of secondary HPT in dialysis patients • Phosphate binders (calcium or noncalcium containing binders) • Vitamin D analogues • Calcium supplementation and/or a calcimimetic Stepped strategy • Normalizing serum phosphate levels • Limiting excessive calcium loading • Using a calcimimetic in patients with elevated PTH levels • Avoiding high dose active vitamin D analog administration and reducing vitamin D analog dose in patients with suppressed PTH levels Step 1 • Measure serum calcium, albumin, phosphate, 25(OH) vitamin D and intact PTH levels Step2 • Treating hyperphosphatemia without causing hypercalcemia * Hyperphosphatemia is associated with: a. Increased mortality in ESRD b. Phosphate is the principal factor leading to calcification Step 2 (I) P <5.5 mg/dL and Ca <9.5 mg/dL: 1.Calcium-based phosphate binders, either calcium carbonate or calcium acetate should be started 2.Keeping daily elemental calcium intake from binders to less than 1500 mg, and total elemental calcium from diet and binders to less than 2000 mg. Step 2 (II) P <5.5 mg/dL and Ca >9.5 mg/dL : No phosphate binder is necessary. (III) P >5.5 mg/dL and Ca >9.5 mg/dL : A non-calcium containing phosphate binder should be used Step 2 (IV) P >5.5 mg/dL and Ca <9.5 mg/dL : 1. Calcium-based phosphate binder used 2. Adding a non-calcium containing phosphate binder if phosphate remains above 5.5 mg/dL Step 3 • Decide whether phosphate binder therapy is sufficient or whether a calcimimetic or vitamin D analogue should be added : 1. If PTH<300 pg/mL,no additional therapy needed 2. If PTH>300 pg/mL with binder therapy, the choice is either cinacalcet or vitamin D analogues Step 3 • If the calcium and phosphate levels are both toward the upper limit: starting cinacalcet • If the calcium level is near or below the lower limit and the phosphate is well within the normal range: Vitamin D should be used • Cinacalcet: Suppressing serum PTH levels without raising the Ca x P product • Vitamin Danalogues: Induce hyperphosphatemia, hypercalcemia and promote vascular calcification at high doses • P >5.5 mg/dL and Ca >8.4 mg/dL P <5.5 mg/dL and Ca >9.5 mg/dL Use Cinacalcet • P <5.5 mg/dL and Ca <9.5 mg/dL Use vitamin D analogue Step 4 • Adjust the doses of phosphate binders, active vitamin D, and cinacalcet to attempt to attain K/DOQI target values