The Quality Improvement
Journey: From TQM to QI
HIVQUAL Workshop
June 24, 2011
Dan Belanger Terry Hamilton Lawrence Hansley
1
Agenda
Welcome and Introductions
SWOT Analysis Small Group Exercise
Total Quality Management
Key Tools and Techniques
Origins of Quality Management
Histogram Small Group Exercise
Continuous Improvement
6 Sigma
Lean
Lean Small Group Exercise
The Model for Improvement
2
Ice Breaker: SWOT Analysis
Small Group Exercise
Your HIV QM Committee is considering
adding consumers to the HIV QM
Committee
To understand the pros and cons you
decide to do a SWOT Analysis (strengths,
weaknesses, opportunities and threats)
Using the worksheet in your packet, each
group brainstorms a SWOT analysis and
reports back
3
Quality Roots
The roots of Total Quality Management
can be traced to early 1920's
production quality control ideas, and
concepts developed in Japan
beginning in the late 1940's and
1950's, pioneered there by Americans
Feigenbaum, Juran and Deming
4
Total Quality Management (TQM)
Total Quality Management features:
the customer-supplier interfaces, (external and
internal customers and suppliers)
an organizational commitment to quality
the importance of communicating this quality
commitment
the acknowledgement that the right
organizational culture is essential for effective
Total Quality Management
5
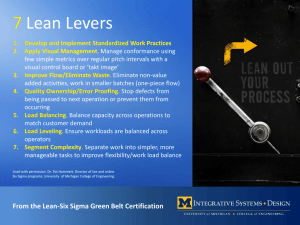
Tools and Techniques
An array of tools and techniques is used for
identifying, measuring, prioritizing and
improving processes critical to quality
6
Process Improvement Tools
These process improvement tools and
techniques include:
PDSA (plan, do, study, act) Cycle
Flow-charting
Cause and effect diagram,
Brainstorming
Pareto Analysis
7
The PDSA cycle
for learning and improvement
Act Plan
Objective
What changes Questions and
are to be made? predictions (why)
Next cycle? Plan to carry out the cycle
(who, what, where, when)
Study
Complete the
analysis of the data
Compare data to
predictions
Summarize what
was learned
Do
Carry out the plan
Document problems
and unexpected
observations
Begin analysis of
the data
8
Flow Charts
Purpose: Graphic depiction of how a
process works
Use: 1) visualize and understand a
process;
2) consider ways to simplify;
3) recognize unnecessary steps;
4) identify who will be involved in or
effected by improvement process
Caution: 1) flowchart must reflect
real process;
2) people who know the process
must be involved;
3) be sure the flowchart focuses on
the identified problem
Commonly Used Flow Chart Symbols:
Terminator
Task or Step
Decision
Wait symbol
9
Flow Chart Example
Client Arrives at Drop-In Center
Patient arrives at front desk
Front Desk Staff Asks Client for Name
& Searches Database
Client in system?
YES
NO
Receptionist asks client
to complete paperwork for new clients
and return it to front desk
Ask client to be seated in the
Waiting room
ETC.
HR Counselor
takes client into
Counseling Room
10
CAUSE-AND-EFFECT DIAGRAM
SAMPLE
Skeleton
Equipment
Environment
Computer
System down
for routine
maintenance
Low show rate
for appointments
Patients
Procedures
People
Patient unaware
of appointment
11
Brainstorming
Purpose: To provide a freewheeling
environment in which everyone is
encouraged to participate.
Use:
generate new ideas/insights
draw out experiences of each
participant
when creative ideas have been
suppressed by group
Caution:
ideas will need elaboration
discussion impedes & limits flow of
ideas
12
Feigenbum, Juran and Deming
Quality Management resulted mainly from the
work and theories of Americans who took the
messages of quality to Japan in the 1950's:
Joseph Juran
W Edwards Deming
Armand Feigenbaum
13
W Edwards Deming
placed great importance and
responsibility on management, at both the
individual and company level, believing
management to be responsible for 94% of
quality problems.
14
Deming’s
14 Point Management Plan
Create constancy of purpose towards
improvement of product and service
Adopt the new philosophy. We can no longer
live with commonly accepted levels of delay,
mistakes and defective workmanship
Cease dependence on mass inspection.
Instead, require statistical evidence that
quality is built in
End the practice of awarding business on the
basis of price
15
Deming’s 14 Point Plan Continued
Find problems. It is management’s job to
work continually on the system
Institute modern methods of training on the
job
Institute modern methods of supervision of
production workers, The responsibility of
foremen must be changed from numbers to
quality
16
Deming’s 14 Point Continued
Drive out fear, so that everyone may work
effectively for the company
Break down barriers between departments
Eliminate numerical goals, posters and
slogans for the workforce asking for new
levels of productivity without providing
methods
17
Deming’s 14 Point Continued
Eliminate work standards that prescribe
numerical quotas
Remove barriers that stand between the
hourly worker and their right to pride of
workmanship
Institute a vigorous program of education and
retraining
Create a structure in top management that
will push on the above points every day
18
Dr Joseph M Juran
developed the quality trilogy – quality planning,
quality improvement and quality control.
Good quality management requires quality actions
to be planned out, improved and
controlled.
The process achieves control at one level of quality
performance, then plans are made to improve the
performance on a project by project basis, using
tools and techniques such as Pareto analysis.
This activity eventually achieves breakthrough to an
improved level, which is again controlled to prevent
any deterioration.
19
Pareto Chart
Purpose
Compare the various factors that contribute to an
overall effect.
Indentify the “vital few” (factors that, warrant the
most attention) from the “useful many” (factors that,
while useful to know about, have relatively smaller
effect).
Based on the Pareto Principle which suggests that
most effects are the result of relatively few causes,
that is, approximately 80% of effects come from 20%
of potential causes.
Analyzing Data
20
Analyzing Data
21
Juran
Juran believed quality is associated with
customer satisfaction and dissatisfaction with
the product
emphasized the necessity for ongoing quality
improvement through a succession of small
improvements
projects carried out throughout the
organization.
22
Juran’s 10 Points to QI
Build awareness of the need and opportunity
for improvement
Set goals for improvement
Organize to reach the goals
Provide training
Carry out projects to solve problems
23
Juran’s 10 Points to QI Continued
Report progress
Give recognition
Communicate results
Keep score of improvements achieved
Maintain momentum
24
Armand V Feigenbaum
Feigenbaum was the originator of “total
quality control”, often referred to as total
quality.
25
Feigenbaum’s Definition of Total
Quality Control
“An effective system for integrating quality
development, quality maintenance and
quality improvement efforts of the various
groups within an organization, so as to
enable production and service at the most
economical levels that allow full customer
satisfaction”.
26
Feigenbaum’s 3 Steps to Quality:
Quality leadership
Modern quality technology
Organizational commitment
27
Late 1950’s Japanese who developed new concepts in
response to the Americans
Dr Kaoru Ishikawa
Shigeo Shingo
Dr Genichi Taguchi
28
Ishikawa’s 7 Basic Tools of Quality
Pareto analysis which are the big problems?
Cause and effect diagrams what causes the
problems?
Stratification how is the data made up?
Check sheets how often it occurs or is done?
Histograms what do overall variations look like?
Scatter charts what are the relationships between
factors?
Process control charts which variations to control
and how?
29
Cause-and-Effect Diagram
Organizes and displays all causes and sub-causes that
may influence a problem, outcome, or effect
Helps push people to think beyond the obvious causes,
(money, time) to find some causes that they can
fix/improve
Helps organize potential solutions and make clear who
should be involved in solutions
Encourages a balanced view
Demonstrates complexity of the problem
30
Cause and Effect Diagram of
HIV-infected Homeless Youth
Not Receiving HIV Primary Care
Individual factors
Individual factors
Individual factors
Poor Resources
History of physical/emotional/
sexual abuse
Sexual
minority
Survival sex
Low educational
attainment
Unstable
Housing
Drug/Alcohol abuse
Family conflict/neglect/
abandomnment
Low
Self-efficacy
Poor condom use
Foster care system
Mental health
disorder
Poor condom use
Poor access to
resources
Incarceration
Stigma
Laws
Violence
Discrimination
Policies
Economics
Poor access to resources
Social factors
Social Factors
31
31
Histograms
Purpose
Used to display the variation in continuous data
like time, weight, size or temperature
Helps teams recognize and analyze patterns in
data that are not apparent simply by looking at a
table of data, or by finding the average or median
32
What’s our Pattern Here?
Group Discussion
(10 Minutes)
Number of days for follow-up GYN appointment
Source: Institute for Healthcare Improvement
Analyzing & Displaying Data
33
Shigeo Shingo
Associated with Just-in-Time manufacturing,
The Use of a checklist- humans can forget or make
mistakes
the inventor of
the single minute exchange of die (SMED) system, in
which set up times are reduced from hours to minutest
Poka-Yoke (mistake proofing) system. In Poka Yoke,
defects are examined, the production system stopped and
immediate feedback given so that the root causes of the
problem may be identified and prevented from occurring
again.
34
The Mistake Proofing System
Shingo distinguished between “errors”, which
are inevitable, and “defects”, which result
when an error reaches a customer
the aim of Poka-Yoke is to stop errors from
becoming defects.
Defects arise because errors are made and
there is a cause and effect relationship
between the two.
35
Dr Genichi Taguchi
believed it is preferable to design
product that is robust or insensitive to
variation in the manufacturing process, rather
than attempt to control variations during
actual manufacture
36
Taguchi’s 3 Quality Stages
System design
Parameter design
Tolerance design
37
Kaizen or Continuous Improvement
The aims of a Kaizen organization are
typically defined as:
To be profitable, stable, sustainable and
innovative.
To eliminate waste of time, money, materials,
resources and effort and increase productivity.
To make incremental improvements to systems,
processes and activities before problems arise
rather than correcting them after the event.
To create a harmonious and dynamic organization
where every employee participates and is valued.
38
Key concepts of Kaizen
Everyone involved in a process or activity,
however apparently insignificant, has
valuable knowledge and participates in a
working team or Kaizen group
Everyone is expected to participate,
analyzing, providing feedback and suggesting
improvements to their area of work.
39
Key concepts of Kaizen continued
Every is a key word in Kaizen: improving
everything that everyone does in every
aspect of the organization in every
department, every minute of every day.
Evolution rather than revolution: continually
making small, 1% improvements to 100
things is more effective, less disruptive and
more sustainable than improving one thing by
100% when the need becomes unavoidable.
40
Key concepts of Kaizen
Every employee is empowered to participate
fully in the improvement process: taking
responsibility, checking and co-coordinating
their own activities. Management practice
enables and facilitates this.
Every employee is involved in the running of
the company, and is trained and informed
about the company. This encourages
commitment and interest, leading to
fulfillment and job satisfaction.
41
The Quality Circle
The idea of the quality circle was first
introduced by Japanese business as a
way to involve all employees in their
organization’s quality program.
42
Quality Circles
A quality circle is a group of 3 to 12 coworkers who agree on a volunteer basis to
meet together regularly to identify and
analyze problems and to brainstorm solutions
Solutions are presented to management
Quality Circle participants in some cases may
implement solutions
43
1970’s-1980’s Western Gurus:
Philip B Crosby
Known for the concepts of
“Quality is Free”
“Zero Defects”,
4 Absolutes of Quality
44
Crosby’s 4 Absolutes of Quality
Quality is conformance to requirements
The system of quality is prevention
The performance standard is zero defect
The measurement of quality is the price of
non-conformance
45
Tom Peters
identified leadership as being central to
the quality improvement process, discarding
the word
“Management” for “Leadership”.
The new role is of facilitator, and the basis is
“Managing by walking about” (MBWA),
enabling the leader to keep in touch with
customers, innovation and people, the three
main areas in the pursuit of excellence.
46
Tom Peters
believes that, as the effective leader
walks, at least 3 major activities
are happening:
Listening suggests caring
Teaching values are transmitted
Facilitating able to give on-the-spot help
47
Framework for Measuring Healthcare
Quality
In 1966 Avedis Donabedian developed the
first conceptual framework to measure the
quality of healthcare
Measure quality by assessing structures,
processes, outcomes of care
48
National Health Service (UK)
NHS Improvement has over 10 years
improvement experience
Use practical knowledge and “how to”
approach to help improve the quality and
productivity of services
Use innovative approaches as well proven
improvement methodology.
Integrates sociological concepts into
improvement work
49
Six Sigma
Since the 1920's the word 'sigma' has been
used by mathematicians and engineers as a
symbol for a unit of measurement in
product quality variation
3.4 parts - or defects - per million
In the mid-1980's engineers in Motorola Inc
in the USA used 'Six Sigma' as a name for
an in-house initiative for reducing defects
in production processes
50
Motorola
In the late-1980's following the success of
the above initiative, Motorola extended the
Six Sigma methods to its critical business
processes
in-house 'branded' name for a performance
improvement methodology
51
Motorola’s Definition of Six Sigma
"...Six Sigma has evolved over the last two decades
and so has its definition. Six Sigma has literal,
conceptual, and practical definitions. At Motorola
University (Motorola's Six Sigma training and
consultancy division), we think about Six Sigma at
three different levels:
As a metric
As a methodology
As a management system
Essentially, Six Sigma is all three at the same time."
52
Six Sigma Methodology
Understanding and managing customer
requirements
Aligning key business processes to achieve
those requirements
Utilizing rigorous data analysis to minimize
variation in those processes
Driving rapid and sustainable improvement to
business processes.."
53
Six Sigma Leaders and Teams
Six Sigma team leaders (Black Belts) work
with their teams (team members will normally
be people trained up to 'Green Belt'
accreditation) to analyze and measure the
performance of the identified critical
processes.
54
the DMAIC model for process
improvement.
DMAIC is commonly used by Six Sigma project
teams and is an acronym for:
Define opportunity
Measure performance
Analyze opportunity
Improve performance
Control performance.."
55
DMAICT process elements
D - Define opportunity
M - Measure performance
A - Analyze opportunity
I - Improve performance
C - Control performance, and optionally:
T - Transfer best practice (to spread the
learning to other areas of the organization)
56
HHCs Past
HHC examples…
Chronic Care Collaboratives
Ambulatory Care Redesign
1,000,000 Lives Campaign
57
BREAKTHROUGHHHCs Improvement System
History of Lean
Kaizen
Driven by metrics to right
size
Staff teams
Value=
What the customer wants
58
Rapid Improvement Event- (R.I.E.)
Hallmarks
Planned, team-based event
Fresh-eyes and pros
1 wk, intensive, facilitated
Specific follow-up to sustain
59
Breakthrough- Impact at HHC
From
start to now, ~$150 million
in revenue or decreased
expenses
≥ 8,800 employees have
participated
~700 R.I.E.s
60
TOOLS We Know
Pick Chart
Pareto Chart
Root Cause Analysis
PDSA
Brainstorming
61
A3
STORY
9
Paper and pencil!
boxes
Eliminate MUDA or Waste
62
A3 Boxes
1
Reason for Action
succinct problem statement,
burning platform
2
Initial State
where you are now
3
Target State
where you want to be
4
Gap
Analysis
difference between boxes 3
and 4
5
Solution approach
ideas/ways for closing the
gaps
6
Rapid Experiments
tests of the Solution
Approaches
7
Completion Plan
what is left to do after the RIE
week
8
Confirmed State
how achievement of Target
State is measured
9
INSIGHTS
63
8 Wastes
1.
2.
3.
4.
5.
6.
7.
8.
Over Production
Waiting
Transport
Extra Processing
Inventory
Motion
Defects
Unused Human Potential
64
6S
Sort
Straighten
Scrub
Safety
Standardize
Sustain
65
5 Why’s
Why?
Why?
Why?
Why?
Why?
Determines Root Cause
66
Just Do It
Type of improvement activity.
Solution is known.
Does not require R.I.E.
Put in place with limited resources
67
Exercise 1
Increase clinician participation in monthly QI
meeting by 10%
1
Reason for Action
Increase clinician
participation in monthly
QI meeting
2
Initial State
3
Target State
4
Gap
Analysis
5
Solution approach
6
Rapid Experiments
7
Completion Plan
8
Confirmed State
9
INSIGHTS
68
PICK ChartDo the High Benefit / Low Difficulty actions now
! Identify Actions then and
group into
P
BENEFIT
DIFFICULTY
6
Possible
High Benefit, Easy to Do.
Implement Now
C
9
7
Impac
t
Implement
1
2
High benefit, Make a plan how to do
it.
I
4
Challenge
I P
C K
Low benefit, but easy to do
K
Kick Out
5
3
8
Low benefit and difficult to do.
Kick it out !
Difficulty
69
Exercise II
Pick Chart
a.
Increase by 15% the number of
MSM who have at least 4 kept
medical appointments during the
year.
b. Engage 3 consumers 2x each
month in QI planning activities.
70
Summary
QI
is a strategy
Many tools
Many opportunities
Just Do It!
71
Model for Improvement
Developed by Associates in Process
improvement
Simple elegant
Captures the central concepts and core
principles of Quality improvement in a clear,
concise fashion
72
Model for Improvement
What are we trying
to accomplish?
How will we know that a
change is an improvement?
What change can we make that
will result in improvement?
Act
Plan
Study
Do
Model
for
Improvement
73
Conclusion
The same basic principles guide Quality
Improvement and Quality Management
Methodologies
The specific methodology used is not as
important as the commitment to quality
improvement principles, taking action and
improving the quality of care
74
Resources
Bruce Agins,MD
Clemens Steinbock
Kevin Garrett
Alan Chapman 2004-2009
Institute for Healthcare Improvement
The Economist Newspaper Copyright 2011
Associates in Process Improvement
www.Businessballs.com
National Health Service, www.improvement.nhs.uk
Copyright 1994-2005 Motorola, Inc.
Toyota Production Systems
Mark R. Chassin and Jerod M. Loeb, The Ongoing Quality
Improvement Journey: Next Stop, High Reliability Health Affairs on
April 25, 2011
75
Further Reading
Beckford, J., “Quality: A Critical Introduction”, Routledge,
London, 1998; 4th edn, 2002
Crosby, P., “Quality is Free: The Art of Making Quality
Certain”, McGraw-Hill, 1979
Ishikawa, K., “What is Total Quality Control?
The Japanese Way”, Prentice Hall, 1985
Juran, J., “Juran on Planning for Quality”, Free Press, New
York, and Collier Macmillan, London, 1988
76
Special Thanks to…
Terry Hamilton
Lawrence Hansley
HHC
77
And…
Thank you!!!!
78