Lange
advertisement

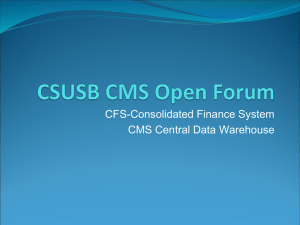
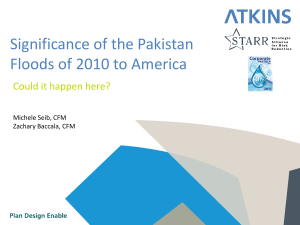
Neurocognitive Manifestations in ME/CFS Gudrun Lange, PhD Professor Department of Physical Medicine and Rehabilitation, Rutgers-NJMS Outline • Why is it important to talk about cognitive function in ME/CFS? • What is the clinical presentation? • How can cognitive dysfunction in ME/CFS be understood? • What is an effective neuropsychological battery? • What is the research evidence? • Final thoughts Brainfog: Common and Disabling • Experienced as difficulties with attention, concentration and multi-tasking • Recognized as important: Listed as symptom in all ME/CFS case definitions • Serves as objective criterion for disability: lack of validated physiological markers Clinical Presentations • “I feel like I’m loosing my mind…” • “I feel like having the brain of an 80-year old in the body of a 36-year old…” • “I feel stupid…” Conceptualization of Cognitive Dysfunction • Possible etiology of cognitive dysfunction • Genetic • Acquired • Severity of cognitive dysfunction • Severe • Moderate • Mild Determination of Severity of Cognitive Dysfunction • Subjective • Patient and family report • Perception of degree of loss of cognitive function • Objective • Neuropsychological evaluation • Statistical determination of degree of loss of cognitive function • Behavioral observations during testing should be taken into consideration An effective neuropsychological battery for ME/CFS patients • Has to include standardized and normed measures that • Sufficiently and repeatedly challenge complex information processing and multitasking • reliably demonstrate areas of cognitive resilience • assess mood and anxiety • ascertain adequate effort Intellectual profiles in ME/CFS WAIS-IV profile: Scores discrepant from expected levels Case 1 Case 2 Case 1 Analysis Subtest Scaled Score Profile The vertical bars represent the standard error of measurement (SEM) Index Level Discrepancy Comparisons Score 1 Score 2 Difference Critical Value .05 VCI - PRI VCI - WMI VCI - PSI PRI - WMI 112 112 112 94 94 77 65 77 18 35 47 17 7.78 8.31 11.76 8.81 Y Y Y Y 9.5 0.5 1 9.2 PRI - PSI WMI - PSI 94 77 65 65 29 12 12.12 12.47 Y N 3 20.2 Comparison Significant Difference Y/N Base Rate Overall Sample Case 2 Analysis Index Level Discrepancy Comparisons Score 1 Score 2 Difference Critical Value .05 VCI - PRI VCI - WMI VCI - PSI PRI - WMI 114 114 114 107 107 111 97 111 7 3 17 -4 8.31 8.82 10.19 9.74 N N Y N 30.3 45.7 19.4 36.2 PRI - PSI WMI - PSI 107 111 97 97 10 14 11 11.38 N Y 35.9 23.7 Comparison Significant Difference Y/N Base Rate Ability Level • Clinical Interview • Wechsler Adult Intelligence Scale - Fourth Edition (WAISIV) • Test of Premorbid Functioning (TOPF) • Beck Depression Inventory II (BDI II) • Spielberger State Trait Anxiety Questionnaire (STAI) • Gordon Diagnostic Test • Stroop Test • DKEFS • Trails • Verbal Fluency Test • Paced Auditory Serial Attention Test (PASAT) • Wisconsin Card Sorting Test (WCST) • California Verbal Learning Test II (CVLT-II) • Wechsler Memory Scale Fourth Edition (WMS-IV) • Boston Naming Test (BNT) • Rey Osterrieth Complex Figure (ROCF) • Judgment of Line Orientation Test (JOL) • Hooper Visual Organization Test • Hand Dynamometer • Grooved Pegboard • Finger Tapping Test (FTT) • Validity Indicator Profile (VIP) Findings on neuropsychological exam • Decreased attention, concentration and slowed processing speed • Problems sequencing pieces of information and prioritizing their use for quick decision making • Limited working memory, • less information available “online” • Learning difficulties: • Changes in learning strategy • Poor absorption and recall Neuropsychological Profile in ME/CFS • Profile suggests mild, subtle deficits • Evaluation of impairment relative to expected level of intellectual function necessary to uncover true deficiencies • Profile not consistent with dementia • Generally no frank memory problem • Profile can be differentiated from conditions of a more focal nature Brain Abnormalities in ME/CFS • Lange et al., 2005 • Used verbal working memory task to • probe brain function using fMRI • simultaneously assessing efficient information processing behaviorally • Statistically controlled for age, mood, anxiety, self-reported mental fatigue score • Equated on prior behavioral test performance on same task Brain Abnormalities in ME/CFS • Controls versus ME/CFS: • No differences in brain activity during simple condition • When task demands get more complex, ME/CFS increased involvement of • Anterior Cingulate BA 24/32 • Left DLF BA 10/44/45/47 • Bilateral supplemental and premotor BA6/8 • Parietal regions BA 7/40 Brain Abnormalities in ME/CFS Brain Abnormalities in ME/CFS • Increased signal change was significantly accounted for by ME/CFS report of mental fatigue • Perceived mental fatigue is reflected by increased functional recruitment of • Left superior parietal region (BA7) • Responsible for shifts in attention • Bilateral supplementary and premotor regions (BA6/8) • Associated with automatic information processing • maintenance of temporal order Brain Abnormalities in ME/CFS • No lack of effort accounted for the differences in signal change • To achieve behavioral performance similar to Controls • Brains of ME/CFS work harder when tasks are complex • Require efficient and quick information processing • Require effective online sequencing and prioritization Consequences of cognitive dysfunction in ME/CFS • Automaticity of cognitive function is often lost • Mundane tasks become effortful • Multi-tasking often impossible • Considered by patients as affecting every aspect of their lives • Mental exertion can last for a long time Is there an effective cognitive screen for ME/CFS patients? • Dementia screens and typical brief bedside memory tests are not appropriate • i.e. MMSE, Mini-Cog • Suggestions: • Serial 7s, Digit Span Sequencing • May work if done for at least a few minutes • Quickly give a 6-or-7 step set of complex driving directions and request repetition Final thoughts • If evaluation of cognitive function is needed • Refer to Clinical Neuropsychologist knowledgeable about ME/CFS • Much more work is needed to familiarize Neuropsychologists with ME/CFS to provide valid and reliable neuropsychological assessments.