Mayo Clinic Children*s Center Introducing the
advertisement

Facing the Death of a
Child:
Perinatal and Pediatric
Palliative Care and
Support
Joanne Cacciatore, Ph D, MSW, FT
Angela O’Neil, MD
Introductions. . .
It always starts with a story. .
Karla &
Theo’s
Love Story.
...
Abnormal
What do you wish would
have been done
differently?
How information is given.
Testing
Who should give information?
With or without
parent input?
{ Parent concerns
People who have not had a child die cannot
understand that.
They can try to understand, they can attempt to
imagine what it’s like, they can absolutely be
helpful and supportive and witness our pain
without trying to change it.
But they cannot know.
Children with Life-Threatening
Conditions
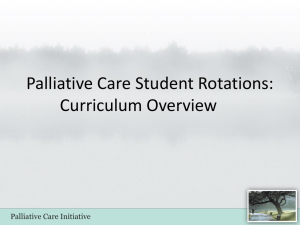
Epidemiology of Childhood
Death
2011 data 6.9 million children died
(2.6 million/yr stillbirths)
73% infants <1 (n=5m)
52% stillbirth (n=2.6m)
20% within first 24 hrs (n=975k)
14% between 1-30 days (n=732k)
14% between 1 -12 mo (n=732k)
7.5% age 1-4 (n=516k)
5.3% age 4-9 (n=365k)
14.2% age 9-19 (n=980k)
Infant/Child Death
<Age 1
1 to 4
4 to 9
9 to 19
Froen, Cacciatore, et al., 2011. The Lancet Series; Carter, Levetown and Friebert. Palliative
Care for Infants, Children and Adolescents. Second Edition. 2011.
Effect of Palliative Care in
the Hospital
Increased hospice discussion (22%
more)
Earlier DNR order (6 days)
Fewer deaths in the ICU (16% less)
Child suffered less pain (19%)
Parents felt more prepared during
child’s last month of life and at
death
Wolfe, J, Hammel JF, Edwards KE, Duncan J, Comeau M, Breyer J, et al: Easing of suffering in children with
cancer at the end of life: is care changing? J Clin Oncol 26(10):1717-1723, 2008.
Active, total care of child’s body, mind and spirit
Begins when illness is diagnosed
Continues regardless of whether or not a child
receives treatment directed at the disease
Address physical, psychological & social distress
Multidisciplinary approach
Provided anywhere, including the home
{
WHO Definition of
Palliative Care
WHO Definition of
Palliative Care
Appropriate for children and families with lifethreatening illness
Enhances quality of life
Intends to neither hasten or postpone death
Any child with life limiting disorder
To have care of Palliative Care teamThe child does NOT need to be:
Dying or actively dying
On Hospice
“Giving up hope” or “Doing nothing”
DNR and/or DNI
Who Should Get a Peds
Pallliative Care consult?
The child can be:
Receiving curative treatment
Receiving complex care
Hoping for a miracle
Local or long distance patient
Why consult Palliative care
early?
Serious illness affects:
Patient quality of life
Sibling growth, development, and behavior
Parental quality of life (esp bereavement)
Interpersonal relationships
Finances and career
Family structure
Structure of home
Individual and collective stress levels
Effect of Critical Illness on
Parents
Altered parental role
Fear of child’s suffering
Fear of child’s death
Unknown long term outcome
Inconsistent information
Minimal communication
Interpersonal relationships
Concerns over economic outcomes
Needle, JS, O’Riordan, M, Smith, PG. Parental anxiety and medical comprehension within 24 hours of
a child’s admission to the PICU. Pediatric Crit Care Medicine 10(6), 2009, 668-674.
Perinatal Palliative Care Program
Goals
• To help families understand the diagnosis and
probable outcomes for their baby
• To help families make decisions based on the
love that they have for their baby
• To assist families in cherishing the time
between the diagnosis and death of their baby
• To honor the unique and special qualities of
each baby
• To emphasize the quality of life over the
quantity of life
• To reduce the emotional, spiritual and
psychosocial suffering using interventions
sensitive to cultural, religious and personal beliefs
Palliative Care Team
Services are additive to care already in progress
Supportive, not a substitute
How can we help? -How can we help the FAMILY?
Focus on psychosocial dimension, ethical end of life decision
making and alleviation of distressing symptoms
Continuity of care
Palliative Care Team
Perinatal Palliative Care
Fetal or neonatal diagnosis of life limiting anomaly
Extreme prematurity (22-24 6/7 week gestation) wishing to pursue
comfort care
Critically ill neonates refractory to medical treatment
Pediatric Palliative Care
Terminal diagnosis of life limiting disorder or disease
Treatment and management of pain
Disclosure
Palliative Care Team
Interdisciplinary Team Members
Doctor
Nursing
Child Life
Chaplain or other spiritual leader
Psychology
Social Work
Tripartite ATTEND Model
Clinician
‐Relationship focus
‐Self focus
Therapeutic
Relationship
Client/Patient
‐Self focus
‐Relationship focus
“Unity is strength… when there is teamwork and
collaboration, wonderful things can be
achieved.”
-Mattie Stepanek (1990-2004)
I am a grieving mother, a bereaved mother who
chooses to continue to live.
I can only hope that my life can somehow reflect
even a small bit, the beauty and love I was so
privileged to touch when I met my son..
{
and shared in his life,
and in his death.
The love of a parent is not contingent upon the
amount of time we had with our child.
Love simply cannot be measured in time.”
Joanne Cacciatore