Progress Towards the Triple-Aim
Behavioral Health and Care Coordination
Integration
Michael W. Yogman, MD, FAAP
Susan Betjemann, LICSW
Christopher Ortengren
Yogman Pediatric Associates, Cambridge, MA
MCAAP Annual Meeting, May 1, 2014
Acknowledgements
This project was supported by a Harvard Pilgrim Quality
Grant
Thank you to the following for their help:
Mt. Auburn Community IPA, Betsy Pollock, The
Massachusetts Child Health Quality Coalition (Gina Rogers
and Rich Antonelli), Mass DPH (Marianne Beach), MCPAP,
Cambridge Health Alliance (Katherine Grimes), Sheila
Donoyan and Lisa Hoey, the staff at Yogman Pediatrics and
our Parent Advisory Group
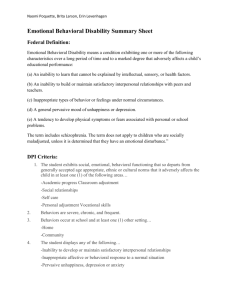
Prevalence of Child Mental Health Disorders
• National Health Interview Survey
• 7.7% of < 18 yo have disabilities that limit activity. 4-fold
increase from the 1960’s
20%
8%
Chronic Mental Health Issues in Children Now Loom Larger Than Physical Problems.”
Anita Slomski, Medical News & Perspectives, JAMA, July 2012
Prevalence of Child Mental Health Disorders
Children 3-17 yo
• ADHD–6.8%
• Behavioral or conduct
disorder–3.5%
• Anxiety–3.0%
• Depression–2.1%
• Autism spectrum–1.1%
• Tourette’s syndrome–
0.2%
Adolescents 12-17 yo
• Illicit drug use
disorder–4.7%
• Alcohol use disorder–
4.2%
• Cigarette dependence
(past month)–2.8%
NSCH 2007
NSDUH 2010-2011
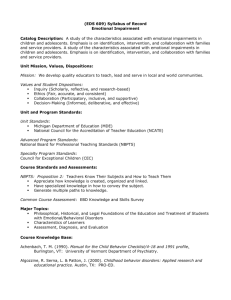
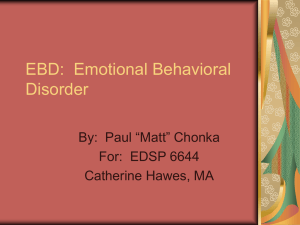
From: National Trends in the Mental Health Care of Children, Adolescents, and Adults by Office-Based
Physicians
JAMA Psychiatry. 2014;71(1):81-90. doi:10.1001/jamapsychiatry.2013.3074
Trends in
Office Based
Medical Visits
by Young
People With
Mental
Disorder
Diagnoses,
1995-2010
Figure Legend:
Trends in Office-Based Medical Visits by Young People With Mental Disorder Diagnoses, 1995-2010Analysis was limited to young
people (≤20 years). The odds ratios (ORs) and 95% CIs for the study period are for disruptive behavior disorders (OR, 2.31 [95%
CI, 1.78-2.99]), mood disorders (OR, 1.92 [95% CI, 1.40-2.64]), anxiety disorders (OR, 2.72 [95% CI, 1.71-4.32]), psychoses and
developmental disorders (OR, 2.27 [95% CI, 1.44-3.59]), and other mental disorders (OR, 1.17 [95% CI, 0.87-1.57]). Data are from
the National Ambulatory Medical Care Survey.
Copyright © 2014 American Medical
Association. All rights reserved.
Addressing the Triple-Aim
-Experience of Care
Patient Experience
• Parent Experience Surveys
• Parent Advisory Group
• Parent Stress Index
Provider and Staff Experience
• Experience Surveys
Addressing the Triple-Aim
-Quality of Care
Quality Outcomes
• Team based coordinated care between
pediatricians and social worker, “warm
handoffs”, parent education, improved access
to BH services, de-stigmatization
Addressing the Triple-Aim
-Quality of Care
Care Coordination Measurement Key Data
Summary
(September 2013 - March 2014)
• 284 recorded patient encounters
• 97 unique patients served
• 53 in office behavioral health therapy/treatment sessions
• 78 subspecialist visits prevented
• 37% patients referred to behavioral health subspecialists
• 44% of all patient encounters focused on behavioral health
• 25% of encounters involved care coordination for BH services
• 46% of encounters required further care coordination (follow
up or referral)
Addressing the Triple-Aim
-Quality of Care
Patient Population Management
• Utilizing up-to-date registry lists for patient follow-up,
targeted quality improvement, and medical cost data
(1)ADD/ADHD
(2) Autism/ASD
(3)Complex Condition
(4)Serious Emotional Disturbance
(5)Comorbid Behavioral Health and Complex Condition
(6)Early Intervention and IEP
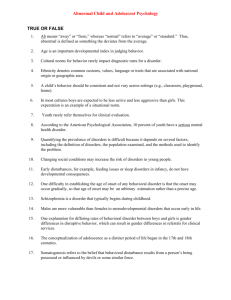
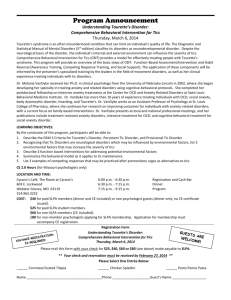
Addressing the Triple-Aim
-Cost
Patient Category
Number of
Patients
identified
Number of
Patients with
Claims Data in
2013
Average Cost per
Patient per
Month
ADD / ADHD
Autism / ASD
Complex
Condition
SED
BH & CC
comorbid
Total
Practice
102
26
66
41
11
25
$271
$762
$862
83
43
$448
48
21
$1,167
971
$168.72
Prevention
• Early Childhood
• Social emotional development, early
identification and intervention
• Family
• Parent support and psycho-education
• Group Interventions
• Targeting both children and families
• Newborn, ADHD and Overweight groups
Child Psychiatry Consultation
• Massachusetts Child Psychiatry
Access Project
• Cambridge Health Alliance
• Katherine E. Grimes, MD, MPH
Sustainability
• Payment for behavioral health care coordination
• Better reimbursement for evidenced based
behavioral treatment rather than just
psychopharmacology treatments
• Reimbursement for same-day care
• Reimbursement for post partum depression
screening
• Reimbursement for non face-to-face care
• Training and supervision of parent partners and
community health workers to provide care
coordination
“It is easier to build strong children
than repair broken men”
-Frederick Douglass