Cross Cancer Institute
advertisement

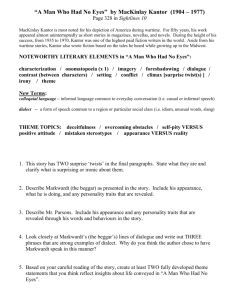
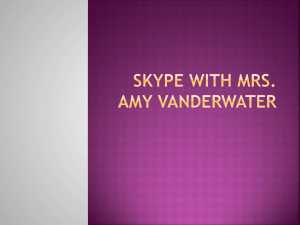
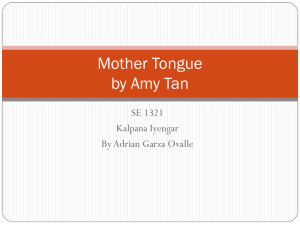
Falls Virtual Learning Session # 4 & Closing Congress Team Rapid Fire Presentation Template Cross Cancer Institute, Edmonton, Alberta Amy Kantor, Quality Consultant Join the Falls Prevention Virtual Learning Collaborative Who We Are Edmonton, Alberta Ambulatory and Inpatient Care • 3 inpatient units • ~56 beds • ~140 RN’s plus NA’s, PT, OT, RT, Pharmacists and MD’s Primary Cancer Care facility, serving all of northern Alberta. Team Members Team Member Role Nadia Kloc Inpatient Nurse Manager Carolyn Howe-Riddell Inpatient Resources Nurse Carole Szwajkowski Nursing Education Judy Poon Rehab Medicine, Physiotherapy Amy Kantor Quality Consultant AIM To lead and coordinate team learning, process and care improvements; to ensure our targeted goals are achieved in falls and injury reduction and that we contribute as active participants in the SHN Falls Prevention VLC. • Reduce incidence of falls (fall rate) by 40% from baseline (to 2.4%) by March • • 2011. Reduce injury from falls by 40% from baseline (to 19%) by March 2011. Scope: Inpatient units (3 units, 56 beds) Change Ideas Changes tested during Falls VLC PDSA Cycles: Implementation of an appropriate Assessment Tool • Initially used Schmidt tool, now working with Morse tool Inventory of mobilization equipment and aids and storage locations • Discovered shortage of transfer belts, purchasing more and moving to a more visible and accessible storage location Evaluate location of majority of falls (~60% occur in the bathroom) • Planning to trial bathroom signs encouraging patients to call for assistance Implementation of a Post-Falls Assessment Tool • Trialing and revising a tool to help discover specific reasons for falling Implement an apple as a symbol for a patient at risk of falling • To be placed outside of patients room, used for recognition and promotional ‘materials’ Measures 1: Falls Rate per 1000 Patient Days 5.00 4.50 4.00 Implemented Risk Assessment Falls/1000 days 3.50 3.00 Change in Event Reporting System 2.50 2.00 1.50 Number of Falls per Month Range: 4-7 1.00 Mean: 5 0.50 0.00 Apr 2010 May 2010 Jun 2010 Jul 2010 Aug 2010 Sep 2010 Oct 2010 Nov 2010 Dec 2010 Jan 2011 Feb 2011 Fall Rate 4.74 3.71 3.29 3.90 4.46 2.00 3.29 2.58 2.76 2.48 3.00 Goal 2.40 2.40 2.40 2.40 2.40 2.40 2.40 2.40 2.40 2.40 2.40 Month Measures Percentage of Falls Causing Injury 90.0% Implemented Risk Assessment 80.0% Change in Event Reporting System Percentage of Harmful Falls 70.0% 60.0% 50.0% 40.0% Number of Falls Causing Injury per Month 30.0% Range: 0-4 20.0% Mean: 2 10.0% 0.0% Apr 2010 May 2010 Jun 2010 Jul 2010 Aug 2010 Sep 2010 Oct 2010 Nov 2010 Dec 2010 Jan 2011 Feb 2011 CCI Data 14.3% 33.3% Goal 19.0% 19.0% 60.0% 0.0% 42.9% 60.0% 80.0% 25.0% 50.0% 50.0% 50.0% 19.0% 19.0% 19.0% 19.0% 19.0% 19.0% 19.0% 19.0% 19.0% Month Measures Percentage of Completed Fall Risk Assessment on Admission 120.0% 100.0% Percentage 80.0% 60.0% Number of Charts Reviewed per Month 40.0% Range: 54-82 Mean: 67 20.0% 0.0% Oct 2010 Nov 2010 Dec 2010 Jan 2011 Feb 2011 CCI Data 66.2% 81.7% 83.3% 82.4% 87.5% Goal 100% 100% 100% 100% 100% Month Lessons Learned Lessons Learned/Key Insights Slow and steady wins the race Buy in from staff is essential to success Important to understand the foundation of the concept first The right tool is needed: take the time to find it, don’t be afraid to change it Follow through is required and it needs to be consistent Ongoing compliance monitoring is key to maintaining gains Changes to our event reporting system just prior to implementation may have affected our data We’re still learning! Quick Wins • Champions emerged from Physiotherapy department Data collection became easy with their help • SHN Virtual Learning Series taught the team about: Quality improvement methodology (Can be applied to other projects) Data collection, analysis and trending Viewing the issue from a broader perspective: i.e. pharmacology, special considerations for the elderly, etc. • Great connections made between departments (Nursing, Education, Physiotherapy, Quality) • Great ideas to build on from other teams in the collaborative Next Steps Key Sustainability Steps/Plan: Target Dates Decide on an assessment tool 1 month Implement bathroom signs 1 month Finalize post falls assessment tool and decide if it is going to be used Next 2 months Roll out education to the staff (serve 1 month apple treats to generate recognition) Launch the apple symbol 1 month Contact Information Amy Kantor Amy.Kantor@albertahealthservices.ca 780-989-5954 Judy Poon Judy.Poon@albertahealthservices.ca 780-432-8841