Hip Alignment and Rebalancing Strategies - PHATS

HIP ALIGNMENT AND
REBALANCING STRATEGIES
HIP ALIGNMENT AND RE-BALANCING
STRATEGIES
By: Scott Adams, BHK, MA, ATC, CES
Scott Adams, BHK, MA, ATC, CES
• Educational Background
– University of Windsor - Bachelors of Human
Kinetics (Kinesiology)
– University of Nebraska Omaha - Masters in
Athletic Training
– Corrective Exercise Specialist
– Survival Operating Systems – Level I
Scott Adams, BHK, MA, ATC, CES
• Career Path
• LaSalle Physiotherapy and Rehabilitation Centers
• St. Clair College
• Accelerated Rehabilitation Centers
• Windsor Spitfires Hockey Club (Ontario Hockey
League)
• Johnstown Chiefs (East Coast Hockey League)
• Pittsburgh Penguins (National Hockey League)
HIP ALIGNMENT AND RE-BALANCING
STRATEGIES
• Topics to Review
– Review Hip Anatomy
– Assessment of alignment
– Un-Balancing of the Hips
– Re-Balancing of the Hips
Courtesy of www.stonetemplesanctuary.com
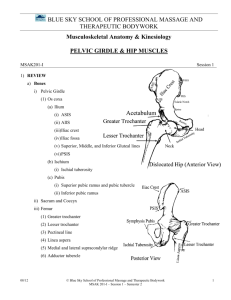
ANATOMY REVIEW
• Hip Joint
– Multi-axial ball and socket synovial joint between the head of the femur and the acetabulum
– Fibrous Capsule – capsule incomplete posteriorly
– Ligaments – illiofemoral, pubofemoral, ischiofemoral
– Intracapsular – ligament of the head of the femur
(very weak)
– Retinacula
ANATOMY REVIEW
Source: www.medicalillustrations.ca
ANATOMY REVIEW
ANATOMY REVIEW
• Prime Movers of Flexion
– TFL
– Pectineus
– Sartorius
– Gracilis
– Illopsoas
Courtesy of ImageRepository.net
ANATOMY REVIEW
• Prime Movers of
Extension
– Gluteus Maximus
– Hamstrings
– Adductor Magnus
(posterior region)
ANATOMY REVIEW
• Prime Movers of
Adduction
– Adductor Longus
– Adductor Brevis
– Adductor Magnus
– Gracilis www.medmeshop.com
ANATOMY REVIEW
• Prime Movers of
Abduction
– Gluteus Medius
– Gluteus Minimus http:// files.myopera.com/san shan/blog/piriformis.gif
ANATOMY REVIEW
• Prime Movers of
Inward Rotation
– Gluteus Minimus
– Tensor Fascia Lata
ANATOMY REVIEW
• Prime Movers of
Outward Rotation
– Gluteus Maximus
– Piriformis
– Obturator Externus
– Obterator Internus
– Superior Gemellus
– Inferior Gemellus
– Quadratus Femoris
– Gluteus Medius www.aroundhawaii.com
ANATOMY REVIEW
• Reference Points for Rotation
– ASIS and PSIS
– We are going to use these two reference points to determine the athletes current resting position
ANATOMY REVIEW
CHRONIC CONTRACTORS
• Muscles that are constantly contracted
• Constant state of fatigue
• May be the primary site of a breakdown leading to chronic injury
UNDERACTIVE MUSCLES
• Muscles that are “lazy”
• They don’t need to work because something is working for them
• Compensation patterns formed
• Leads to chronic injury
CHEST MUSCLES
• Pre and post treatment of releasing the chest muscles
• Note: Hip position http://www.hellerworkstructuralintegration.
com/assets/images/client_photos.jpg
MOVEMENT DIFFERENCES
MOVEMENT DIFFERENCES
MOVEMENT DIFFERENCES
ASSESSING HIP ORIENTATION
• Athlete Supine
• Hips and knees bent
ASSESSING HIP ORIENTATION
• Perform three bridges
ASSESSING HIP ORIENTATION
• Gently return the athlete to a supine position with the legs resting on the table
ASSESSING HIP ORIENTATION
• Landmark the ASIS
– Compare left vs. right
– Note variation in the height of each
ASSESSING HIP ORIENTATION
• Have the athlete move into a prone position
• Landmark the PSIS
– Compare left vs. right
ASSESSING HIP ORIENTATION
• Note leg lengths
• Gives an insight if an up-shift has occurred
• This will not show a true anatomical leg length
ASSESSING HIP ORIENTATION
• RESULTS
– If ASIS and PSIS are even, the hips are in a balanced position
ASSESSING HIP ORIENTATION
• IF ASIS on one side is high, and PSIS on opposite side is high -> we have a rotation of the hips
ASSESSING HIP ORIENTATION
• If the ASIS and PSIS are elevated on the same side -> an up-shift has occurred
ASSESSING HIP ORIENTATION
• If the PSIS or ASIS on the same side are a different distance away from the midline -> an out-flair or in-flair has occurred
CORRECTING HIP ORIENTATION
• Rotation
– Break arm method
• Up-Shift
– Distraction method
• Flairs
– Abduction contraction
CORRECTING HIP ORIENTATION
• Perform corrective strategy
• Have patient remain supine, hips and knees bent as in starting position
• Perform 3 reps of isometric contractions and different angles (adduction and abduction)
• Perform 3 bridges
• Return to original position and re-assess in supine
CORRECTING HIP ORIENTATION
• Focus on lengthening “chronic contractors”
– Massage, myofascial stretching, etc
• Awaken “underactive” muscles
– Isolated muscle strengthening
• Integrate into movements
– Squats, lunges, rotational movements
• Integrate into sport-specific movements
CORRECTING HIP ORIENTATION
• REMEMBER
– The role fascia plays on chronic muscles -
> the hip flexor may not be the true source of dysfunction
-> look up and down the movement chain
THANK YOU