CONFERENCE ON “ FOOD ADDITIVES : SAFETY IN USE AND CONSUMER CONCERNS“
JOMO KENYATTA UNIVERSITY OF AGRICULTURE AND TECHNOLOGY
NAIROBI , 24 JUNE 2014
HAZARD
is the potencial capacity of producing harm.
is proportional to both the
and the
.
RISK ANALYSIS
•
Food additives are highly regulated at global level. (i.e. EFSA, FAs etc. etc.)
•
No food additive can be used without safety assessment and approval
•
Safety assessment is undertaken PRIOR to approval
•
The applicant (industry) provides the safety data, which have to be performed to
defined quality standards (GLP, QA, OECD, UE guidelines……)
•
The assessment Panels – which include scientists and regulators with a wide range of
expertise – are responsible for safety assessments
Hazard identification
Inherent biological activity
Hazard assessment
Assessment of relevance for humans
Dose-response analysis
EXPOSURE ASSESSMENT
Active principle
Dose of food additives
Dose in individuals
Dose in special population groups
Max/min chronically/occasionally
HAZARD IDENTIFICATION
Identification of adverse health effects
In silico methodologies
In vitro toxicology data
Animal-based toxicological studies
Human observation
HAZARD ASSESSMENT
Quantification of adverse health effects
Kinetic variability
Dynamic variability
Mode/mechanism of action
Selection of critical data
Dose-response for critical effect
RISK CHARACTERISATION
Principle 1
Risk management should follow a structured approach
Principle 2
Protection of human health should be the primary consideration in risk management decisions
Principle 3
Risk management decisions and practices should be transparent
Principle 4
Determination of risk assessment policy should be included as a specific component of risk management
Principle 5
Risk management should ensure the scientific integrity of the risk assessment process by maintaining
the functional separation or risk assessment and risk management
Principle 6
Risk management decisions should include clear, interactive communication with consumers and other
interested parties in all aspects of the process
Principle 7
Risk management should be a continuing process that takes into account all newly generated data in the
evaluation and review of risk management decisions
Reference points (RPs) in toxicology studies used to calculate
a safe level for human intake:
Benchmark Dose (BMD).
Toxicant and/or NON Genotoxic Carcinogen
Toxicants
Dietary supplements
Botanicals – Herbs
Contaminants
•
ADI
(Acceptable Daily Intake)
•
ARfD
(Acute Reference Dose)
•
TMDI
(Tolerable Maximum daily Intake)
•
XYZ
……………………………………………………… etc. etc
ADI represents the
amount of a food
additive, a pesticide
or a veterinary drug
residue, expressed on
a body weight basis,
that can be ingested
daily over a lifetime
without appreciable
health risk.
ARfD
represents the
amount of a pesticide,
expressed on a body
weight basis, that can
be ingested over a
short period of time
(one day) without
appreciable health risk
T(M)DI
represents
permissible human
daily exposure to those
contaminants,
expressed on a body
weight basis,
unavoidably associated
with the consumption
of nutritious foods.
ALLOCATION
ADI – ARfD -TMDI– xxz…..
TOXICOLOGICAL PROTOCOL
Absorption
LD50 oral
Mutagenesis
Distribution
LD50 dermal
Clastogenesis
Metabolism
LC50 inhalation
Aneuploidy
Excretion
Skin irritation
Eye irritation
Skin sensitization
Teratogenicity tests (Rat-Rabbit)
Two generation reproductive toxicity
Mouse
90 day toxicity
Rat
90 day toxicity
Dog
90 day toxicity
Dog
1 year toxicity
Mouse 18 months
Rat 104 weeks
• The greatest concentration or amount of an agent, found by
study or observation that causes detectable, usually adverse
(or toxic?) alteration of morphology, functional capacity,
growth, development or lifespan of the target
HUMANS
sensitive subjects
HUMANS
population average
ARfD
AOEL
1
10
dose mg/kg bw
100
ADI =
NOAEL
SF
ADI = Admissible Daily Intake mg/kg b.w.
NOAEL = No Observed Adverse Effect Level (mg/kg b.w.)
SF = Safety Factor (10, 100, n)
Differences
10
Interindividual Differences
10
Interspecies
-∞
Log Concentration
+∞
Exposure assessment is
a key element of risk assessment and
a tool for risk management
It’s theoretically simple but practically complex due to data deficiencies
Examples of exposure models: ILSI Europe’s ‘ GUIDEA ‘ and FACET
•
Which substances are present in what amounts in a given food/diet:
including information concerning factors influencing their levels and qualities such as
bioavailability
•
How much of the foods containing these substances are consumed
and what is the consumption of potentially relevant risk groups, including high users?
•
What are the conditions and the probabilities of consuming occasionally or regularly
high amounts of such foods which at the same time contain high levels of the substance(s) in
question?
:
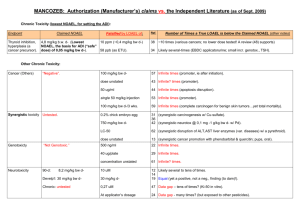
Regulated Maximum Levels (MLs) in the EU for: mycotoxins (aflatoxins, ochratoxin A, patulin,
deoxynivalenol, zearalenone, fumonisins, T2 and HT-2-toxin) metals (cadmium, lead, mercury and inorganic
tin) dioxins and dioxin-like PCBs, 3-MCPD, polycyclic aromatic hydrocarbons (benz(o)pyrene).
Manufacturer’s Use Levels
Total Diet Survey ( TDS ) determines levels of various contaminants and nutrients in foods.
Duplicate Diets Test persons consume their ordinary diet, but for subsequent analysis, they also prepare
a duplicate portion of all food products as prepared, served and consumed.
Individual Food Diary Records interviews.
Household Budget Surveys ( HBS ) national surveys mainly focusing on consumption expenditure.
• Methodologies to integrate food consumption, fate and
chemical concentration to make the best estimate of exposure.
Concentration
of chemical in
diet
Weight of
diet consumed
daily
Body weight
(60 kg )
Exposure = mg/kg body weight/day
Sampling and Analysis
Temporal- extrapolation to lifetime exposure
Under/Over reporting
Representativeness of population sample
Other sources of exposure eg. supplements , medicines
Coding system not specific enough
Portion size
Processed food
Consumer Loyalty
Quantity of
food
consumed
Distribution of
concentrations
Usage level of
the Additive
in food
Presence
probability
Occurrence of
the Additive
in food
INTAKE
Specific
Codification
System
ILSI EUROPE
http://www.ilsi-guidea.org/index.php?title=Main_Page
PERCEIVED RISKS (media)
REAL RISK (WHO)
Nutritional Deficiencies
Food Additives
Bacterial Intoxications
Nutritional Deficiencies
Biological Toxins
Bacterial Intoxications
Biological Toxins
Food Additives
ABSORPTION
GENOTOXICITY
In vitro testing
TOXICITY (28-day/90-day study)
TRIGGERS FOR CONSIDERING TIER 2
Toxicity in the 28/90-day study
Guidance for submission for food additive evaluations EFSA Panel on Food
Additives and Nutrient Sources added to Food (ANS) - EFSA Journal 2012;10(7):2760
Systemic availability
Genotoxicity in vitro
ADME
Single dose
GENOTOXICITY
In vivo testing
TOXICITY (stand alone or combined)
Chronic toxicity
Carcinogenicity
REPRODUCTIVE & DEVELOPMENTAL TOXICITY
Extended One–Generation Reproduction Toxicity Study
PRENATAL DEVELOPMENTAL TOXICITY (Teratogenicity)
TRIGGERS FOR CONSIDERING TIER 3
Bioaccumulation
Positive in vivo genotoxicity
Chronic toxicity/Carcinogenicity
Reproductive & developmental toxicity
Guidance for submission for food additive evaluations EFSA Panel on Food
Additives and Nutrient Sources added to Food (ANS) - EFSA Journal 2012;10(7):2760
ADME
Repeated doses
CARCINOGENICITY
Mode of action
REPRODUCTIVE & DEVELOPMENTAL TOXICITY
Endocrine Disruptor?
SPECIALIZED STUDIE
Immunotoxicity
Neurotoxicity
Endocrine activity
Mode of Action
Guidance for submission for food additive evaluations EFSA Panel on Food
Additives and Nutrient Sources added to Food (ANS) - EFSA Journal 2012;10(7):2760
 0
0