Patient Flow Management System
at
Parker Adventist Hospital
Jason Makaroff – Director of Process Improvement
Jennette Bergstrom – Director of Acute Care Services
Brandon Robertson – Administrative Resident
Contents
•
•
•
•
Introduction
Patient Flow Committee
Current State/Symptoms/Approach
Solution: Patient Flow System
– Structured Framework
– Forecasting: Data Driven Decision Making
– Daily Operations
– Next Steps: Adding Granularity
Patient Flow Committee: Mission
Mission
To design a process that promotes the flow of patients
through the organization such that a patient’s hospital
experience feels safe, timely, efficient and proceeds
with minimal delays with bed utilization optimized.
Patient Flow Committee: Objectives
1. Optimize utilization of existing patient beds (capacity) and associates
caring for patients while providing the safest possible care.
2. Avoid diversions/transfers for patient safety, patient, physician and
associate satisfaction and to promote organizational growth & viability.
3. Ensure compliance with regulatory guidelines and requirements for
patient flow.
4. Establish (data/reports) infrastructure for real-time monitoring of
organization capacity and demand for utilization by all appropriate
managers that will provide guidance for optimal staffing.
5. Develop and establish methods e.g. guidelines/protocols/algorithms
and mechanisms to facilitate appropriate patient flow.
6. Facilitate collaboration within the facility for PI projects, monitoring,
and opportunities for improvement.
7. Celebrate Success!
Current State
• Frequent Bed Shortages in Acute Care Services
• Highly Stressful, Reactive Environment
• No Defined Processes for Managing Capacity vs. Demand
• No Ability to Plan Ahead
• Delays in Discharges on the Floor Due to Uncoordinated
Resources
Symptoms
• Long delays in the Emergency Department
• Excessive PACU Hold Times
• No beds available for patients coming out of surgery
• Average TAT for discharges is greater than 3 hours
• Discharge orders being written late morning/early afternoon
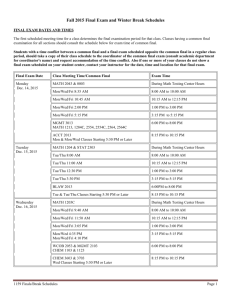
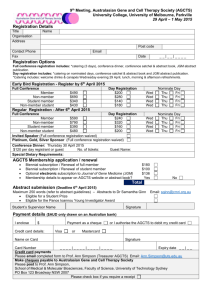
Understanding the Patient Flow Patterns
Admits: 1st Flr vs. 2nd Flr
Emergency department
admissions influenced by natural
variation.
11
10
Quantity of Admits
Surgery Schedule influenced by
artificial variation.
9
8
Admits 1st Floor
7
Admits 2nd Floor
6
Admits 2nd Floor Goal
5
4
3
Monday
Tuesday
Wednesday
Thursday
Friday
Weekday
Data indicates potential for
bottlenecks to occur on Mondays
and Tuesdays.
Discharges: 1st Flr vs. 2nd Flr
Quantity of Discharges
10
9
8
DCs 1st Floor
7
DCs 2nd Floor
6
DCs 2nd Floor Goal
5
4
3
Monday
Tuesday
Wednesday
Weekday
Thursday
Friday
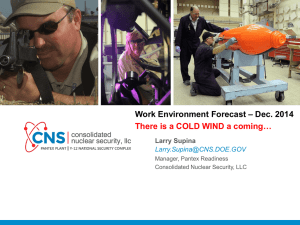
Understanding the Patient Flow Patterns
Inpatient Elective Surgery Schedule Fluctuations
3/15/2010 - 4/27/2010
14
12
Number of Cases
12
10
10
8
10
9
10
9 9
9
8
8
7
6
6
6
5
4
5
4
5
5
4
4 4
3
2
2 2
4
3
3
2
1
1
Mon
Tue
Wed
Thu
Fri
Mon
Tue
Wed
Thu
Fri
Mon
Tue
Wed
Thu
Fri
Mon
Tue
Wed
Thu
Fri
Mon
Tue
Wed
Thu
Fri
Mon
Tue
Wed
Thu
Fri
Mon
Tue
0
12
11
Day of Week
Highly variable elective surgery schedule makes it difficult to plan resources
effectively and the hospital environment becomes more reactive than proactive.
Approach
•
Develop & implement a plan for managing
demand and capacity real-time.
•
Move the organization from being reactive
to pro-actively responding to peaks in
demand with regards to patient flow.
Patient Flow System
Managing Demand and Capacity Real-time.
1.
Define facility-wide definitions for capacity and demand.
•
•
Capacity Levels defined for Green, Yellow, and Red
Efficient Capacity defined as 85% or less of maximum beds
available
Green: 85% of Efficient Capacity or Less
Yellow: Between 85 and 95% of Efficient Capacity
Red: Greater than 95% of Efficient Capacity
•
•
•
2.
•
Working with clinical and ancillary support departments,
define operational policies for each department that are
dependent on the current level of demand vs. capacity.
Defined policies and procedures for operating in green, yellow, and
red capacity status levels.
•
Department specific operational functions for each capacity level
•
Defined standardized procedures for Administrative Managers and
staff to conduct bed meetings.
•
Provide structured mechanisms for standardizing report out in bed
meetings.
•
Provide focal point for Admin Managers to direct resources in
relation to capacity and demand levels.
3.
1.
2.
3.
4.
Define policies for Discharge Lounge and Overflow Areas
for use during Yellow and Red Capacity Status events.
Define policies for discharge lounge and overflow activation.
Designate physical location and staffing for discharge lounge.
Train Admin Managers on implementation of discharge lounge and
overflow areas.
Educate staff on discharge lounge usage and overflow area procedures.
4.
1.
2.
3.
Define hospital-wide communication plan for Capacity
Status
Admin managers determine hospital’s capacity status based on current
surgical schedule and planned discharges coupled with 90 days of
historical data on patient volume.
PBX operator is notified by Admin Manager to send house-wide
communication of capacity status via pager and VOIP phones.
Unit Secretaries and department leaders update capacity signage on each
unit to reflect current state of capacity status house-wide.
5.
1.
2.
3.
4.
5.
6.
Create marketing and training materials to promote
cultural change and hardwire the process into the
organization.
Health stream module developed to train all organization leaders on the
concepts of the Patient Flow System.
Logo for Patient Flow System designed and used on all materials related
to patient flow for associate recognition and acceptance.
Discussion on Patient Flow System integrated into Employee forums
through flyers mailed to associates residences and presentation in forum.
Rounding logs created for hard-wiring the process into the organization.
Rounding conducted on leaders.
Rounding to be scheduled for associates.
Patient Flow System: Forecasting
1.
Develop tools for predicting current day forecast for admissions and
discharges.
2.
Integrate forecasts into day to day operations.
Patient Flow System: Forecasting
• Predictive ability: >75%
• Uses data sources from MEDITECH
and utilized by Admin Managers
• Has the ability to forecast the current
day’s capacity status color thereby
initiating multiple house-wide
processes
Lessons Learned
Lessons Learned
•
•
•
•
•
•
•
•
•
Adding a night-time bed meeting at 2230 hours is effective for
preparing for next day discharges.
Acute Care Services director position overseeing all areas of acute
care has helped to promote best practices in each area (ICU,
Gen/Surg, Med/Tele).
Spread strategy for implementing Patient Flow System is effective.
Discharge Lounge helps reduce the number of delayed discharges.
Strong executive sponsorship is required to be successful.
Data is available, but obtaining it in a usable format is challenging.
Patient safety has increased.
Opportunities exist for creating tools that allow forecasting for staffing
Challenges hospitalists to work harder and more efficiently.
Patient Flow System: Next Steps
•
•
•
Add more standardization around bed meeting report outs
Next version of Patient Flow System will increase granularity and
manage capacity on a department level.
Future plan of Patient Flow System is to automate forecasting by
pulling data from the enterprise database and building a forecasting
tool for My Virtual Workplace.
•
•
•
•
•
Develop tools for predicting one week forecasts based on historical data pulled from
Centura’s data repositories.
Integrate forecasts into day to day operations to provide operational direction for ancillary
departments based on anticipated volume.
Provides a foundation for building staffing models based on historical data.
Update policies with suggestions for increasing process efficiencies in
ancillary and clinical departments during each capacity level.
Patient Flow Dashboard with graphics that track metrics on Patient
Flow in each department. (draft example)
“Well done is better than well said.”
-Benjamin Franklin
 0
0