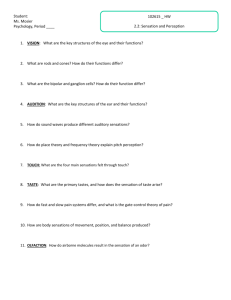
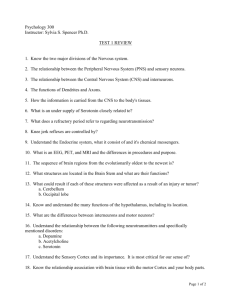
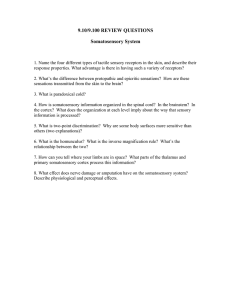
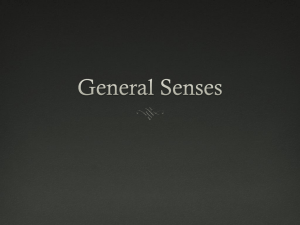
CM100: PHYSIOLOGY SENSORY RECEPTORS & SOMATIC SENSATIONS ROGELIO JUNIOR B. RIVERA, MD | SEPTEMBER 6, 2023 TABLE OF CONTENTS I. SENSORY RECEPTORS 1 A. TYPES OF SENSORY RECEPTORS AND STIMULI 1 B. TRANSDUCTION OF SENSORY STIMULI 1 C. PHYSIOLOGICAL CLASSIFICATION OF NERVE FIBERS 3 II. SPATIAL AND TEMPORAL SUMMATIONS 4 A. SPATIAL SUMMATIONS 4 B. TEMPORAL SUMMATIONS 4 III. NEURONAL POOLS AND CIRCUITS 4 A. RELAYING OF SIGNALS THROUGH NEURONAL POOLS 4 B. NEURONAL CIRCUIT WITH BOTH EXCITATORY 5 AND INHIBITORY SIGNALS 5 III. SOMATIC SENSES A. CLASSIFICATION OF SOMATIC SENSES 6 6 B. DETECTION AND TRANSMISSION OF TACTILE SENSES 6 C. PROPRIOCEPTION OF SKELETAL MUSCLES 7 IV. SENSORY PATHWAYS FOR SOMATIC SIGNALS IN CNS 7 ● Each nerve tract terminates at a specific point in the central nervous system ● Type of sensation felt is determined by the point in the nervous system to which the fiber leads B. TRANSDUCTION OF SENSORY STIMULI ● Receptor potential → Change in membrane electrical potential resulting from type of stimulus that excites the receptor → Common among all sensory receptors Receptor Potentials ● Receptor potential → Change in membrane potential and permeability of the receptors → Mechanisms: ▪ Mechanical deformation − Stretches receptor membrane − Opens ion channels ▪ Application of a chemical − Opens ion channels ▪ Change of the temperature − Alters membrane permeability ▪ Effects of electromagnetic radiation − Directly or indirectly changes receptor membrane characteristics to allow ions to flow through channels Table 1. Mechanisms of Receptor Potentials in the Membrane A. ANATOMICAL ORGANIZATION 7 B. SENSORY PATHWAYS 7 Mechanism C. DORSAL COLUMN-MEDIAL LEMNISCATE SYSTEM 7 Mechanical deformation D. ANTEROLATERAL PATHWAY 8 ● Stretches receptor membrane ● Opens ion channels E. THALAMIC AND CORTICAL SOMATOSENSORY AREAS 8 Application of a chemical ● Opens ion channels F. SOMATOSENSORY CORTEX Change in temperature ● Alters membrane permeability 8 V. TEMPERATURE SENSATION 9 V. PAIN SENSATION 9 A. NOCICEPTORS 9 B. POSITIVE MODULATION OF PAIN SENSATIONS 9 C. CENTRAL PAIN PATHWAYS 10 VI. REFERENCES 10 I. SENSORY RECEPTORS A. TYPES OF SENSORY RECEPTORS AND STIMULI ● Mechanoreceptors → Detect mechanical compression or stretching ● Thermoreceptors → Detect changes in temperature ● Nociceptors → A.k.a. pain receptors → Detect physical or chemical damage ● Electromagnetic receptors → A.k.a. photoreceptors → Detect light on the retina of the eye ● Chemoreceptors → Detect taste, smell, oxygen level, osmolality of body fluids, and other factors that make up the chemistry of the body Effects radiation of Effect electromagnetic ● In/directly changes receptor membrane characteristics to allow flow of ions through channels LECTURER NOTES ● All these [mechanisms] change the membrane permeability, allowing ions to diffuse and change transmembrane potentials ● Maximum Receptor Potential Amplitude → . The maximum amplitude of most sensory receptor potentials is about 100 mV ▪ Only occurs at extremely high intensity of sensory stimulus ● Receptor Potential and Action Potential Relationship → When the receptor potential rises above a threshold level, action potentials are produced → The more the receptor potential rises above the threshold level, the greater becomes the action potential frequency Differential Sensitivity of Receptors ● Differential sensitivities → Each type of receptor is highly sensitive to one type of stimulus yet almost non-responsive to another The Labeled Line Principle ● Receptors only transmit one modality of sensation → Specificity of nerve fibers → Principal types of sensation experienced → Pain, touch, sight, sound, etc ● Nerve fibers only transmits impulses Trans # 3 Figure 1. Relation between receptor potential and action potentials when the receptor potential rises above threshold level A5: Apuya, Baldo, Bata, Batua, Bufete, Calicdan, Ced, Co, Eborde, Espinas, Galay, Hamor TH: Abalon 1 of 15 Figure 2. Excitation of a Sensory Nerve Fiber by a Receptor Potential Produced in a Pacinian Corpuscle Figure 2 ● From the left-hand side of the figure → Small area of terminal fiber is deformed by compression of the corpuscle → Ion channels open in the membrane; allows sodium ion diffusion towards fiber interior → Sodium ion diffusion causes increased positivity inside fiber called receptor potential ▪ Induces a local circuit of current flow that spreads along the nerve fiber ● First node of Ranvier → Lies inside Pacinian corpuscle capsule → Location of fiber membrane depolarization by local current flow → Typical action potentials are then transmitted along the nerve fiber towards the central nervous system ● Relation Between Stimulus Intensity and the Receptor Potential → Frequency of repetitive action potentials increases approximately in proportion to the increase in receptor potential ▪ ↑ action potential frequency, ↑ receptor potential → Very intense receptor stimulation → Less additional increase in action potential (Refer to Figure 3) Figure 3. Relation of Amplitude of Receptor Potential to Strength of a Mechanical Stimulus Applied to a Pacinian Corpuscle Adaptations of Receptors ● Adapt either partially or completely to any constant stimulus after a period of time ● Continuous sensory stimulus → Receptor responds at a high impulse rate → Respond at a progressively slower rate → Rate of action potentials decreases to very few or to none at all Figure 4. Adaptation of Different Types of Receptors Figure 4 ● Pacinian corpuscle adapts very rapidly ● Hair receptors adapt within a second or so ● Some joint capsule and muscle spindle receptors adapt slowly ● Some sensory receptors adapt to a far greater extent than others → Pacinian corpuscles adapt to “extinction” within a few hundredths of a second → Receptors at the bases of the hairs adapt to extinction within a second or more → Most mechanoreceptors eventually adapt almost completely ● Nonadapting receptors → Mechanoreceptors that require some hours or days to adapt to a stimulus → The longest measured time for almost complete adaptation of a mechanoreceptor is about 2 days ▪ Carotid and aortic baroreceptors ▪ Specialized baroreceptors may never fully adapt → Chemoreceptors and pain receptors probably never adapt completely Adaptive Mechanisms of Receptors ● Different for each type of receptor → Similar to how development of a receptor potential is an individual property → E.g. in the eye: rods and cones adapt by changing the concentrations of their light-sensitive chemicals → Pacinian corpuscle ▪ Mechanoreceptor that has been studied in great detail ● Adaptation can occur in two ways: → Resulting from readjustments in the structure of the receptor ▪ Due to the viscoelastic structure of the Pacinian corpuscle − When a distorting force is applied to one side of the corpuscle, this force is directly transmitted to the same side of the central nerve fiber, thus eliciting a receptor potential − Receptor potential appears at the onset of compression but disappears within a small fraction of a second, even though the compression continues o Fluid within the corpuscle redistributes → Receptor potential is no longer elicited → Resulting from an electrical type of accommodation in the terminal nerve fibril ▪ Accommodation − Much slower mechanism of adaptation of the corpuscle − Occurs in the nerve fiber itself − Central core fiber continues to be distorted → Tip of nerve fiber gradually becomes accommodated to stimulus o Continued stimulation will result in progressive inactivation of the sodium channels = Sodium current flow through the channels causes them to close gradually - seen in all or most cell membrane sodium channels Receptors According to Adaptability ● Tonic Receptors → Slowly adapting receptors → Continue to transmit impulses to the brain as long as the stimulus is present (minutes, hours, even days; hence “tonic”) CM 100 Sensory Receptors and Somatic Sensations 2 of 15 → Keep the brain constantly apprised of the status of the body and its relation to its surroundings ▪ E.g. impulses from the muscle spindles and Golgi tendon apparatuses allow the nervous system to know the status of muscle contraction and load on the muscle tendon at each instant → Other slowly adapting receptors include the following: ▪ Receptors of the macula in the vestibular apparatus ▪ Pain receptors ▪ Baroreceptors of the arterial tree ▪ Chemoreceptors of the carotid and aortic bodies ● Rate, Movement, and Phasic Receptors → Rapidly adapting to stimulus → Cannot be used to transmit a continuous signal because they are stimulated only when the stimulus strength changes → React strongly while a change is taking place → E.g. Pacinian corpuscle ▪ Sudden pressure applied to the tissue excites this receptor for a few milliseconds, and then its excitation is over − However, the pressure continues ▪ Signal is transmitted again later when pressure is released ▪ Exceedingly important in apprising the nervous system of rapid tissue deformations ▪ Useless for transmitting information about constant conditions in the body Table 2. Comparison of Tonic and Phasic Receptors Rate of adaptation Information transmitted Tonic Receptors Phasic Receptors Slowly adapting Rapidly adapting Constant status of the body Rapid tissue deformations Predictive Function of the Rate Receptors ● If the rate at which some change in the body’s status is taking place is known, the state of the body a few seconds or even a few minutes later can be predicted ● E.g. receptors of the semicircular canals in the vestibular apparatus → Detect the rate at which the head begins to turn when a person runs around a curve ▪ A person can predict how much he or she will turn within the next 2 seconds ▪ Able to adjust the motion of the legs ahead of time to keep from losing balance ● E.g. receptors located in or near the joints → Help detect the rates of movement of the different parts of the body → When running: ▪ Information from the joint rate receptors → Nervous system predicts where the feet will be during any precise fraction of the next second ▪ Appropriate motor signals can be transmitted to the muscles of the legs to make any necessary anticipatory corrections in position so the person will not fall ▪ Loss of this predictive function → Impossible for person to run C. PHYSIOLOGICAL CLASSIFICATION OF NERVE FIBERS ● Some signals need to be transmitted to or from the central nervous system extremely rapidly; otherwise, the information would be useless ● Some types of sensory information do not need to be transmitted rapidly → E.g. prolonged aching pain → Slowly conducting fibers suffice CM 100 Sensory Receptors and Somatic Sensations Figure 5. General sensory nerve classification Figure 2 ● Sizes, velocities of conduction, and functions of the different nerve fiber types are given → Range from 0.5 to 20 micrometers in diameter → The larger the diameter, the greater the conducting velocity → The range of conducting velocities between 0.5 and 120 m/sec General Classification of Nerve Fibers ● Type A fibers → Further subdivided into α, β,γ, and δ fibers → Typical large and medium-sized myelinated fibers of spinal nerves ● Type C fibers → Small unmyelinated nerve fibers → Conduct impulses at low velocities → Constitute more than half of the sensory fibers in most peripheral nerves and all postganglionic autonomic fibers Alternative Classification Used by Sensory Physiologists ● Group Ia → Fibers from the annulospiral endings of muscle spindles → ≈17 microns in diameter on average → α-type A fibers ● Group Ib → Fibers from the Golgi tendon organs → ≈16 micrometers in diameter on average → α-type A fibers ● Group II → Fibers from most discrete cutaneous tactile receptors and from the flower-spray endings of the muscle spindles → ≈8 micrometers in diameter on average → β-and γ-type A fibers ● Group III → Fibers carrying temperature, crude touch, and pricking pain sensations → ≈3 micrometers in diameter on average → δ-type A fibers ● Group IV → Unmyelinated fibers carrying pain, itch, temperature, and crude touch sensations → 0.5–2 micrometers in diameter → Type C fibers 3 of 15 Table 3. Summary of Alternative Classification of Nerve Fibers Type of Fiber Function/Origin Average Diameter General Classification Group Ia Annulospiral endings of muscle spindles ~17 microns α-type A fibers Group Ib Golgi tendon organs ~16 microns Group II Most discrete ~ 8 micrometers β-and γ-type A cutaneous tactile fibers receptors; flower-spray endings of muscle spindles Group III Carry temperature, crude touch, and pricking pain sensations Group IV Unmyelinated fibers carrying pain, itch, temperature, and crude touch sensations B. TEMPORAL SUMMATIONS ● Increased transmission of signals by increasing the frequency of nerve impulses in each fiber ~ 3 micrometers δ-type A fibers 0.5 to 2 micrometers Type C fibers II. SPATIAL AND TEMPORAL SUMMATIONS ● Signal intensity must always be conveyed ● The different gradations of intensity can be transmitted either by → Spatial summation ▪ Using increasing numbers of parallel fibers → Temporal summation ▪ Sending more action potentials along a single fiber A. SPATIAL SUMMATIONS ● Increasing signal strength is transmitted by using progressively greater numbers of fibers Figure 7. Example of a Temporal Summation Figure 7 ● A changing number of impulses (along the x-axis) translates to an increase in strength of signal (along the y-axis) III. NEURONAL POOLS AND CIRCUITS ● Thousands to millions in the central nervous system → Some of these pools contain few neurons, whereas others have vast numbers → Entire cerebral cortex: could be considered as a single, large neuronal pool → Other neuronal pools: basal ganglia, specific nuclei (thalamus, cerebellum, mesencephalon, pons, and medulla) → The spinal cord’s dorsal gray matter: one long pool of neurons ● Each neuronal pool has its own special organization that causes it to process signals in its own unique way → Allows the total consortium of pools to achieve the multitude of functions of the nervous system ● The pools also have many similar principles of function A. RELAYING OF SIGNALS THROUGH NEURONAL POOLS Neuron Organization for Relaying Signals ● Input fibers → Divide hundreds to thousands of times, providing a thousand or more terminal fibrils → Fibrils spread into a large area in the pool where they synapse with dendrites or cell bodies → Dendrites usually arborize and spread hundreds to thousands of micrometers in the pool ● Stimulatory field → The neuronal area stimulated by incoming nerve fiber → Many terminals from each input fiber lie on the nearest neuron in its “field” → Progressively fewer terminals lie on the neurons farther away Figure 6. Spatial Summation Pattern of Stimulation Figure 6 ● Skin innervated by parallel pain fibers ● Parallel pain fibers arborize into free nerve endings → The entire cluster of fibers from one pain fiber frequently covers the receptor field of the fiber ▪ An area of skin as large as 5cm in diameter → Arborizing fibrils overlap those from other pain fibers ● A pinprick of the skin usually stimulates endings from many different pain fibers simultaneously → When the pinprick is in the center of the receptive field of a particular pain fiber, the degree of stimulation of that fiber is far greater than when it is in the periphery of the field ▪ Number of free nerve endings concentrated in the middle ▪ Number diminishes toward the periphery ● Lower portion of Figure 3: → Three views of the cross section of the nerve bundle → Weak stimulus: single nerve fiber (denoted by the red fiber) and weak stimulation of adjacent fibers → Moderate and strong stimuli: progressively more fibers stimulated ● Stronger signals spread to more fibers = spatial summation CM 100 Sensory Receptors and Somatic Sensations Threshold and Subthreshold Stimuli ● Excitation or facilitation ● Single excitatory presynaptic terminal = no action potential in a postsynaptic neuron ● Large number of input terminals (neurons 1 and 2 in Figure 8) must discharge on the same neuron either simultaneously or in rapid succession to elicit action potential or excitation → Excitatory stimulus ▪ Enough terminals to cause a neuron to discharge ▪ “Suprathreshold stimulus” − Above the threshold required for excitation → Subthreshold stimulus ▪ Not enough terminals to cause excitation ▪ Neurons are facilitated − Neurons that are more likely to be excited by signals arriving through other incoming nerve fibers ● Refer to Figure 8 for the Basic Organization of a Neuronal Pool 4 of 15 Figure 10. Divergence in Neuronal Pathways Figure 8. Basic Organization of a Neuronal Pool Figure 8 ● Input fibers - left ● “Output” fibers (dendrites and neuronal bodies) - right ● Input fiber 1 has enough terminals to cause neuron a to discharge → Excitatory stimulus to neuron a ● Input fiber 1 also contributes to neurons b and c, but not enough to cause excitation → Subthreshold stimulus to neurons b and c; neurons are facilitated Figure 9. “Discharge” and “Facilitated” Zones of the Neuronal Pool Figure 9 ● Discharge Zone → “Excited zone” or “liminal zone” → Central portion of the field → Region where all neurons are stimulated by the incoming fiber ● Facilitated Zone → “Subthreshold zone” or “subliminal zone” → Lies on each side of the discharge zone → Where neurons are facilitated but not excited ● Inhibition of Neuronal Pool → Some input fibers inhibit neurons → Entire field of becomes the inhibitory zone → Large number of endings in center → Great degree of inhibition ▪ Progressively less inhibition towards the edges Divergence of Signals Passing Through Neuronal Pools ● A phenomenon where weak signals enter a neuronal pool to excite far greater numbers of nerve fibers leaving the pool ● Two major types: → Amplifying type of divergence ▪ An input signal spreads to an increasing number of neurons as it passes through successive orders of neurons in its path ▪ Exhibited by corticospinal pathway (control of skeletal muscles) − A single large pyramidal cell in the motor cortex can excite 10,000 muscle fibers (under highly facilitated conditions) → Divergence into multiple tracts ▪ Signal is transmitted into two directions from the pool ▪ E.g. information transmitted up the dorsal columns of spinal cord can be transmitted into: − The cerebellum; and − Through the lower regions of the brain (thalamus and cerebral cortex) ▪ Almost all sensory information relayed to deeper structures of thalamus and discrete regions of the cerebral cortex CM 100 Sensory Receptors and Somatic Sensations Convergence of Signals ● Convergence denotes signals that unite to excite a single neuron ● Single-source convergence → Multiple terminals from a single incoming fiber tract terminating on the same neuron → An action potential from a single input terminal does not cause excitation of the accompanying neurons → Action potentials from multiple terminals provide enough spatial summation to bring the neuron to the threshold required for discharge ● Multiple-source convergence → Excitatory or inhibitory signals coming from multiple sources → Interneurons in the spinal cord receive signals from the: ▪ Peripheral nerve fibers entering the cord ▪ Propriospinal fibers passing from one segment of the cord to another ▪ Corticospinal fibers from the cerebral cortex ▪ Other long pathways descending from the brain into the spinal cord → Signals received by the spinal cord interneurons then converge on anterior motor neurons to control muscle function → Summation of information is achieved through the summated effect of varying information types Figure 11. Convergence of Multiple Input Fibers onto a Single Neuron B. NEURONAL CIRCUIT WITH BOTH EXCITATORY AND INHIBITORY SIGNALS ● Incoming signals can elicit both excitatory signal in one direction and an inhibitory signal in another ● Reciprocal inhibition circuit → Occurs in control of antagonistic pairs of muscles, so that the desired action of a muscle group/s will not be opposed → E.g. excitatory signal moves leg muscles forward, and an inhibitory signal inhibits muscles on the back of the legs to prevent opposing action → This type of circuit is important in preventing overactivity in many parts of the brain 5 of 15 Figure 12. Inhibitory Circuit Figure 12 ● The input fiber directly excites the excitatory pathway, but also stimulates an intermediate inhibitory neuron (neuron 2) ● Neuron 2 secretes a different type of transmitter to inhibit the second output pathway from the pool III. SOMATIC SENSES ● Somatic senses → Nervous mechanism that collect sensory information from all over the body ● Special senses → Vision, hearing, smell, taste, and equilibrium A. CLASSIFICATION OF SOMATIC SENSES ● Mechanoreceptive → Tactile senses ▪ Touch, pressure, vibration, and tickle senses → Position senses ▪ Static position and rate movement senses → Stimulated by mechanical displacement of some tissue of the body ● Thermoreceptive senses → Detect heat and cold ● Pain sense → Activated by factors that damage the tissue ● Other Classification of Somatic Sensations → Exteroreceptive sensations ▪ From the surface of the body → Proprioceptive sensations ▪ Relating to the physical state of the body ▪ Position sensations, tendon and muscle sensations, pressure sensations from the bottom of the feet, and sensation of equilibrium (special sensation rather than somatic) → Visceral sensations ▪ Viscera of the body ▪ Sensations from internal organs → Deep sensations ▪ From deep tissues ▪ Fasciae, muscles, and bone ▪ “Deep” pressure, pain, and vibration B. DETECTION AND TRANSMISSION OF TACTILE SENSES ● Touch, pressure, and vibration are classified as three separate sensations but are detected by the same types of receptors → Touch sensation - stimulation of tactile receptors in the skin or in tissues immediately beneath the skin → Pressure sensation - deformation of deeper tissues → Vibration sensations - rapidly repetitive sensory signals Classification of Low Threshold Mechanoreceptors ● According to adaptation of receptors → FA (fast adapting) afferents → SA (slow adapting) afferents ● According to their receptive fields → Type I ▪ Small receptive fields with well defined borders ▪ Usually found in non-hairy (glabrous) skin → Type II ▪ Wider receptive fields with poorly defined borders Receptors in Glabrous Skin ● Meissner’s corpuscle (MC) → Great sensitivity → Elongated encapsulated nerve ending of large (type Aβ) myelinated sensory nerve fiber ▪ Many branching terminal nerve filaments inside capsule → Detects light touch → Present in non-hairy parts of the skin ▪ Areas of the skin where highly developed discernment of spatial locations of touch sensations ▪ E.g. fingertips, lips, soles → Adapt in a fraction of a second after they are stimulated ▪ Particularly sensitive to movement of objects over the surface of the skin and low-frequency vibration → Can be tested clinically using the two-point discrimination ● Expanded tip tactile receptors (ETTR) → Found in fingertips and other areas with large numbers of Meissner’s corpuscle → Merkel’s discs ▪ Grouped together in a receptor organ called touch domes − Extremely sensitive receptor − Tonic receptors for sustained light touch; detects texture − Project upward against the underside of skin epithelium ▪ Innervated by a single large myelinated nerve fiber (type Aβ) → In hairy parts of the skin, ETTR vs MC ▪ Contain moderate amounts of ETTR but almost no MC ▪ ETTR transmit initially strong but partially adapting signal → Continuing weaker signal that adapts slowly ▪ ETTR gives out steady-state signals to determine continuous touch of objects against the skin ● Ruffini’s endings → Fusiform capsules anchored firmly to the surrounding connective tissue → SA2 → Stimulated by stretch (tension) and twisting (torque) → In joint capsules, signal degree of joint rotation → Important for signaling continuous states of deformation of the tissues ▪ Heavy prolonged touch ▪ Pressure signals ● Pacinian corpuscle → Large, oval, lamellated nerve endings found deep in dermis and hypodermis → Immediately beneath the skin and deep in the fascial tissues of the body → FA2 → Senses coarse touch, pressure, and vibrations Receptors in Hairy Skin ● SA1 fibers connect to Merkel’s discs ● SA2 fibers connect to Ruffini’s corpuscles ● FA2 fibers connect to Pacinian corpuscles → In tissues of muscles and blood vessels ● No exact analogue for FA1 fibers → Hair units wrap around hair follicles, connecting with ~20 hair units; extremely sensitive to movement of even one hair follicle → Field units respond to light touch in skin but have large receptive fields Other Tactile Receptors ● Free nerve endings → Found everywhere in the skin and in many other tissues → Detect touch and pressure → E.g. light contact with the cornea of the eye ● Hair end-organ → Consists of a hair and its basal nerve fiber → Adapts readily → Detects movement of objects on the surface of the body and initial contact with the body Transmission of Tactile Signals in Peripheral Nerve Fibers ● Transmission velocity → Almost all specialized sensory receptors - 30 to 70 m/sec → Free nerve ending tactile receptors (via small type Aδ myelinated fiber) - 5 to 30 m/sec → Some tactile free nerve endings (via type C unmyelinated fibers) up to 2 m/sec CM 100 Sensory Receptors and Somatic Sensations 6 of 15 ● Rapidly transmitted sensory signals → Precise localization on the skin → Minute gradations of intensity → Rapid changes in sensory signal intensity ● Slowly transmitted sensory signals (cruder type) → Pressure → Poorly localized touch → Tickle → Transmitted via very small nerve fibers requiring much less space in the peripheral nerve bundle Detection of Vibration ● Different receptors detect different frequencies of vibration ● Pacinian corpuscle - 30 to 800 cycles/sec → Respond extremely rapidly to minute and rapid deformations of the tissues → Type Aβ nerve fibers (1000 impulses/sec) ● Meissner’s corpuscle (and other low frequency vibrations) → Stimulated by low-frequency (slow) vibrations (2 up to 80 cycles/sec) → Adapt less rapidly than Pacinian corpuscles Detection of Tickle and Itch ● Detected by fast adapting free nerve endings → Very sensitive, rapidly adapting → Found almost exclusively in superficial layers of the skin → Skin - only tissue from which tickle and itch can be elicited → Transmitted by very small type C, unmyelinated fibers → Signal - scratch reflex C. PROPRIOCEPTION OF SKELETAL MUSCLES ● Golgi Tendon Organ (group Ib) → Small encapsulated nerve endings that penetrate among the collagen bundles at the myotendinous junction → Measures the force generated by the muscle from tension ● Muscle spindles → Several sensory nerves encapsulated by modified perimysium → With concentric layers of flattened cells containing interstitial fluid and intrafusal fibers → Contains two types of sensory endings ▪ Group Ia – sensitive to dynamics of muscle length ▪ Group II – sensitive to static length → Measure length and rate of stretch of muscles IV. SENSORY PATHWAYS FOR SOMATIC SIGNALS IN CNS A. ANATOMICAL ORGANIZATION ● First order neuron → Cell body is located in posterior root ganglion → Peripheral process connects with a sensory receptor ending → Central process enters spinal cord through posterior root ganglion; synapses with second order neuron ● Second order neuron → Gives rise to axon that decussates → Ascends to a higher level in CNS where it synapses with the third order neuron ● Third order neuron → Usually in the thalamus → Projects to a sensory region in the cerebral cortex B. SENSORY PATHWAYS ● Dorsal roots of the spinal nerves - entry point of sensory signals from the somatic segments ● Two alternative sensory pathways: → Dorsal column-medial lemniscal (DCML) system → Anterolateral system C. DORSAL COLUMN-MEDIAL LEMNISCATE SYSTEM ● Carries signals upward to the medulla of the brain mainly in the dorsal columns of the cord → Synapse and cross to opposite side of the medulla → Brain stem → Thalamus via medial lemniscus ● Large myelinated nerve fibers from specialized mechanoreceptors → Fibers divide upon entering spinal cord into medial and lateral branches ▪ Medial branch turns medially → Upward in dorsal column → Dorsal column pathway → Brain ▪ Lateral branch enters dorsal horn of cord gray matter → Divides many times → Terminals synapse with local neurons in intermediate and anterior portions of cord gray matter CM 100 Sensory Receptors and Somatic Sensations − Functions of the lateral branch neurons: o Major share of fibers enter dorsal columns of the cord then travel upward to the brain o Many fibers are short and terminate locally in the spinal cord gray matter → Elicit spinal cord reflexes o Give rise to the spinocerebellar tracts ● Signal transmission to the brain – 30 to 110 m/sec ● High degree of spatial orientation → In the dorsal columns of the spinal cord: ▪ Fibers from the lower parts of the body lie toward the center of the cord ▪ Those that enter the cord at higher segmental levels form successive layers laterally → In the thalamus: ▪ Distinct spatial orientation is still maintained ▪ The tail end of the body is represented by the most lateral portions of the ventrobasal complex ▪ The head and face are represented by the medial areas of the complex → Crossing of the medial lemniscus in the medulla causes contralateral representation of the body by the thalamus ● Limited to discrete types of mechanoreceptive sensations ● Types of sensations transmitted: 1. Touch sensations requiring a high degree of localization of stimulus 2. Touch sensations requiring transmission of fine gradations of intensity 3. Phasic sensations, such as vibratory sensations 4. Sensations that signal movement against the skin\ 5. Position sensations from the joints 6. Pressure sensations related to fine degrees of judgment of pressure intensity Damage to the DCML ● Below level of decussation: loss of fine somatosensory discriminatory ability on ipsilateral side of lesion ● Above level of decussation: loss of fine somatosensory discriminatory ability on contralateral side of lesion ● Agraphestesia and astereognosis ● Cutaneous pain and temperature are unaffected ● Visceral pain substantially diminished Trigeminal Pathway for Fine Touch and Proprioception of Face ● Primary afferent fibers → Synapse in several brainstem nuclei including main sensory nucleus and descending nucleus of trigeminal nerve ● Similar pathway to DCML ● Brainstem nuclei relay tactile information through contralateral ventral posteromedial (VPM) thalamic nucleus by way of the trigeminothalamic tract ● Third order neurons project to facial area of somatosensory cortex ● Senses touch, pressure, pain, temperature, and proprioception in face Spinocerebellar and Proprioceptive Pathways ● Dorsal (Posterior) Spinocerebellar Tract → Receive proprioceptive signals from muscle spindles and golgi tendons from trunk and lower limbs → Unconscious muscle joint sense ● Ventral (Anterior) Spinocerebellar Tract → Receive proprioceptive signals from muscle spindles and golgi tendons from trunk, and upper and lower limbs → Unconscious muscle joint sense Figure 13. Anatomy of the Dorsal Spinocerebellar Tract 7 of 15 ● Drowsiness or barbiturate anesthesia → Thalamic neurons tend to undergo an alternating sequence of excitatory and inhibitory postsynaptic potentials ● Spinothalamic tract → Also projects to other thalamic nuclei → Posterior nucleus and central lateral nucleus of intralaminar complex ● Intralaminar nuclei → Not somatotropically organized → Project diffusely to cerebral cortex and basal ganglia Figure 14. Anatomy of the Ventral Spinocerebellar Tract Proprioceptive Information to Cortex ● Ascending pathways of lower limb → Main axons of dorsal spinocerebellar tract give off a branch in the medulla which terminates in nucleus z → Axons from nucleus z then form part of internal arcuate fibers and medial lemniscus → They ascend to the VPL nucleus of the thalamus ● Ascending pathways of upper limb → Dorsal root ganglion fibers from cervical spinal levels ascend in cuneate fasciculus to external cuneate nucleus → Axons from external cuneate nucleus then form the cuneocerebellar tract → Enters cerebellum through inferior peduncle → Terminates in cerebellar cortex → Route to cerebral cortex for proprioception in upper limb is the same as that for discriminative touch (DCML) D. ANTEROLATERAL PATHWAY ● Pathway: Spinal cord from the dorsal spinal nerve roots → Dorsal horns of the spinal gray matter → Opposite side of the cord → Anterior and lateral white columns of the cord ● Termination: lower brain stem & thalamus ● Smaller myelinated fibers ● Signal transmission – few to 40 m/sec ● Less spatial orientation compared to the DCML ● Ability to transmit a broad spectrum of sensory modalities → E.g. pain, warmth, cold, and crude tactile sensations ● Types of sensations transmitted: 1. Pain 2. Thermal sensations (warm and cold) 3. Crude touch and pressure sensations capable only of crude localizing ability on the surface of the body 4. Tickle and itch sensations 5. Sexual sensations E. THALAMIC AND CORTICAL SOMATOSENSORY AREAS ● Ventroposterior nuclear complex of thalamus → Main termination site for ascending somatosensory information in diencephalon ● Two major nuclei → VPL ▪ Medial lemniscus forms main input ▪ Receives pain and temperature info from spinothalamic tract → VPM ▪ Trigeminothalamic tract forms the main input ● Smaller nucleus – VPI (ventral posterior inferior) → Responds to activation of nociceptors → Main input to spinothalamic tract Inhibitory and Excitatory Receptive Fields in Thalamus ● Inhibition may take place in: → Dorsal column nuclei → Dorsal horn of the spinal cord → Thalamus ● VPL and VPM contain GABAergic inhibitory interneurons ● GABAergic inhibitory interneurons in reticular nucleus of thalamus also project into VPL and VPM ● Thalamocortical and corticothalamic → Send axon collaterals to reticular nucleus ▪ Neurons complete feedback ▪ Feedforward inhibitory circuits with nucleus in other thalamic nuclei Thalamic Nuclei and Spinothalamic Tract ● Thalamic neurons depend on: → Sleep/wake cycle → Presence/absence of anesthesia CM 100 Sensory Receptors and Somatic Sensations F. SOMATOSENSORY CORTEX ● Third order neurons in thalamus project to the somatosensory cortex ● Divided into about 50 unique sections known as Brodmann's areas → Based on histological structural differences → Neurophysiologists and neurologists use the map as reference for many different functional areas of the human cortex by number Figure 15. Brodmann’s Areas ● Central Fissure → Extends horizontally across the brain → Generally, sensory signals from all feeling modalities terminate in the cerebral cortex immediately posterior to the central fissure → Anterior portion: motor cortex ▪ Constitutes the posterior half of the frontal lobe ▪ Control of muscle contractions and body movements ▪ Major share of motor control in response to somatosensory signals received from sensory portions of the cortex − Sensory portions keep motor cortex informed about positions and motions of different body parts at each instant ● Parietal lobe ▪ Anterior portion: Reception and interpretation of somatosensory signals ▪ Posterior portion: Provides higher levels of interpretation ● Occipital lobe – visual signals terminate ● Temporal lobe – auditory signals terminate ● Third-order sensory neurons in the thalamus project to the somatosensory cortex Somatosensory Areas I and II ● Main somatosensory receiving areas of the cortex ● Somatosensory Area I (S-I) cortex → Primary somatosensory cortex → More extensive and important than somatosensory area II → Located on the postcentral gyrus → Has a high degree of localization of different parts of the body → Responsible for the initial processing of somatosensory information → Begins higher-order processing such as feature extraction → Has a somatotopic organization ▪ Sensation for the face → lateral part of the postcentral gyrus, above the lateral fissure ▪ Sensation for upper limbs → dorsolateral part of the postcentral gyrus ▪ Sensation for lower limbs → medial surface of the hemisphere → Has a columnar organization ▪ Neurons along a line perpendicular to the cortical surface have similar response properties and receptive fields → Has functional and morphological subdivisions, with each having a somatotropic map ▪ Based on the arrangements of neurons in the various layers of the cortex ▪ Subdivisions are Brodmann areas 3a, 3b, 1, and 2 8 of 15 ▪ Cutaneous input → 3b and 1 ▪ Muscle and joint input (proprioceptive) → 3a and 2 ▪ Tactile and proprioceptive information → Separate cortical zones → Nearby cortical columns process information for different sensory modalities ▪ E.g. FA mechanoreceptors → 3b area; SA mechanoreceptors → Neighboring column ● S-II cortex → Secondary somatosensory cortex → Located in the superior bank of the lateral fissure → Contains a somatotopic map ● Sensory homunculus → Map of the surface of the body and face of a human on the postcentral gyrus → Distorted ▪ The volume of neural tissue devoted to a body region is proportional to the density of its innervation → Expression of place coding of somatosensory information → Layer VI ▪ Large numbers of axons extend to the thalamus ▪ Provides signals from cerebral cortex ▪ Control excitatory levels of incoming sensory signals entering the thalamus V. TEMPERATURE SENSATION ● Seen in the skin, hypothalamus, and spinal cord ● Most cutaneous thermoreceptors are free nerve endings with small axons (C and A𝛿 fibers) Warmth Receptors ● Begin firing at ~30ºC ● Rate plateaus at 44-46ºC ● Rate steeply falls beyond 46ºC; sensation replaced by pain ● Warm sensation → Mediated by Transient Receptor Potential (TRP) family of channels ▪ Specifically TRPV (Vanilloid) channels TRPV 1-4 → TRPVI ▪ Vanilloid receptor activated by capsaicin ▪ High temperature threshold; may mediate some painful aspects of heat ▪ Other TRPV classes activated at more moderate temperatures Cold Receptors ● Relatively quiet at 40ºC ● Rate peaks at 24-28ºC ● Rate decreases until temperature falls to ~10ºC ● <10ºC – firing stops and cold becomes effective local anesthetic ● Cold sensation → Mediated by TRP family, specifically TRPM (Melastatin) → TRPM8 ▪ Channels begin to open at ~27ºC, maximally activated at 8ºC ▪ Also a menthol receptor → TRPA 1 – cold sensitive ion channel V. PAIN SENSATION Figure 16. Representation of Different Areas of the Body in S-1 Effects of Somatosensory Cortex Lesions ● Produces sensory changes similar to somatosensory thalamus lesions, but more localized ● Usually only part of the cortex is involved → Sensory loss may be confined ▪ Depends on the location of the lesion with respect to the sensory homunculus ● Sensory modalities most affected are discriminative touch and position sense → Disturbed graphesthesia and stereognosis ▪ Ability to recognize objects as they are handled ● Pain and thermal sensation may be relatively unaffected Layers of the Somatosensory Cortex ● Contains six layers of neurons ● Neurons in each layer perform functions different from the following layers: Table 4. Layers of the Somatosensory Cortex Layer Function Layer IV ● First to be excited by incoming sensory signal ● Signal spreads toward the surface of the cortex towards deeper layers Layer I and II ● Receive diffuse, nonspecific input signals from lower brain centers that facilitate specific regions of the cortex Layer II and III ● Neurons send axons to related portions of the cerebral cortex on opposite side of brain → Via corpus callosum Layer V and VI ● Send axons to deeper parts of the nervous system → Layer V ▪ Larger and project to more distant areas (basal ganglia, brain stem, spinal cord) ▪ Control signal transmission CM 100 Sensory Receptors and Somatic Sensations A. NOCICEPTORS ● Comes from the Latin “nocere” (to hurt) and “recipere” (to receive) ● Mediates pain sensations and warns the body of damage ● Free nerve endings that are widely distributed throughout the body → Absent in the brain parenchyma ● A𝛿 vs C pain fibers → A𝛿 fibers ▪ Fast pain (first pain) ▪ Sharp and highly localized ▪ Terminate in laminas I, V, and X of dorsal horn → C fibers ▪ Slow pain (second pain) ▪ Duller, more diffuse ▪ Terminate in laminas I and II of dorsal horn Selectivity of Nociceptors ● Mechanical nociceptors → Respond to pressure, particularly those from sharp objects ● Thermal nociceptors → Heat-sensitive nociceptors express TRPV1 and TRPV2 ▪ Activated at 45ºC when tissues begin to be destroyed → Cold-sensitive nociceptors express TRPM8 and TRPA1 ▪ Activated <15ºC ● Chemical nociceptors → Respond to a variety of agents: ▪ K+, pH extremes, neuroactive substances like histamine, bradykinin, and various environmental irritants ● Polymodal nociceptors → Contain a combination of the abovementioned receptors B. POSITIVE MODULATION OF PAIN SENSATIONS ● Damaged tissues are more sensitive to further stimuli and exhibit hyperalgesia ● Primary hyperalgesia – occurs in area of damaged tissue ● Secondary hyperalgesia → Occurs around 20 minutes after → Affects surrounding tissues ● Axon reflex (in order): → Damaged tissues release substances that promote inflammation → Mast cells release histamine, directly exciting nociceptors 9 of 15 → Action potentials propagate and spread into branches of same axons innervating neighboring regions → Spreading axon branches release substances that sensitize other nociceptive terminals Negative Modulation ● How pain is perceived is strongly under the control of the brain → Nociceptors can fire wildly yet illicit very low perception of pain → Excruciating pain can be perceived even when there are no nociceptors firing ● Pain can be modified by both: → Nonpainful sensory input → Neural activity from other nuclei within the brain → Pain evoked by nociceptors can be reduced by simultaneously activating low threshold mechanoreceptors → Activation of A and A fibers leads to release of GABA and other neurotransmitters in the dorsal horn ● Presence of endorphins (endogenous morphine) and enkephalins → Modulate pain by binding to opioid receptors in brain ● Phantom limb → Follows amputation of limbs in some individuals ● Central pain → Can be caused by lesions in thalamus or along spinothalamocortical pathway → Severe and spontaneous pain → Interruption of nociceptive pathway by same lesion can simultaneously reduce or prevent the pain VI. REFERENCES Hall, J. & Hall, M. (2021). Guyton and Hall’s Textbook of Medical Physiology (14th Edition). Rivera, R. (2023). The Somatic Senses [Lecture]. C. CENTRAL PAIN PATHWAYS ● Spinothalamic tract → Most important pathway for somatic pain and temperature sensations ● Terminate in the VPI although some terminate in the VPL ● Nociceptive signals → Transmitted to somatosensory cortex and other cortical areas involved in affective response → To cingulate gyrus and insula ● Cells signaling visceral input also convey information from cutaneous receptor → “Referred pain” Spinothalamic Tract ● Cells with inhibitory receptive fields ● Inhibition may come from weak mechanical stimuli ● Most effective inhibition often from noxious stimuli ● Nociceptive inhibitory fields → Encompass a large area → May account for effectiveness of various physical manipulations such as TENS and acupuncture Spinoreticular Tract ● Typically have large receptive fields ● Dorsal horn neurons from this tract target multiple regions in medullary and pontine reticular formation ● Reticular formation → Involved in arousal and attention → Also gives rise to reticulospinal projections which control the transmission of pain Spinomesencephalic Tract ● Tract terminates in several midbrain nuclei including periaqueductal gray → Important component of endogenous analgesia system ● Information from midbrain relayed to thalamus and amygdala the Effects of Lesions Along the Spinothalamic Tract and Thalamus ● Loss of discriminative and motivational affective components of pain on contralateral side of body ● Anterolateral cordotomy can be done to treat chronic pain → Especially in cancer (done rarely nowadays) ● Destruction of VPL and VPM → Diminishes contralateral sensation of body or face → Mostly due to the damage to the DCML and its trigeminal equivalent → Discriminative component of pain also lost ● Thalamic pain → Central pain state due to lesions in somatosensory thalamus → Even slightest touch induces pain Neuropathic Pain ● Pain that occurs in the absence of nociceptive stimuli ● Likely occurs when there is damage to any part of the pathways involved in transmitting nociceptive information ● Causalgia → Develops when a peripheral nerve is damaged → Pain is experienced along the area supplied by the damage nerve → Very difficult to treat CM 100 Sensory Receptors and Somatic Sensations 10 of 15 APPENDIX Figure 16. Receptive Fields Figure 17. Dermatomes Figure 18. Pathway of the Dorsal Column-Medial Lemniscal System CM 100 Sensory Receptors and Somatic Sensations 11 of 15 Table 3. Comparison of Sensory Pathways for Transmitting Somatic Signals into the Central Nervous System Rate of adaptation Information transmitted DCML Anterolateral Slowly adapting Rapidly adapting Constant status of the body Rapid tissue deformations Note: Information was directly taken from the Guyton & Hall’s Textbook of Medical Physiology (14th Edition), (2021). However, these were not lectured by Dr. Rivera. PROLONGATION OF A SIGNAL BY A NEURONAL POOL ● Afterdischarge → Phenomenon wherein a signal entering a pool causes a prolonged output discharge → Lasts a few milliseconds to as long as many minutes after the incoming signal is over Synaptic Afterdischarge ● Especially when long-lasting synaptic transmitter substances are used, excitatory synapses discharge on dendrites create a postsynaptic electrical potential lasting for many milliseconds ● Afterdischarge continues to excite the neuron, causing continuous emission of output impulses ● Afterdischarge can sustain a signal output from a single instantaneous input signal Reverberatory Circuits ● Re-excitation of input in same circuit that causes sustained repetitive discharge ● Single neuron reverberation → Output neuron sends nerve fiber back to its own dendrites or some for restimulation ● Additional neurons in the feedback circuit causes longer delay between initial discharge and the feedback signal ● Reverberatory Circuit with Facilitatory and Inhibitory Fibers → Facilitatory signals enhance reverberation intensity and frequency, while inhibitory signals depress or stops the reverberation ● Reverberatory Circuit with Parallel Fibers → Strength of total reverberating signal depends on number of parallel fibers momentarily involved in the reverberation Signal Prolongation ● In reverberatory circuits, input stimulus causing short response can create longer outputs ● Critical Point is where intensity of output signal peaks before total cessation, which can be caused by fatigue in the synaptic junctions of the circuit ● Fatigue can break a circuit feedback by lowering threshold level of subsequent neurons ● Duration of total signal before cessation is controlled by signals from brain regions with inhibitory or facilitative effects on the circuit ● Continuous Signal Output ● Output signals are emitted continuously, even without excitatory input signals ● Caused by: → Intrinsic Neuronal Excitability ▪ Repetitive discharge if the tissues’ level of excitatory membrane potential rises above a certain threshold level ▪ Occurs in neurons of cerebellum, interneurons of spinal cord ▪ Rate of firing can be increased (excitatory signals) or decreased (inhibitory signals) − Inhibitory signals can decrease firing rate to zero → Reverberating Circuit ▪ Excitatory and inhibitory control signals are not the cause of the output signals, but they control the changing level of intensity ▪ Signals can be increased or decreased by accessory input signals into the reverberating neuronal pathway ▪ ANS to vascular tone, gut tone, constriction of iris in the eye, and heart rate Rhythmical Signal Output ● From reverberating circuits or succession of sequential reverberating circuits that feed signals in a circular pathway from one neuronal pool to the next CM 100 Sensory Receptors and Somatic Sensations ● (e.g.) Changes in respiratory signal output in phrenic nerve → Arterial oxygen deficiency → Carotid body stimulated → Frequency and amplitude of respiratory rhythmical output signal increase progressively INSTABILITY AND STABILITY OF NEURONAL CIRCUITS ● Prevent the continuous re-excitation and transmission of no information signals in the brain Inhibitory Circuits ● Inhibitory Feedback Circuits → Return from the termini of pathways to the initial excitatory neurons of the same pathways → Occur in all sensory nervous pathways → Inhibits either the input neurons or intermediate neurons when the termini become overly excited ● Neuronal Pools Exerting Gross Inhibitory Control → Controls widespread areas of brain → Occurs in many basal ganglia influencing muscle control system Synaptic Fatigue ● Synaptic transmission becomes progressively weaker the more prolonged and more intense the period of excitation → The shorter the interval between successive flexor reflexes, the less the intensity of subsequent reflex response ● Overused pathways = rapidly fatigues, sensitivities decrease ● Underused pathways = rested, sensitivities increase ● Long-term sensitivity of synapses can be change by upregulation or downregulation of receptor proteins at synaptic sites Referred Pain ● Pain in a part of a body fairly remote from the tissue causing the pain ● Important in visceral ailments: clinical sign is referred pain ● Mechanism of Referred Pain → Stimulation of visceral pain fibers → Conduction of pain signals from viscera through same neurons conducting pain from the skin → Person feels the sensations originating from the skin Figure 4. Mechanism of referred pain and referred hyperplasia Branches of visceral pain fibers synapse in the spinal cord on the same second-order neurons (1 and 2) receiving the pain signals from the skin Visceral Pain ● Pain from the viscera ● Visceral pain from abdomen and chest is a criterion used for diagnosing visceral inflammation, visceral infectious disease, and visceral ailments → Transmitted through type C pain fibers → Pain type: chronic, aching, suffering ● Often, viscera have sensory receptors only for pain ● Highly localized damage to viscera seldom cause severe pain ● Diffuse stimulation of pain nerve endings causes severe pain ● Causes of True Visceral Pain → Ischemia ▪ Formation of acidic metabolic end products or tissue-degenerative products − bradykinin, proteolytic enzymes 12 of 15 → Chemical stimuli ▪ Leak of damaging substance − proteolytic acidic gastric juice → Spasm of a Hollow Viscus ▪ Mechanical stimulation of pain nerve endings of a portion of gut, gallbladder, bile duct, ureter, and other hollow viscus ▪ Caused by diminished blood flow to muscle + increased metabolic need for nutrients ▪ Pain from spastic viscus: cramps − appendicitis, gastroenteritis, constipation, menstruation, parturition, gallbladder disease, ureteral obstruction → Overdistention of a Hollow Viscus ▪ Extreme overfilling of hollow viscera can lead to pain. ▪ Overdistention may collapse blood vessels around or within the organ, possibly causing ischemic pain. → Insensitive Viscera ▪ Some visceral areas are almost entirely insensitive to pain, including liver parenchyma and lung alveoli. ▪ Liver capsule is highly sensitive to direct trauma and stretching. ▪ Bile ducts in the liver are sensitive to pain. ▪ In the lungs, alveoli are insensitive, but bronchi and parietal pleura are very sensitive to pain ● “Parietal pain” caused by visceral disease → Disease affecting a viscus can spread to the parietal peritoneum, pleura, or pericardium → Parietal surfaces, like the skin, have extensive pain innervation from peripheral spinal nerves ● Location of visceral pain → The patient's brain lacks direct knowledge of internal organs, making it challenging to pinpoint the exact location of internal pain. → Sensations from the abdomen and thorax have two pathways to the central nervous system ▪ True visceral pathway - true visceral pain travels through autonomic nerve bundles ▪ Parietal pathway - parietal sensations, are transmitted directly to local spinal nerves from the parietal peritoneum, pleura, or pericardium ● Transmission of Referred Pain via Visceral Pathways → Referred pain from visceral organs is often localized in the dermatomal segment associated with the organ's embryonic origin, not its current location ▪ Example: Heart pain originates in the neck and upper thorax during embryonic development, so it's referred to areas like the neck, shoulder, pectoral muscles, arm, and substernal area ▪ Pain typically occurs on the left side due to the left side of the heart being more commonly involved in coronary disease ● Pain from viscera is often localized in two body areas due to dual transmission through referred visceral and direct parietal pathways Clinical Abnormalities of Pain and Other Somatic Sensations ● Hyperalgesia - excessive sensitivity to pain. → Possible causes: ▪ Primary hyperalgesia: Excessive sensitivity of pain receptors. ▪ Secondary hyperalgesia: Facilitation of sensory transmission. ● Herpes Zoster (shingles) - results from herpesvirus infection in a dorsal root ganglion → Causes severe pain in the dermatomal segment served by the infected ganglion, resulting in a segmental type of pain that encircles about half of the body ● Tic Douloureux (trigeminal/glossopharyngeal neuralgia) characterized by lancinating or stabbing pain on one side of the face. → This pain feels like sudden electrical shocks and can be intermittent or almost continuous ● Brown-Séquard Syndrome - occurs when the spinal cord is partially transected on one side, as opposed to complete transection → Motor functions on the same side as the transections are blocked in all segments below the level of the transection → Some sensory modalities are lost on the transected side, while others are lost on the opposite side ● Headaches - form of pain felt on the surface of the head, originating from deep head structures → Headache of meningitis → Headache caused by low CSF CM 100 Sensory Receptors and Somatic Sensations → Migraine headache → Alcoholic headache PAIN RECEPTORS ● Free nerve endings → Pain receptors in the skin and other tissues are all free nerve endings → Widespread in the superficial layers of the skin, periosteum, arterial walls, joint surfaces, falx, and tentorium → Most other deep tissues are only sparsely supplied → Any widespread tissue damage can summate to slow, chronic, aching type of pain Rate of Tissue Damage as a Stimulus for Pain ● Above 45°C → Heat pain on skin starts to be perceived → Tissues begin to damage ● Heat pain → Correlated to the rate at which damage to the tissue is occurring, not with the total damage that has already occurred. ● Pain intensity → Correlated with the rate of tissue damage ▪ E.g. other than heat: bacterial infection, tissue ischemia, tissue contusion, etc. → Correlated with a chemical pain stimuli ▪ Bradykinin is believed to be the agent most responsible for causing pain after tissue damage → Correlated with local increase in K+ concentration or increase in proteolytic enzymes ▪ Proteolytic enzymes directly attack the nerve endings and excite pain by making the nerve membranes more permeable to ions ● Tissue Ischemia → Causes pain within few minutes after the blood flow to a tissue is blocked → Suggested cause of pain is the accumulation of lactic acid in tissues upon anaerobic metabolism → Can also be caused by chemical agents formed in the tissues upon cell damage: bradykinin and proteolytic enzymes → Greater rate of metabolism of tissue = more rapid pain ▪ E.g. blood pressure cuff placed and inflated around the upper arm until the arterial blood flow ceases − muscle pain on forearm within 15-20 secs (when it’s exercised) − muscle pain on forearm may not appear for 3-4 mins (in the absence of muscle exercise) ● Muscle Spasm → Common cause of pain and a basis of many clinical pain syndromes → Increases rate of metabolism in the muscle tissue → Direct effect: stimulation of mechanosensitive pain receptors → Indirect effect: compression of blood vessels THERMAL RECEPTORS ● Seen in the skin, the hypothalamus, and the spinal cord ● Most cutaneous thermoreceptors are free nerve endings with small axons (A∂ and C fibers) Table 1. Warmth Vs. Cold Receptors Warmth Receptor Cold Receptor ● Begin firing at approx. 30oC ● Relatively quiet at 40oC ● Rate plateaus at 44-46oC ● Rate peaks at 24-28oC ● Rate steeply falls beyond 46oC ● Rate then decreases until and sensation is replaced by temperature falls to approx. pain 10oC ● Below approx. 10oC, firing stops and cold becomes effective local anesthetic Table 2. Warm VS Cold Sensations Warm Sensation Cold Sensation ● Mediated by the Transient ● Mediated by the TRP family, Receptor Potential (TRP) family specifically the Transient of channels, specifically the Receptor Potential Melastanin Transient Receptor Potential (TRPM) Vanilloid (TRPV) channels 1-4 ● TRPM8 channels begin to open ● TRPV1 at approx. 27oC and are → Vanilloid receptor maximally activated at 8oC 13 of 15 → Activated by capsaicin → Has high temperature threshold and may mediate some of the painful aspects of heat ● Other TRPV classes are activated at more moderate temperatures ● TRPM8 is also a menthol receptor ● TRPA1 is a cold sensitive ion channel DUAL PATHWAYS IN CNS FOR TRANSMISSION OF PAIN ● All pain receptors are free nerve endings ● Tw separate pathways for transmitting pain signals into the CNS: → Fast-sharp pain pathway → Slow-chronic pain pathway ● The double system pain innervation often gives a “double” pain sensation on a sudden painful stimulus → Fast-sharp pain (small type Aδ fibers) to the brain, and then slow pain (type C fibers) by a second or so later ● Fast-sharp pain signals → Elicited by either mechanical or thermal pain stimuli → Small type Aδ fibers ▪ Transmitted in peripheral nerves to spinal cord at velocities between 6 and 30 m/s → Apprises the person rapidly to pain ▪ Makes the person react immediately to remove himself/herself from the stimulus. ● Slow-chronic pain signals → Elicited mostly by chemical stimuli, sometimes by persisting mechanical or thermal stimuli → Type C fibers ▪ Transmitted in peripheral nerves to spinal cord at velocities between 0.5 and 2m/s → Tend to become greater over time → Eventually produce intolerable pain, and make the person keep trying to relieve the cause of the pain ● Transmission of both “fast-sharp” and “slow-chronic” pain signals: → entrance to dorsal spinal roots > interneurons (at dorsal horns) > 2 processing systems on the way to the brain (neospinothalamic tract or paleospinothalamic pathway) Figure 5. Two processing systems of pain into the brainstem, thalamus, and cerebral cortex Neospinothalamic Tract for Fast Pain ● Fast pricking pain pathway ● Neospinothalamic Tract sequence: → Aδ fibers → Lamina I (lamina marginalis) of the dorsal horns → 2nd order neurons of neospinothalamic tract (long fibers which cross to the opposite side of the cord → Anterior commissure → Upward to the anterolateral columns in the brain ● Termination in the brainstem and thalamus: → Reticular areas (few fibers) → Ventrobasal complex (many fibers, uninterrupted) ▪ Termination along with dorsal column-medial lemniscal tract for tactile sensations → Posterior nuclear group (few fibers) → Signals from the aforementioned thalamic areas are transmitted to other basal areas of the brain, and to the somatosensory cortex CM 100 Sensory Receptors and Somatic Sensations ● Localization of fast pain: → Fast-sharp pain is more exactly localized than slow-chronic pain → Poor localization occurs when pain receptors are only stimulated, without stimulation of tactile receptors (within 10 cm or so to the stimulated area) → Exact localization occurs during simultaneous excitation of dorsal column-medial lemniscal system by the tactile receptors ● Glutamate → Believed to be secreted at type Aδ pain nerve fiber endings → One of the most widely used excitatory transmitters in CNS → Duration of action lasts for only a few milliseconds Paleospinothalamic Pathway ● Slow burning pain pathway ● Much older system ● Transmission via peripheral slow-chronic type C pain fibers ● Transmit some signals from type Aδ fibers ● Paleospinothalamic sequence: → Peripheral fibers → Substanstia gelatinosa in spinal cord (laminae II + lamina III of dorsal horns) → Short fiber neurons within dorsal horns → Lamina V in dorsal horns → Long axons passing through anterior commissure to the opposite cord > (upward) >> anterolateral pathway in the brain ● Substance P → Slow-chronic neurotransmitter of type C nerve endings → Released more slowly than glutamate (seconds to minutes) → Double pain sensation (pinprick): glutamate acts first, followed by substance P ● Projection of Paleospinothalamic Pathway → Terminates in brain stem: ▪ Reticular nuclei of the medulla, pons, and mesencephalon ▪ Tectal area of the mesencephalon to superior and inferior colliculi ▪ Periaqueductal gray region surrounding the aqueduct of Sylvius → Only 10-25% pass all the way to thalamus ▪ Multiple short-fiber neurons relay pain signals into intralaminar and ventrolateral nuclei of thalamus and portions of hypothalamus ● Poor capability of NS to Localize Precisely the Source of Pain → Imprecise pain transmission ▪ Due to pathway’s multisynaptic, diffuse connectivity ● Function of Reticular Formation, Thalamus, and Cerebral Cortex in Pain Appreciation → Complete removal of somatic sensory of cerebral cortex ≠ no pain perception → Cortex interprets pain quality though it is the principal function of lower centers ● Special Capability of Pain Signals to Arouse Brain → Electrical simulation in reticular areas of brain stem and intralaminar nuclei of thalamus has strong arousal effect on brain → Example: a person in severe pain cannot sleep ● Surgical Interruption of Pain Pathways → Done to provide pain relief for severe and intractable pain ▪ Rapidly spreading cancer → Cordotomy ▪ Cutting of pain-conducting tracts of spinal cord anterolaterally (opposite the pain source) ▪ Done for pain located lower part of body ▪ Not always successful: − Pain fibers upper part of body do not cross opposite side of spinal cord: cannot be transected − Return of pain as a result of sensitization of other pathways PAIN SUPPRESSION SYSTEM IN THE BRAIN AND SPINAL CORD ● Analgesia system → Pain control system: capability of brain to suppress pain signals → Result: variation in the degree of pain reaction of an individual → Block pain signals at initial entry point (spinal cord) → Block local cord reflexes from pain signals ▪ Withdrawal reflexes ● Major Components: → Periaqueductal gray and Periventricular areas 14 of 15 ▪ Mesencephalon and upper pons (aqueduct of Sylvius) and portions of 3rd and 4th ventricle ▪ Suppress strong pain signals entering via dorsal spinal roots ▪ Areas at higher levels of brain exciting periaqueductal gray: − Periventricular nucleus (hypothalamus) and medial forebrain bundle (hypothalamus) → Raphe magnus nucleus and Nucleus reticularis paragigantocellularis ▪ Thin midline nucleus located in lower pons and upper medulla ▪ Second order signals transmitted down the dorsolateral columns in spinal cord ▪ Suppress strong pain signals entering via dorsal spinal roots → Pain inhibitory complex ▪ Dorsal horns of spinal cord ▪ Point where analgesia signals can block pain before being relayed to brain ● Transmitters of analgesia system: → Enkephalin ▪ Cause presynaptic and postsynaptic inhibition of incoming type C and type Aδ pain fibers ▪ Secreted by nerve fibers from periventricular nuclei and periaqueductal gray area → Serotonin ▪ Secreted by nerve fibers from raphe magnus nucleus ▪ Also causes local cord neurons to secrete enkephalin ● Brain’s Opiate System → Causes extreme degree of analgesia → Morphine-like agents (opiates) are found in dorsal horns of spinal cord → Morphine receptors of analgesia system: receptors for morphine-like neurotransmitters secreted by brain → Opiate-like substances of NS: ▪ β-endorphin - hypothalamus and pituitary gland ▪ Met-enkephalin - brainstem and spinal cord ▪ Leu-enkephalin - brainstem and spinal cord ▪ Dynorphin - brainstem and spinal cord (lower quantity) ▪ Protein Molecules of Opiate-like substances of NS: Pro-opiomelanocortin, Proenkephalin, and Prodynorphin CM 100 Sensory Receptors and Somatic Sensations 15 of 15