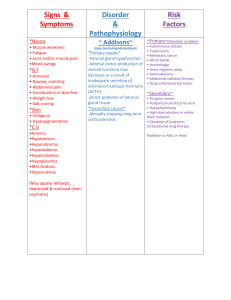
Med-Surg - Gastrointestinal System, part 1: Introduction, Anatomy and Physiology Review The gastrointestinal system provides nutrients to support the body's functions through digestion, and it also allows for elimination of waste products through defecation. There are three main components of the GI system. One is the alimentary canal, so this includes the oral cavity, the pharynx, esophagus, stomach, small intestine, large intestine, rectum, and anal canal. Then we also have accessory organs, which include the salivary glands, the liver, the pancreas, and the gallbladder. And then we have the peritoneum, which is the serous membrane that holds the digestive organs in place in the abdominal cavity of the body. All right. Let's now go into a little more detail of each of the components of the alimentary canal. And this illustration can be found in our Medical-Surgical Nursing Flashcard deck. So first of all, we have the oral cavity, which contains the buccal mucosa, lips, tongue, hard palate, soft palate, and teeth. You can also see the salivary glands here. Functions of the oral cavity include mechanical and chemical digestion. So we have mechanical digestion that is taking place, which is the grinding of food into smaller pieces through mastication. And we also have chemical digestion, which is taking place. So digestion of carbohydrates will begin in the oral cavity through the action of salivary amylase, which is an enzyme. Then from the oral cavity, the food will move through the pharynx down the esophagus. So the esophagus is a muscular tube that connects the pharynx to the stomach, and it contains two sphincters. So we have this upper esophageal sphincter, which helps to protect against reflux of food into the airways and also prevents entry of air into the digestive tract. And then we have this lower esophageal sphincter, which prevents reflux of gastric contents into the esophagus. So when we talk about GERD or gastroesophageal reflux disease, that disorder is associated with a weakened lower esophageal sphincter. All right. So from the esophagus, the food will move into the stomach and the top part of the stomach here is the fundus, then we have the body and the pylorus here at the end. So functions of the stomach include mechanical and chemical digestion. So there's a variety of cells here in the stomach that we've outlined on the flashcard, which include neck cells, G-cells, parietal cells, and chief cells. So those cells will secrete mucus, gastrin, and hydrochloric acid. And basically, the food will be mixed with gastric secretions to form chyme, which which is spelled C-H-Y-M-E. And this chyme will empty into the small intestine. All right. So the small intestine has three parts. From proximal to distal, we have the duodenum, the jejunum, and the ilium. So our little cool chicken hint here on the card is that DJ Ilium plays at the GI club. So if I ever become a DJ, I'm totally calling myself DJ Ilium, and you guys are all invited to my club. All right. So in the small intestine, we have digestion that takes place as well as absorption. And then we have peristalsis which moves the food from the stomach to the large intestine. A couple of other things I want to mention about the small intestine. Inactivated pancreatic enzymes will enter the duodenum and become activated and help to digest carbohydrates, fats, and protein. We also have bile that enters the duodenum and that helps to emulsify fat. All right, then the food moves to the large intestine. So structures in the large intestine include the cecum, the ascending colon, the transverse colon, the descending colon, the sigmoid colon, and the rectum and anal canal. So feces will move through the colon through segmental contractions. In the colon, we have the absorption of water and electrolytes. So if a patient has to have their colon removed, we're not going to have that absorption of water and they are going to have very liquid stool. And then defecation is controlled by both internal and external anal sphincters. Med-Surg - Gastrointestinal System, part 2: Pancreas, Liver, Gallbladder, Biliary Tract Anatomy and Physiology Review Let's first talk about the pancreas, which has both exocrine and endocrine functions. As an exocrine organ, the acinar cells in the pancreas will secrete inactivated enzymes that travel to the small intestine where they become activated, and then they help to digest carbohydrates, fats, and protein. Now, later on in this playlist, we're going to talk about pancreatitis, which is a disorder that causes premature activation of those enzymes before they reach the small intestine and that causes auto digestion of the pancreas. As an endocrine organ, the islets of Langerhans are cells that produce hormones that regulate blood sugar levels in the body. So examples of hormones include insulin and glucagon. So if you want more details about the endocrine function of the pancreas, definitely go and check out my endocrine system playlist. So I go in a lot of detail in that playlist about insulin and diabetes, etc. Next, we have the liver, which is comprised of two lobes, and each lobe is made up of lobules, which are the functional units of the liver. The liver is responsible for many things in the body. This includes the storage of minerals and fat-soluble vitamins, bile production and secretion, bilirubin metabolism and secretion, detoxification of harmful drugs and substances. It's also responsible for plasma protein synthesis. For example, albumin and clotting factors. So albumin is an important protein that keeps fluid in the bloodstream, and clotting factors are needed for clotting or hemostasis. The liver also plays a role with fat metabolism, including cholesterol synthesis and elimination. It plays a role in carbohydrate metabolism as well. For example, glycogenolysis is the breakdown of glycogen, which is stored carbohydrate energy in the liver, and it breaks down that glycogen to glucose as needed. So you can see that there are a lot of different functions of the liver. So when we talk about disorders of the liver, such as cirrhosis, we're going to see a laundry list of signs and symptoms associated with those disorders because of all of these functions. Next, we have the gall bladder, which is a pear-shaped organ that is located underneath the liver. So the gallbladder stores and concentrates bile from the liver. So the liver makes the bile. The gallbladder stores that bile, and then it releases bile into the small intestine where it emulsifies fat. Let's take a look at the biliary tract. Here's an illustration from our medical-surgical nursing flashcard deck. So when I was in nursing school, I longed for a simplified illustration like this to better understand the different ducts and the flow of bile, and I never did find it. So I hope this illustration is helpful for you along with my explanation. So here we have the gallbladder, and that resides underneath the liver, which is not shown, but we do show the left and right hepatic ducts, which would be coming off the liver. So the left and right hepatic ducts combine to form the common hepatic duct. And so off of the gallbladder, we have the cystic duct, which combines with this common hepatic duct to form the common bile duct. And then the common bile duct combines with the pancreatic duct, and then it empties into the small intestine here at the sphincter of Oddi, which is in the duodenum. So bile will leave here, go through the cystic duct, come down here, go through the common bile duct and then into the small intestine. So later on in this video playlist, we're going to talk about cholecystitis, which is the inflammation of the gallbladder, and that is typically caused by cholelithiasis, which is a gallstone. So depending on where that gallstone is will determine what kinds of signs and symptoms your patient will have. So often you will find that gallstone in the cystic duct, which will cause inflammation of the gallbladder and symptoms that are specific to the gallbladder. However, if that gallstone resides in the common bile duct, then we can end up with bile backing into the liver, which will cause liver symptoms as well as gallbladder symptoms. And we can even have a gallstone that causes issues with this pancreatic duct, which in turn can cause pancreatitis. Med-Surg - Gastrointestinal System, part 3: Diagnostic Tests The first test I'm going to talk about is an EGD, which is an esophagogastroduodenoscopy. This is a procedure that is done under moderate sedation, where a scope is inserted down the throat, and the esophagus, stomach, and the duodenum are visualized with that camera. And the patient needs to be NPO for about six to eight hours before the procedure, or per facility policy. No kind of bowel prep is needed for this procedure because we're going in this way. However, with a sigmoidoscopy, which goes up this way - this procedure visualizes the anus, rectum, and sigmoid colon - anesthesia is not required, but you do have to have the patient be NPO after midnight before the procedure, and they will need to drink polyethylene glycol, some kind of drink such as GoLytely, to clean out those bowels. Then we have a colonoscopy, which is done under moderate sedation, like the EGD. With a colonoscopy, we scope much further in so we can visualize the anus, rectum, sigmoid colon, descending colon, transverse colon, and the ascending colon. So just like with the sigmoidoscopy, the patient will need to be NPO after midnight, and they will need to consume some of that polyethylene glycol in order to clean out the bowels. So any time I talk about a colonoscopy, I remember one night as a new grad on night shift, where I had to give, literally, like four gallons of GoLytely, which is polyethylene glycol, to a bed-bound patient. And let me just say I will never forget that evening, and thank goodness for my amazing CNAs who were there by my side, helping with that situation. Next, we have a gastrointestinal series, or GI series, which is a procedure that is used to identify GI abnormalities such as an ulcer, tumor, or obstruction. So with this procedure, the patient will drink some barium and x-rays are taken as the barium moves through the patient's GI tract. So the patient will need to be NPO for eight hours prior to the procedure. In addition, they should not smoke or chew gum for eight hours prior to the procedure and then after the procedure. You want to encourage a patient to increase their fluid intake in order to flush out that barium. In addition, you should warn them that their stools will be whitish in color for several days until that barium is cleared out. Lab values associated with the gastrointestinal system as well as the expected range for each of those lab values can be found in our medical-surgical nursing flashcard deck. You can also find those lab values and ranges in our lab values flashcard deck, which also contains my silly ways and mnemonics for remembering those ranges. So if you struggle with lab values, you may want to check that deck out. All right. AST and ALT, if those levels are elevated, that is strongly indicative of liver dysfunction, such as cirrhosis or hepatitis. Amylase and lipase are pancreatic enzymes. So if we have an increase in either of those enzymes, then that is indicative of pancreatic dysfunction, such as pancreatitis. Bilirubin will be elevated in the presence of liver dysfunction. Other causes of elevated bilirubin include hemolytic anemia, as well as a blood transfusion reaction. Ammonia will be elevated in the presence of liver disease. So a patient with advanced cirrhosis will often have elevated ammonia levels, and that can cause encephalopathy. So ammonia will build up in the brain and cause confusion in that patient. Albumin, prealbumin, and total protein may be decreased in the presence of liver dysfunction, but these values will also be decreased if the patient has malnutrition. Med-Surg - Gastrointestinal System, part 4: Dysphagia, GERD, Hiatal Hernia So let's start with dysphagia, which is difficulty swallowing. This can be caused by a structural abnormality. It can also be caused by a disorder that affects the nerves or muscles that are involved in swallowing. So examples of disorders that can result in dysphagia include a stroke, cerebral palsy, Parkinson's and ALS. Signs and symptoms of dysphagia include coughing and frequent clearing of the throat, difficulty with eating or drinking and aspiration pneumonia. So aspiration pneumonia is where food or liquid ends up down in the airways, so in the lungs, and that causes inflammation and infection. So in terms of diagnosis, when we suspect that a patient has difficulty swallowing, we need to make sure a referral is sent to the speech language pathologist. This is the member of the interdisciplinary team that is going to come and evaluate the patient's swallowing ability and make recommendations in terms of diet. So after the speech language pathologist sees the patient, they will recommend one of four levels of a diet. So level one dysphagia diet means that all of the patients food is going to be pureed and their liquids are going to be thickened. So in the hospital, we have some pre-thickened liquids that you can give the patient. But if the patient wants something like coffee, you have to mix this special thickening powder in with the coffee to thicken those liquids, which makes it easier to swallow. And any day that I work with a patient who has to consume thickened liquids, I'm just so grateful that I can swallow effectively, and I don't have to drink that stuff because it is not appetizing. Anyway, so that level one is the more serious dysphagia. And again, it's all pureed. If we have level two or three, that's going to include soft and moist foods. In addition to a speech language pathologist evaluation, other diagnostic tools include a barium swallow test as well as an EGD to try to identify any kind of structural abnormalities. In terms of treatment, like I mentioned, someone with dysphagia will need to have their liquids thickened, and the dysphagia diet will include either pureed or soft and moist foods. In addition, we want to make sure the head of the bed is up when the patient is consuming food, because when they're laying down, it makes aspiration much more likely. We also need to teach our patient to tuck their chin against their chest when they are swallowing, so they need to tuck it like that. They should not be extending their neck back when they're swallowing. It should be tucked, so provide that guidance. And then in worst case scenarios, if the patient cannot safely consume food because of their dysphagia, they may require a feeding tube. Next, let's talk about GERD, which is gastro esophageal reflux disease. So this is where the gastric contents which contain just of enzymes back flows into the esophagus, and it causes pain and mucosal damage, so it leads to esophagitis, which is inflammation of the esophagus. It can also lead to something called Barrett's esophagus. So when the cells in the esophagus are repeatedly exposed to that stomach acid, they mutate and that turns into Barrett's esophagus. And that places the patient at high risk for esophageal cancer. So the pathophysiology behind GERD is that we often have excessive relaxation or weakness of that lower esophageal sphincter. That sphincter is supposed to prevent stomach contents from back flowing into the esophagus, but that sphincter is not working correctly, then GERD can occur. Risk factors associated with GERD include obesity, smoking, alcohol use, older age, pregnancy, ascitis, and hiatal hernia, which we're going to talk about after GERD. In terms of signs and symptoms, the patient will exhibit dyspepsia, which is a fancy name for indigestion. In addition, they may complain of throat irritation, a bitter taste. They will have burning pain in their esophagus that will feel better when they're sitting up and be worse when they're laying down, which makes sense, right? If you're sitting upright, then gravity is working for you and those stomach contents are more likely to stay in the stomach. If you're laying down, then it makes it much easier for those stomach contents to back flow into the esophagus. In addition, a chronic cough is common in patients who have GERD. We can diagnose GERD with a number of diagnostic procedures and tests, including an EGD and upper GI series, so that's a barium swallow, as well as esophageal PH monitoring and something called esophageal manometry. This is where we test the function of that lower esophageal sphincter. In terms of treatment, a number of medications can be very effective in the treatment of GERD. This includes antacids, H2-receptor antagonist, PPIs and prokinetic agents. And I have a whole video dedicated to those classes of medications in my pharmacology playlist, so definitely check that out. In terms of surgical interventions, if medications and lifestyle modifications are unsuccessful, the patient can undergo a Nissen fundoplication. And it sounds like fun multiplication, but it's really not fun. It's a pretty invasive surgical procedure where the top of the stomach so the fundus is wrapped around the esophagus. In terms of patient teaching, we want to advise our patient to avoid fatty, fried, and spicy foods. They should avoid citrus foods as well as caffeine. They should try to eat smaller meals, so maybe like five smaller meals as opposed to three large meals. They should remain upright after meals, so that's going to make it less likely for reflux to occur. They should avoid eating right before bedtime. Again, because if they eat and then go to bed, laying down is going to make it more likely that reflex occurs. We want them to avoid tight fitting clothing because if they have like a tight belt on, for example, it will make it harder for the GI contents to work their way through the GI system and make it more likely that they can reflux. They should lose weight if applicable. Quit smoking, if applicable, reduce their alcohol intake and then elevate the head of their bed at home so they can do this with blocks. Or they can get one of the more fancy beds where you can lift the head of the bed, kind of like a hospital bed. The last disorder I want to cover in this video is a hiatal hernia. This is where we have protrusion of the stomach through the diaphragm into the thoracic cavity. So normally, we have our thoracic cavity, our diaphragm, our abdominal cavity below that. There's a hole in the diaphragm to allow the esophagus to go through it. That's called a hiatus. And with this disorder, a portion of the stomach comes through that opening, the hiatus, and it can cause a number of symptoms. It can also become caught and become strangulated. And if this occurs, this blocks blood flow to this organ and can result in necrosis. So signs and symptoms of a hiatal hernia include heartburn, dysphagia and chest pain after meals. Diagnosis can be done with a barium swallow study as well as an EGD. Treatment includes the same GERD medications that we previously talked about, so antacids, PPIs, prokinetic agents, etc. And then the surgery is the same, too. If the patient is requiring a surgical intervention, if meds and lifestyle changes are unsuccessful, a fundoplication surgery would be indicated. Again, that's where the top of the stomach, the fundus is wrapped around the esophagus. And then in terms of patient teaching, we're going to teach the patient all the same things as we did with GERD. So we want to avoid spicy, fatty foods when avoid caffeine and citrus, eat smaller meals, remain upright after meals, etc. Med-Surg - Gastrointestinal System, part 5: Gastritis and Peptic Ulcer Disease First up, we have gastritis, which is inflammation of the gastric mucosa. So any time you see itis, that means inflammation. So with gastritis, we have inflammation of that gastric mucosa. Risk factors with gastritis include H. pylori, which is a bacteria that can not only cause gastritis, it can result in peptic ulcer disease, which we're going to talk about next. Other risk factors include long term NSAID use, smoking, stress, as well as heavy alcohol use. Signs and symptoms can include dyspepsia, which is a fancy name for heartburn or indigestion. Other symptoms include nausea and vomiting, stomach pain, bloating, and lack of appetite. In addition, if gastritis gets really bad, it can lead to the formation of ulcers which can bleed, which in turn can cause anemia. In terms of labs and diagnostic tools that we can use in the diagnosis of gastritis, we can use an EGD, and obtain a biopsy during that EGD. We can also use an upper GI series. We may perform a fecal occult blood test. So this is going to test for the presence of blood in the patient's stool, which may be present if the patient has an ulcer. In addition, we could do a urea breath test to test for the presence of H. pylori, that bacteria that can cause gastritis, as well as peptic ulcer disease. In terms of treatment, we want to advise the patient to make some lifestyle modifications and avoid alcohol, quit smoking, and reduce stress if possible. Medications that can be helpful include PPIs, H2 antagonist, as well as antacids. And then if the patient has an H. pylori infection, they will require antibiotics as well. Next, let's talk about peptic ulcer disease, or PUD, which is a disorder that you will need to know inside and out for nursing school. And then if you work on a med surg floor after school, you will see this condition a lot. So with peptic ulcer disease, we have an erosion in the mucosa of the stomach, esophagus, or the duodenum, which is the first part of that small intestine. A key risk factor for peptic ulcer disease is an H. pylori infection. Other risk factors include chronic NSAID use, as well as the use of corticosteroids. Signs and symptoms of PUD can include epigastric pain, so that's going to be pain in the upper abdomen. In addition, the patient may have nausea and vomiting, bloating, hematemesis, which means they'll have bloody vomit or bloody emesis. So if the patient's emesis looks like coffee grounds, so coffee grounds emesis, that is indicative that there may be blood in that vomit. In addition, the patient may have melena, which is a term for bloody stools. In terms of the pain that the patient will experience with PUD, the pain will vary a little bit, depending on whether the patient has a gastric ulcer or a duodenal ulcer. If the patient has a gastric ulcer, they will have pain about 15 to 30 minutes after consuming a meal. The pain will be worse during the day, and it will be worse with eating. This is differentiated from a duodenal ulcer, where the patient will have pain about two to three hours after a meal, so a little longer, and their pain will be worse at night, and it will actually feel a little better with eating. The gold standard for diagnosing peptic ulcer disease is using an EGD, or esophagogastroduodenoscopy. In terms of treatment, if the patient has an H. pylori infection, they are going to be required to take multiple antibiotics over a prolonged amount of time in order to prevent antibiotic resistance. Other medications that can be used include H2 blockers, PPI's, antacids, as well as sucralfate. And if you're not familiar with any of those medications, definitely check out my pharmacology video playlist because I have a video that is devoted to providing details of all of those medication classes. In terms of patient teaching, we want to advise our patient to avoid NSAIDs, caffeine, smoking, and alcohol. Complications of PUD can include hypovolemic shock. So if the patient's ulcer is bleeding extensively, that can cause hypovolemic shock. Signs and symptoms include hypotension, tachycardia, tachypnea, as well as decreased urine output. Treatment of hypovolemic shock will include the administration of blood products, as well as IV fluids. Another complication of PUD is perforation. So with the ulcer, if it erodes through the entire mucosa, we can end up with contamination of the peritoneal cavity with gastric contents. And this will cause signs and symptoms such as severe pain, fever, and a rigid, board-like abdomen, which means the patient likely has peritonitis, which is inflammation of that peritoneal cavity. So treatment of perforation and that peritonitis is with emergency surgery. So the surgeon will have to open the patient all the way up and do a wash out of the abdomen. So a peritoneal lavage. And then in all likelihood, the patient will need a wound VAC, and if they're at my hospital, then I will be the one taking care of their abdominal wound VAC. Med-Surg - Gastrointestinal System, part 6: Irritable Bowel Syndrome, Abdominal Hernia First up, we have irritable bowel syndrome, or IBS, which is an intestinal disorder that causes abdominal pain and changes in bowel movements in the absence of other disorders. So the pathophysiology behind IBS is unknown, but risk factors can include stress, mental health disorders, intestinal bacterial overgrowth, as well as food sensitivities. Signs and symptoms can include abdominal pain, diarrhea, constipation, or a combination of both diarrhea and constipation. And then patients often report improvement in symptoms upon defecation. So in terms of diagnosis, we usually ask the patient to keep a food symptom journal in order to identify triggers of their symptoms. So foods that sometimes trigger these symptoms include milk, alcohol, caffeine, wheat, or eggs. In addition, we would need to do diagnostic testing to rule out other disorders, so this would include blood test and stool tests. In terms of treatment, two key medications that would be used in the treatment of IBS include Alosetron, which is used for IBS with diarrhea, and Lubiprostone, which is used for IBS with constipation. In terms of patient teaching, in addition to keeping that symptom food journal, we want the patient to increase their fiber intake, increase their physical activity, avoid gluten, and reduce stress if possible. Next, we have an abdominal hernia, which is where a section of the intestine protrudes through weakness in the abdominal wall, so you can have a biblical hernia, which happens over the belly button, or an inguinal hernia, which happens around the groin area. So the pathophysiology behind this disorder is that we have muscle weakness and/or increased inter-abdominal pressure that allows for that herniation. So when I was pregnant with my second child, I ended up within a biblical hernia. So before getting pregnant, I had a laparoscopic surgery in my abdomen, and they closed my abdomen up. But by opening and closing my abdomen, it created a weakness in my abdominal wall. Then when I got pregnant, that obviously caused increased intra-abdominal pressure, and that's how I ended up with that umbilical hernia. So when that portion of the intestine protrudes through the abdominal wall, it can get caught and strangulated. And that, in turn, can cause obstruction of the bowel and bowel necrosis. So it can be very dangerous. In terms of risk factors associated with an abdominal hernia, those include obesity, pregnancy, which was my issue, as well as lifting of heavy objects. In terms of signs and symptoms, those include a lump or protrusion at the affected site. So when I was pregnant, I had this huge belly button that was sticking out, and I thought, "Oh, I guess I have an outie belly button while I'm pregnant." But no, it turned out it was a hernia. In addition, if we end up with strangulation of that bowel, that can cause severe pain and decreased bowel sounds, when we have that strangulation or obstruction. In terms of treatment, the patient can be given what's called a truss, which is like a belt that holds the protruding tissue in place. We can also do a surgical repair of the hernia, which is what I had after I gave birth. And then if we end up with strangulation of the bowel, that may require a bowel resection, so removal of part of the bowel. In terms of patient teaching following a hernia repair, we want to advise the patient to avoid coughing. And if they need to cough or sneeze, they should splint the area. In addition, they should avoid heavy lifting and straining. Med-Surg - Gastrointestinal System, part 7: Intestinal Obstruction, Ostomies First, let's talk about an intestinal obstruction, which is something I see a lot of at the hospital as a wound care nurse. So with an intestinal obstruction, we have the complete or partial blockage of the intestines, and this is a potentially life-threatening situation. So with an intestinal obstruction, we can have a mechanical obstruction, which means the bowel is physically blocked by a tumor, a fecal impaction or adhesions from surgery. Or we can have a non-mechanical obstruction, which is a paralytic ileus, which is caused by a neuromuscular disorder that results in decreased or absent peristalsis. Risk factors for a paralytic ileus include abdominal surgery, electrolyte imbalances, abdominal infections, as well as decreased blood supply to the intestines. Signs and symptoms of an intestinal obstruction include abdominal distension and pain, constipation, possible nausea and vomiting, and absent bowel sounds distal to the obstruction. If the patient has a small bowel obstruction, that causes profuse vomiting and severe fluid and electrolyte imbalances, it can also cause metabolic alkalosis. If the patient has a large bowel obstruction, that typically doesn't cause much vomiting and usually doesn't result in severe electrolyte imbalances, either. In terms of diagnosis, we would use an abdominal CT with contrast to diagnose an intestinal obstruction. If a patient has an obstruction, we are going to place them on NPO. We're going to place an NG tube to help decompress the stomach, and then we're going to administer fluids and electrolytes as ordered. In terms of surgical interventions, the patient may require a colon resection, which is removal of part of the colon, and they may also need a colostomy, which we're going to talk more about here in just a minute. In terms of nursing care, we're going to maintain strict I's & O's, and then monitor the patient's electrolyte levels and their acid-base balance. Let's now talk about an ostomy, which is a surgical procedure that reroutes part of the intestine through the abdominal wall, forming a stoma. So an ileostomy is created from the ilium, which is part of the small intestine, and output from an ileostomy will be loose and watery. A colostomy is formed from the large intestine, and the output from the colostomy will vary depending on what type of colostomy the patient has. If the patient has an ascending colostomy, that will be more liquid. If they have a descending or sigmoid colostomy, then their stool output will be more formed. And the reason for this is that the colon, one of its key jobs is to absorb water. So if we're creating an ostomy off of the small intestine, then, there is no chance for the large intestine to absorb that water. And that's why that output is going to be very liquid. If we still have stool going through most of the colon and the ostomy is created out of the descending or sigmoid colon, then the colon had the chance to absorb a lot of that water before we have that output. And that's why it's more formed when we have a descending or sigmoid colostomy. A patient with a new ostomy requires a great deal of education and support. So if you have a patient with a new ostomy, make sure the provider has submitted an order for a wound ostomy nurse to come and help provide some of that teaching. However, you can't rely on the wound ostomy nurse to provide all of that teaching. You need to provide education as well. So one thing you want to tell your patient to do is to assess their stoma regularly. It should be pink or red, and it should be moist. It should not appear pale or blue, which would indicate the presence of ischemia. If you notice that, that's something you're going to want to alert the provider about right away. You also want to advise your patient to empty their ostomy bag when it is one-third to one-half full. And if there is any leaking, then the whole appliance needs to be changed right away, particularly with ileostomies, because the output from an ileostomy has all of those digestive-type enzymes from the small intestine. And if that stool output sits there on the patient's skin, it will eat away at the patient's skin and cause a great deal of pain and problems. So if you notice that there's any leaking of the ostomy, you need to change the whole thing out and not put a washcloth on there or just tape things on, tape it down. You got to change the whole thing. When you are changing the appliance, you want to make sure you cut the opening in the barrier - or the wafer, is what it's called sometimes - no more than one-eighth of an inch bigger than the stoma because again, we don't want any stool output on the patient's skin. So the opening needs to be bigger than the stoma, but just barely. So under one-eighth of an inch. In addition, you want to advise your patient to chew their food thoroughly. They should consume a low fiber diet for the first six to eight weeks after they get their ostomy and then avoid foods that cause gas or odor. Med-Surg - Gastrointestinal System, part 8: Appendicitis and Peritonitis So with appendicitis, that means inflammation of the appendix. With peritonitis, that's inflammation of the peritoneum. So appendicitis is caused when the opening of the appendix becomes obstructed by something like a fecalith, which is a hard, stony mass of feces or a tumor or due to some kind of infection. This causes inflammation of the appendix. It also causes ischemia, so impaired blood flow to the appendix, and that results in bacterial overgrowth. So in terms of signs and symptoms, the hallmark symptom of appendicitis is right lower quadrant pain at McBurney's point. So if your patient is having pain in that quadrant, then you would definitely be suspicious that appendicitis is present. In addition, the patient will have rebound tenderness in that area, meaning that when you push down, it may not hurt so much. But when you let go, when that skin is rebounding, that's when the patient will have more pain. Other signs and symptoms include loss of appetite, nausea and vomiting, as well as fever. We would diagnose the patient with appendicitis using a CT scan. In addition, their labs may show elevated white blood cells. In terms of treatment for a patient with appendicitis, they will be placed on NPO. We will provide IV fluids and antibiotics. And then in terms of surgery, we're going to do an appendectomy, which is removal of the appendix. Typically, we can do this through a laparoscopic approach. But if the appendix has ruptured, then they may require an open appendectomy, where we open up the whole abdomen. In terms of complications, peritonitis and perforation are two possible complications if the appendix ruptures. So if your patient is having pain with their appendicitis and they suddenly say, "Wow, all that pain just went away," then that is actually a red flag and may mean that their appendix has ruptured. Next, let's talk about peritonitis, which is inflammation of the peritoneum, which is that serous membrane that surrounds the abdominal organs. So with peritonitis, we have contamination of the peritoneal cavity with bacteria, and this leads to inflammation. Things that can cause the peritoneal cavity to become contaminated include trauma, infection, as well as perforation of an organ, such as perforation of the appendix, of diverticulitis, or of peptic ulcers. So signs and symptoms of peritonitis include a rigid board-like abdomen. That is a key symptom of this condition. Other signs and symptoms include abdominal pain, nausea and vomiting, fever, rebound tenderness, as well as tachycardia. Diagnosis of peritonitis can be done using an abdominal x-ray, CT, or ultrasound. In terms of treatment, a patient with peritonitis will be placed on NPO, and we will place an NG tube to decompress the stomach and then provide IV fluids, antibiotics, and analgesics. If the cause of the peritonitis was due to a ruptured organ, then the patient will need to undergo surgery to repair or remove that organ. And then they will also need an intra-abdominal lavage, which means we're going to be opening them all the way up and washing out that whole peritoneal cavity due to that contamination. And then we need to closely monitor our patient for signs and symptoms of sepsis because this is definitely a key complication that can happen with peritonitis. Med-Surg - Gastrointestinal System, part 9: Ulcerative Colitis, Crohn's Disease, Diverticulitis Let's first talk about ulcerative colitis, which is a chronic inflammatory disorder of the colon, and it is caused by immune system dysfunction that results in inflammation of the mucosa of the colon and the formation of continuous ulcerations. So this is differentiated from Crohn's disease, where you have patchy or sporadic ulcerations. With ulcerative colitis, those ulcerations are going to be continuous throughout the colon. And just like other autoimmune disorders, patients with ulcerative colitis will have periods of exacerbations as well as remissions. In terms of signs and symptoms of this disorder, these include diarrhea with blood or pus. So the patient will have 10 to 20 liquid stools per day. In addition, they will have fever, abdominal pain, fecal urgency, weight loss, weakness, as well as possible anemia and dehydration, which makes sense, right? If we are having diarrhea 10 to 20 times a day, then we are losing a lot of fluid, which is what's causing the dehydration. In addition, we are losing electrolytes, in all likelihood, so we can end up with electrolyte abnormalities such as hypokalemia. And then if we've got blood in the stool, in the diarrhea, then we are losing red blood cells as well, which is why we may have anemia with ulcerative colitis. So in terms of other labs that will be abnormal, we will see an increase in white blood cells, and we will also see an increase in ESR and CRP. So ESR is erythrocyte sedimentation rate and CRP is C-reactive protein, and those two labs are elevated when we have chronic inflammation like we have with ulcerative colitis. Diagnosis of ulcerative colitis can be done through a colonoscopy, where we collect biopsies. In terms of medications that are helpful in the treatment of ulcerative colitis, we can use sulfasalazine, which is a GI anti-inflammatory medication. We can also use corticosteroids such as prednisone, which has an anti-inflammatory and immunosuppressant-type action. Other immunosuppressants are helpful, such as cyclosporine, and then antidiarrheals can be used as well. In terms of surgical interventions, if the patient's ulcerative colitis is very severe, they may require a proctocolectomy with an ileostomy. So a proctocolectomy means that we are removing the entire colon and rectum. And then in terms of nursing care, we're going to want to closely monitor our patient's Is and Os and their electrolyte levels because of the risk for electrolyte imbalances, such as hypokalemia. We're also going to want to monitor their CBC levels because of the risk of blood loss with this disorder. And then for patient teaching, they should be NPO during exacerbations. Ongoing, we want the patient to consume a high-calorie diet and a low fiber diet. So low fiber because we want the GI contents to slow down as they go through the GI tract. In addition, we should advise our patient to avoid caffeine, alcohol, and lactose because those things can make the diarrhea worse. And then we should encourage the patient to eat smaller, more frequent meals as opposed to bigger meals three times a day. So scattering the meals and making them smaller can help. Now let's talk about Crohn's disease, which is another chronic inflammatory disorder of the GI tract. Like ulcerative colitis, it is an autoimmune disorder that is characterized by periods of exacerbations and remission. However, there are some key differences between these disorders. First of all, with Crohn's disease, the entire GI tract can be involved. This is different than with ulcerative colitis, which just affects the colon. In addition, with Crohn's disease, we have the formation of patchy ulcerations or skip lesions. So these ulcerations will be sporadic in the GI tract, as opposed to ulcerative colitis, which had continuous lesions throughout the colon. In addition, these ulcerations with Crohn's disease can affect all layers of the bowel wall, and then in turn, this can cause the formation of fistulas. So a fistula is an abnormal tunnel between two organs that should not be there. So examples of tunnels that can or fistulas that can form with Crohn's disease include a fistula between one part of the intestine and the other, or between the intestine and the bladder, or the intestine and the vagina. And you can only imagine what complications we would have if we have stool going from the intestine into the vagina or bladder. So fistulas are a key risk when we're talking about Crohn's disease. Signs and symptoms of Crohn's disease include diarrhea. So five to six loose stools per day. Patients with Crohn's disease often have steatorrhea, which means we have a high fat content in the stool. They may have right lower quadrant pain, as well as weight loss, anemia, fever, and fatigue. Abnormal labs that may be present with Crohn's disease include an elevation in white blood cells as well as elevated ESR and CRP, which indicate the presence of inflammation. Diagnosis includes the use of endoscopy. So this can include a colonoscopy and an EGD. In terms of medications that are helpful, the same medications we used with ulcerative colitis are also helpful here with Crohn's disease. So that includes sulfasalazine, which is a GI antiinflammatory medication, immunosuppressants, as well as anti-diarrheal agents. And then surgical interventions that may be required include a small bowel resection or a colectomy and an ileostomy. In terms of nursing care, we're going to want to monitor our patient's Is and Os, their electrolyte levels and CBC levels, and we're going to want to monitor for complications, which include fistulas, malnutrition, as well as an intestinal obstruction. And then a lot of the same patient teaching applies here with Crohn's disease that we had with ulcerative colitis. So during acute exacerbations, we want our patient to be NPO. If they have a very severe exacerbation, they may require TPN. Ongoing, we want them to consume a high-calorie, low-fiber diet, and we want them to eat smaller, more frequent meals ongoing as well. Now let's talk about diverticulitis. So with diverticulosis, we have the formation of these pouches off of the intestine, and these pouches form due to high intraluminal pressure, which can be caused by obesity, low-fiber diet, as well as genetic factors. If we have the accumulation of undigested food and bacteria in these pouches, it can cause those diverticula to get inflamed, which leads to diverticulitis. So signs and symptoms of diverticulitis include left lower quadrant abdominal pain. And the reason why we have this pain in the left lower quadrant is that diverticulitis primarily affects the descending or sigmoid colon, and that's where that is located. In addition, the patient may have bloating, fever, or nausea and vomiting. In terms of abnormal labs, we may see an elevation in white blood cells as well as ESR because of the inflammation. In addition, if there is bleeding associated with the diverticulitis, we may have a decrease in blood levels. In terms of diagnosis, we can use a barium enema, colonoscopy, CT, as well as a lower GI series to help diagnose this condition. Treatment includes antibiotics as well as analgesics. And then in terms of nursing care, we're going to want to monitor for complications, which can include perforation of the diverticula. So that is something I see a lot at my hospital as a wound care nurse. So I help with the wound vac treatment for patients who have GI conditions such as perforated diverticulitis. Other complications include peritonitis, bleeding, as well as the possible formation of fistulas. In terms of patient teaching, we want them to be NPO or consume a clear liquid diet during exacerbations and then progress to a low-fiber diet, but ongoing, we want them to have a high-fiber diet. Med-Surg - Gastrointestinal System, part 10: Pancreatitis Pancreatitis is inflammation of the pancreas. So any time you see -itis, that means inflammation, so inflammation of the pancreas. So normally, the pancreas sends inactivated enzymes to the small intestine, where they become activated and they help to digest fat, protein, and carbs. With pancreatitis, those enzymes become prematurely activated, such that they end up auto-digesting the pancreas, and that results in fibrosis of the pancreas. So risk factors associated with pancreatitis include alcohol abuse, which is a really important key factor. Other risk factors can include bile tract disease, GI surgery, gallstones, trauma, as well as medication toxicity. Signs and symptoms can include severe, left upper quadrant, or epigastric pain, and there will be possible radiation of this pain to the left shoulder or back. In addition, the patient will have nausea and vomiting, and they'll have something called Cullen's sign, which is where we have blue-grey discoloration around the umbilicus or the belly button. So I was trying to think of a good way to help you guys remember Cullen's sign. One of my viewers said, "Hey, Edward Cullen from Twilight has kind of a blue-grey discoloration to his complexion." And so I have to admit I've not seen Twilight, but I did Google Edward Cullen, and he does kind of have a pale complexion, might be a little blue or grey in discoloration. If that helps you to remember Cullen's sign, then I am all for that. The other sign that may be present is Turner's sign, so we do have a cool chicken hint here for Turner Sign. So if you turn your patient over on their side, you will see Turner's sign, which is ecchymosis that will show up on the patient's flank. Other signs and symptoms include jaundice as well as tetani, which is associated with hypocalcemia that we often see with pancreatitis. Abnormal labs that are associated with pancreatitis are very important to know. Labs that may be elevated include amylase, lipase, white blood cells, bilirubin, as well as glucose. So why is glucose elevated? Well, the pancreas normally makes insulin. So if the pancreas is messed up and not making enough insulin, then that glucose is not getting from the bloodstream into the body's cells, and it's accumulating in the bloodstream. Lab values that may be decreased include calcium, magnesium, and platelets. So in terms of diagnosis, we can use an ultrasound, CT scan, or MRI to help diagnose pancreatitis. For patient with pancreatitis, we're going to place them on NPO and then gradually have them consume a bland and low-fat diet over time. In addition, we're going to provide IV fluids and electrolytes. We're going to provide opioid analgesics because pancreatitis is associated with severe pain. In addition, we need to provide antibiotics, antiemetics for nausea and vomiting, insulin so that we can get that glucose into the body's cells, and then pancreatic enzymes with all meals and snacks. Because again, the pancreas is messed up, so it's not doing its normal job, which includes bringing those digestive enzymes over to the small intestine to help with digestion. In terms of nursing care, we're going to want to monitor for complications, which can include chronic pancreatitis, which is something we see often with alcohol abuse. Other complications include a pancreatic pseudocyst. So this is where we have these fluid-filled sacs that form kind of in or around the pancreas. And then type 1 diabetes is also a complication of chronic pancreatitis. In terms of patient teaching, we want to definitely emphasize that the patient should not consume alcohol. And if appropriate, we should refer the patient to an alcohol recovery program. And then we should encourage the patient to consume a low-fat diet, ongoing, and no smoking. Med-Surg - Gastrointestinal System, part 11: Cirrhosis, Paracentesis, Esophageal Varices With cirrhosis, we have inflammation of the liver that causes the destruction and the replacement of the hepatocytes, which are those liver cells, with scar tissue. The three main causes and types of cirrhosis include postnecrotic cirrhosis, which is caused by viral hepatitis or toxins or drugs. Then we have biliary cirrhosis, which is also called biliary cholangitis. This is where we have damage to the bile ducts, and that causes bile to back up into the liver, which damages those hepatocytes. And then finally, we have Laennec's cirrhosis, which is caused by chronic alcoholism. Early signs of cirrhosis include fatigue, hepatomegaly, which is enlargement of the liver, nausea and vomiting, as well as abdominal pain. As cirrhosis progresses, we end up with many signs and symptoms because the liver is responsible for a lot of different functions in the body. So some of those late signs and symptoms include bleeding and bruising, partially because the liver is responsible for making some clotting factors and those are needed for hemostasis. So if we don't have those clotting factors, we're going to end up with more bleeding. Patients with cirrhosis will also have jaundice, which is yellow discoloration of the skin, as well as like the whites of the eye. Patients will also have ascites, which is the buildup of fluid in the abdomen, as well as esophageal varices, which are fragile, swollen blood vessels in the esophagus. Patients will also end up with portal hypertension, which is increased pressure in the portal vein, which carries blood from the digestive organs into the liver. In addition, the patient may have peripheral edema, as well as something called Fetor Hepaticus. So this means they have a foul, musty breath odor. Other symptoms include hepatic encephalopathy. So with cirrhosis, we have a buildup of ammonia in the body, and that ammonia could also build up in the brain, which causes confusion. So that is hepatic encephalopathy. In addition, the patient may have pruritus, which is like itching; Petechiae, which are those red dots that show up on the skin, as well as spider angiomas; Palmar Erythema so red palms; dark urine; and clay colored stools. Labs that will be elevated with cirrhosis include increased ALT, AST, bilirubin, as well as ammonia. Labs that will be decreased include decreased serum protein and albumin. So albumin is a really important protein that we find in the bloodstream, and it helps to keep fluid in the intravascular space in those blood vessels. If we don't have enough albumin, which we don't with cirrhosis because the liver isn't functioning properly so it's not making enough albumin, then that fluid will leave the bloodstream and go to the extra vascular space. The gold standard for diagnosing cirrhosis is using a liver biopsy. Other diagnostic tools that can be helpful include ultrasound, CT, and MRI. There is no cure for cirrhosis. Medications that may be prescribed include vitamin and mineral supplements, as well as diuretics to get rid of that excess fluid, and lactulose, which is a laxative that helps to bring down ammonia levels. And it will also cause the patient to poop a lot because it's a laxative. Procedures include a paracentesis, which helps to remove that excess fluid from the abdomen, and we're going to talk more about that in just a minute. A liver transplant may be an option as well for the patient. In terms of nursing care, we're going to want to monitor our patients' eyes and nose, restrict fluids and sodium as ordered, measure the patient's abdominal girth daily, and then monitor for complications, which can include encephalopathy, portal hypertension, esophageal varices, as well as hemorrhage. In terms of patient teaching, you want to advise your patient to consume a low sodium diet, eat small, frequent meals, and if the patient has an alcohol abuse issue, then you definitely want to encourage an alcohol recovery program. Next, let's talk about a paracentesis, which is a procedure where we insert a needle through the patient's abdominal wall and remove fluid from that peritoneal cavity. So if the patient has ascites related to their cirrhosis, which is causing respiratory distress, then this procedure can help bring some relief. In terms of nursing care before the procedure, you want to make sure informed consent was received, and you also want the patient to empty their bladder. So if we're poking in their abdomen, we do not want to accidentally perforate their bladder, which is why we have them empty their bladder. In addition, we're going to take the patient's vital signs. We're going to measure their weight and measure their abdominal girth. After the procedure, we're going to measure those same things. So vital signs, weight, and abdominal girth. We're also going to be on the lookout for hypovolemia because that peritoneal fluid that we removed is high in protein, which can cause a fluid shift. In addition, if the provider has prescribed albumin, we will administer that to the patient as well. The last thing I want to cover in this video are esophageal varices, which I mentioned briefly when I was talking about cirrhosis. So esophageal varices are swollen, fragile blood vessels in the esophagus that can hemorrhage, which is life threatening. So the key risk factor for esophageal varices is portal hypertension. So that portal vein carries blood from the digestive organs into the liver. When the liver is scarred like it is with cirrhosis, then blood flow is impaired into that liver. And that causes increased pressure in that portal vein and causes blood to back up or be shunted into the surrounding blood vessels. So if we have bleeding associated with these esophageal varices, the patient may have symptoms such as hypotension and tachycardia. There are some medications and procedures that can be used to help prevent that bleeding and address those esophageal varices. So medications that can be used include basal constrictors, as well as non-selective beta blockers. And examples of procedures that could be used include endoscopic sclera therapy as well as band ligation. Med-Surg - Gastrointestinal System, part 12: Hepatitis, Cholecystitis, Bariatric Surgery Hepatitis is inflammation of the liver that is caused by a virus or a hepatotoxic medication or chemical. Let's first talk about the different types of viral hepatitis. So we have hepatitis A, B, C, D, and E. Hepatitis A and E are spread through the fecal-oral route; for example, contaminated water. Hepatitis B, C, and D are spread through blood and bodily fluids. We have vaccines for hepatitis A and B. There is no vaccine for hepatitis C. And of note, you can only get hepatitis D if you have hepatitis B. So if you get your vaccine to hepatitis B, then you won't get hepatitis D. So if a patient has chronic hepatitis, that can lead to cirrhosis or liver cancer. Risk factors for viral hepatitis include IV drug use, body piercings, tattoos, high-risk sexual practices, as well as travel to underdeveloped countries. Signs and symptoms can include fever, lethargy, nausea and vomiting, jaundice, which is yellow discoloration of the skin and of the whites of the eyes. In addition, the patient may have clay-colored stools, dark urine, abdominal pain, as well as arthralgia, which is joint pain. Abnormal labs that may be present with hepatitis include an increase in ALT, AST, as well as bilirubin, and then diagnosis of viral hepatitis can be done with serological testing, which tests for the presence of antibodies for the different types of viral hepatitis. And then, in terms of treatment, with hepatitis A and E, those types are usually self-resolving and don't really require much treatment, other than supportive care. We can use antiviral agents for chronic hepatitis B or acute or chronic hepatitis C. Next, let's talk about cholecystitis, which is inflammation of the gallbladder, and this is typically caused by cholelithiasis, which is a gallstone. So that gallstone will block the cystic duct or the common bile duct and cause inflammation of the gallbladder, impaired bile flow, and eventual necrosis of the cells in the gallbladder. So risk factors associated with cholecystitis include cholelithiasis, as I just described. Other risk factors include a high-fat diet, obesity, genetics, older age, and the female gender. In terms of signs and symptoms, the patient will likely have right-upper-quadrant pain that may radiate to the right shoulder. They will have pain upon ingestion of high-fat foods. They may also complain of nausea and vomiting, dyspepsia, which is a fancy name for indigestion, as well as gas and bloating. And if the liver becomes involved - for example, if the gallstone is in that common bile duct - then we may end up with symptoms such as jaundice, dark-colored urine, and clay-colored stools because of that liver involvement. White blood cells are often elevated with cholelithiasis. If we have liver involvement, then liver enzymes such as AST and bilirubin may be elevated. And if we have pancreatic involvement because that pancreatic duct will join with the common bile duct before it reaches the small intestine, then we may have elevation in amylase and light pace. In terms of diagnosing cholecystitis, we would use an ultrasound. Treatment includes the use of analgesics. We can also do a lithotripsy, which uses shockwaves to break up those gallstones. The patient may ultimately require a cholecystectomy, which is removal of that gallbladder. In terms of nursing care, we're going to want to monitor for complications, which can include pancreatitis if the pancreas becomes involved. It can also include peritonitis, which can be caused by perforation of the gallbladder. So if the gallbladder perforates, then all of those contents are going to contaminate the abdominal cavity, that peritoneal cavity, which can result in peritonitis. In terms of patient teaching, we want to advise our patient to consume a low-fat diet, they should avoid gas-causing foods, and they should lose weight, if applicable. The last topic I'm going to cover in this video and in this gastrointestinal playlist is bariatric surgery. So this is a surgical intervention aimed at reducing an individual's gastric capacity or absorption, and we perform this in morbidly obese patients, so typically with a BMI over 40 or with a BMI over 35 with other risk factors. So in terms of post-op nursing care, we're going to want to monitor the patient for dumping syndrome. Signs and symptoms of dumping syndrome include abdominal cramping, tachycardia, nausea, diarrhea, as well as diaphoresis. We also need to provide some important teaching to our patient who just had bariatric surgery. So we need to advise them to chew their food slowly and thoroughly. We need to advise them to eat six small meals a day versus three large meals. They should not consume liquids with meals. They will need to have liquids between meals. They should recline after meals in order to slow gastric emptying and prevent dumping syndrome. And then they should avoid foods that are high in sugar, fat, and carbohydrates. All right, it's time for a quiz. I have four questions for you. First question. What types of hepatitis are preventable through vaccination? The answer is hepatitis A and B. Question number two. What procedure uses shockwaves to break up gallstones? The answer is lithotripsy. Question number three. What type of diet would be recommended for a patient with cholecystitis? The answer is a low-fat diet. Question number four. What complication of bariatric surgery is characterized by abdominal cramping, tachycardia, diaphoresis, and diarrhea? The answer is dumping syndrome. All right. That is it for this video and for this gastrointestinal playlist. I hope you have found it super helpful. Take care, and good luck with studying. Hepatitis is inflammation of the liver that can be caused due to-- hepatitis is inflammation of the liver that can be caused to-- that can be caused due to exposure to a virus or due to a. Med-Surg Endocrine System, part 1: Introduction & Key functions So let's first talk about the overall function of the endocrine system, which is the release of hormones. So hormones are like chemical messengers. So these hormones are released from organs and glands in the body, and we'll go over all of those. And they allow for many different functions in the body. This includes growth and development, metabolism, reproduction, electrolyte and acid-base balance, as well as the body's response to infection, illness, and stress. So the endocrine system has a lot of control over the body. If a particular gland or organ releases too many hormones, right - we have too much - that can cause a disorder. And if an organ or gland releases too little of that hormone, then we can also end up with a disorder as well. So a lot of the disorders and diseases we'll talk about are because of too much or too little of those hormones. Med-Surg Endocrine System, part 2: Organs, glands & hormone overview Starting with the hypothalamus, the hypothalamus is located in the brain and it produces four key hormones that I'd be familiar with. One is corticotropin-releasing hormone. Then we have thyroid-releasing hormone, growth hormone-releasing hormone, and gonadotropin-releasing hormone. You notice that all four of these end in that releasing hormone. And then if you look at the first letter of each of these hormones, we have C, T, G, G. and my little mnemonic I use to help me recall these hormones is Cutthroat good game. That was a Cutthroat game, but good game anyway, and that's just my silly way to remember these hormones. Then, moving on to the pituitary gland. The pituitary gland is also located in the brain. Some hormones are released from the anterior pituitary gland and some hormones are released from the posterior pituitary gland. The hormones released from the anterior pituitary gland include thyroid-stimulating hormone, prolactin, follicle-stimulating hormone, luteinizing hormone, adrenocorticotropic hormone, and growth hormone. And then the two key hormones released from the posterior pituitary gland include ADH, which is anti-diuretic hormone, and oxytocin. The way I remember these six key hormones from the anterior pituitary gland is I look at the first letter of each, which is T-P F-L-A-G, which kind of looks like TP FLAG. I think about the anterior pituitary gland surrendering or giving up hormones and flying a white TP flag. That's my little inappropriate potty-humor way of remembering what hormones are released by the anterior pituitary gland. Moving on to the thyroid gland in the neck. The thyroid gland produces T3, which is triiodothyronine; T4, which is thyroxine; and calcitonin. From now on, I'm going to refer to those as T3 and T4, so I don't have to try to pronounce triiodothyronine anymore. Then we are going to move on to the parathyroid glands. So we have four parathyroid glands located right next to the thyroid gland, and they produce parathyroid hormone, or PTH. Then we go down to the adrenal glands. The adrenal glands rest on top of the kidneys. And some hormones are released from the adrenal cortex, which is the outer layer of the adrenal gland, and then some hormones are released from the adrenal medulla, which is the inside of the adrenal gland. So the hormones released by the adrenal cortex include aldosterone, cortisol, and androgens. And then from the adrenal medulla, the hormones produced there include epinephrine and norepinephrine. Then we have the pancreas, which is situated behind the stomach. The pancreas produces insulin and glucagon. The testes is another endocrine gland. It produces testosterone. And then the ovaries produce estrogen and progesterone. Med-Surg Endocrine System, part 3: Cortisol, T3/T4, GH, Estrogen, Progesterone, Testosterone, Oxytocin & Prolactin Let's first talk about cortisol. Cortisol is a glucocorticoid that is considered the stress hormone in the body. It has more to do with chronic stress than it does acute stress. If you're being chased by a bear, that's definitely acute stress, and that would cause the release of epinephrine and norepinephrine from the adrenal medulla. However, if you have more chronic stress, say with nursing school, that can result in elevated cortisol levels. If you have elevated cortisol levels for a long period of time, that can have some detrimental effects on the body. Including decreased immune function, increased blood pressure, and high levels of glucose in the bloodstream. That is one of the effects of cortisol. Cortisol has a number of functions in the body, including regulation of metabolism, your immune response, as well as your body's response to stress. What controls the release of cortisol? It starts in the hypothalamus. So the hypothalamus will produce CRH, which causes the release of ACTH from the anterior pituitary gland. And then this causes the release of cortisol from the adrenal cortex. We will be getting into dysfunctions that are caused by too much cortisol, such as Cushing's disease, or not enough cortisol, such as Addison's disease. So those diseases will be covered in another video in this playlist. Next, let's talk about thyroid hormones, T3 and T4. And also just so you know, T3 is the active form of T4. Thyroid hormones control many functions in the body, including metabolism, growth and development, heart function, brain function, muscle function, as well as digestion and bone maintenance. In terms of what controls release of thyroid hormones, it starts again in the hypothalamus. So the hypothalamus produces TRH, which causes the anterior pituitary gland to produce TSH. And then this allows for production of T3 and T4 in the thyroid gland. We will be getting into dysfunctions of the thyroid hormones as well. If we have too much T3 or T4, we can end up with hyperthyroidism. And if we don't have enough, then we can have hypothyroidism. Next, we have growth hormone, or GH. And another name for growth hormone is somatotropin. Growth hormone controls growth, which is pretty intuitive, and metabolism in the body. And it also controls protein synthesis. In terms of the release of growth hormone, again it starts in the hypothalamus. The hypothalamus will produce GHRH, growth hormone-releasing hormone, and that causes growth hormone, GH, to be produced in the anterior pituitary gland. And we will be going over dysfunctions of growth hormones. So if we have too much growth hormone, that's growth hormone excess. That causes problems. And if we don't have enough, that also causes issues that we will be discussing. Next, let's talk about estrogen. Estrogen is a hormone that stimulates development of female sex organs, and it also is instrumental in the regulation of the menstrual cycle. We're not going to go into details of the menstrual cycle in this playlist. But we will be talking about it more in my reproductive system playlist. In terms of what controls release of estrogen, it starts in the hypothalamus. The hypothalamus first produces gonadotropin-releasing hormone. This causes LH and FSH to be produced in the anterior pituitary gland, and then that allows for production of estrogen in the ovaries. Next we have progesterone. So progesterone also plays a role in the regulation of the menstrual cycle. And it also plays a key role in the maintenance of pregnancy. The pathway, again - you guessed it - it starts in the hypothalamus where the hypothalamus releases gonadotropin-releasing hormone. This causes LH to be released from the anterior pituitary gland, and this allows for progesterone to be produced in the ovaries. Now we had testosterone. Testosterone helps to stimulate the development of male sex organs, and it's also instrumental in sperm production. The pathway - I know you guys are going to get this. Gonadotropin-releasing hormone is produced in the hypothalamus, which causes FSH and LH to be produced in the anterior pituitary gland. And then this allows for sperm and testosterone production in the testes. Next we have oxytocin. So in females, it causes contraction of the uterus and also promotes lactation. In males, it controls production of testosterone as well as sperm release. Most hormones in the endocrine system are controlled through a negative feedback mechanism, which we will be talking about at length in another video. Oxytocin, on the other hand, is controlled by a positive feedback mechanism, which we'll also talk about in that video. So in women, oxytocin is released in response to uterine contractions as well as breastfeeding. Then let's talk about prolactin. Prolactin is a hormone that primarily promotes lactation. So that one is pretty easy to remember, because you have prolactin and lactation. It is released from the anterior pituitary gland. Levels of prolactin in the body are basically controlled by levels of dopamine, estrogen, and other hormones circulating in the body. Med-Surg Endocrine System, part 4: ADH, Aldosterone & RAAS Let's first talk about ADH. ADH helps to control blood pressure and blood volume in the body by regulating the reabsorption or excretion of water in the kidneys. So if we have more ADH, that's going to cause more reabsorption of water. If we have lower levels of ADH, that's going to cause more excretion of water. ADH is secreted from the posterior pituitary gland, in response to three things. One is low blood volume. So if we have hypovolemia, which is not enough blood volume, then more ADH will be produced. That will cause more reabsorption of water, which will help to bring up that blood volume. Also, the second thing is if the body senses that blood pressure is low, it will want to bring that up. And the way it does that is it releases ADH, which causes more reabsorption of water at the kidneys, which helps to increase the blood volume, which will increase blood pressure. And then the third thing the body does if it senses hypernatremia. So if we have concentrated blood, so it's concentrated with sodium, we want to try to dilute it. And in order to do that, we release ADH, causes reabsorption of water, and that will help dilute [the sodium in] the blood and bring those sodium levels back down to normal. So those are the three things that cause the body to release more ADH from the posterior pituitary gland. And ADH is going to be an important hormone to remember. And we will be talking about different conditions and disorders that cause issues with ADH. Okay. Now, let's move to aldosterone. Aldosterone is a hormone that increases blood volume and blood pressure by causing kidney reabsorption of both water and sodium. So unlike with ADH, we were just reabsorbing more water, with aldosterone it's both sodium and water. In addition, aldosterone will cause excretion of potassium. So the release of aldosterone is controlled by the renin-angiotensin-aldosterone system, which I will go through those steps now. So the whole system basically kicks off when there is decreased blood flow to the kidneys, which usually means that there is low blood pressure in the body. So when there's this decreased blood flow to the kidneys, the kidneys release renin. Renin in turn activates angiotensinogen into angiotensin I. Angiotensin I is converted in angiotensin II by ACE, which is angiotensin converting enzyme. And that is produced by the lungs. Then angiotensin II causes a number of actions to take place, all of which increase blood pressure in the body. The first thing that angiotensin II does is that is causes vasoconstriction of the afferent arterioles in the nephrons, in the kidneys, which increases sodium and water reabsorption, okay? The second thing that angiotensin II does is that it causes aldosterone to be released from the adrenal cortex, which, as we talked about, causes the reabsorption of sodium and water at the kidneys, which helps to increase blood pressure and blood volume. Then it also causes vasoconstriction of blood vessels throughout the body. So by constricting those blood vessels, that also helps to bring up that blood pressure. So again, all three of these things that angiotensin II does are all intended to help increase that blood pressure when there is low blood pressure initially. Med-Surg Endocrine System, part 5: Epinephrine, Norepinephrine, Calcitonin, PTH, Insulin & Glucagon Let's first talk about epinephrine and norepinephrine. These two hormones are catecholamines that are released by the adrenal medulla - so that's the inside of the adrenal gland - in response to acute stress. So if you are being chased by a bear, that would be acute stress, and that would kick off your body's flight or fight response and result in the release of epinephrine and norepinephrine. These hormones will cause a number of changes in the body, including vasoconstriction, increase of heart rate and blood pressure, bronchodilation, pupil dilation, increase blood flow to the muscles, and increase blood glucose levels. Your body's basically preparing to run from the bear, and it wants to make sure that you're getting enough oxygen in those lungs and that the blood is circulating throughout the body and getting that oxygen and nutrients to your skeletal muscles and everywhere else. So those are the changes you can expect when epinephrine and norepinephrine are released. Keep in mind that epinephrine has more of an effect on the heart, versus norepinephrine which has more of an effect on the blood vessels. So in terms of what controls release of epinephrine and norepinephrine, when you have an acute stress situation, the sympathetic nervous system is activated, which activates nerves that are connected to that adrenal medulla, which allows for the secretion of epinephrine and norepinephrine. Now let's talk about calcitonin, which is a hormone that decreases blood calcium levels. It opposes the action of parathyroid hormone, which we'll talk about next. So it decreases blood calcium levels by doing two different things. The first thing it does is it decreases the activity of osteoclasts. So osteoclasts are cells that break down the bone and move that calcium into the bloodstream. And we don't want that, right, because we're trying to decrease levels of calcium in the bloodstream. So it opposes the action of osteoclasts. Then the other thing that calcitonin does is it increases excretion of calcium at the kidney. So we're just getting rid of extra calcium so it doesn't build up in the bloodstream. So the way that I remember what calcitonin does is if you look at the word calcitonin, you can remember that calcitonin tones down the calcium. And that little hint is here on card 11 [of the Endocrine System section in the Medical-Surgical Flashcards]. So what stimulates release of calcitonin? When the body senses that we have too much calcium in the bloodstream, or hypercalcemia, this stimulates a release of calcitonin from the thyroid gland. Now, let's talk about parathyroid hormone, or PTH. This basically does the opposite of what calcitonin does. So PTH wants to increase the amount of calcium in the bloodstream, and it does this by doing three different things. The first thing it does is it pulls calcium out of the bones and into the bloodstream. The second thing it does is it causes the kidneys to reabsorb more calcium, and it also causes the kidneys to release vitamin D, which helps with the absorption of calcium in the body. And then the third thing it does is it increases absorption of calcium in the intestines. So it does all of these three things to bring those calcium levels up in the bloodstream. So what controls release of PTH? When the body senses that there's not enough calcium in the bloodstream, so hypocalcemia, that stimulates the release of PTH from the parathyroid gland. Let's talk about insulin and glucagon. Insulin decreases blood glucose levels. Insulin allows glucose to move from the bloodstream into the body's cells, where it can be used for energy. So when the body senses that blood glucose levels are rising, insulin is released from the beta cells in the pancreas to help escort that glucose into the body's cells. Glucagon is basically doing the opposite. It wants to increase blood glucose levels, as opposed to insulin, which wants to decrease blood glucose levels. Glucagon increases blood glucose levels in three different ways. The first way is through glycogenolysis. So this is where we convert glycogen in the liver into glucose and then release that into the bloodstream. The second way that glucagon increases blood glucose levels is through gluconeogenesis, so this is production of new glucose. And then the third way that glucagon increases blood glucose levels is it causes the adipose tissue to break down fat for use as energy. So it does these three things to bring up those blood glucose levels. So when the body senses that blood glucose levels are low, then glucagon is released from the alpha cells in the pancreas. Med-Surg Endocrine System, part 6: Negative Feedback Mechanism vs. Positive Feedback Mechanism So let's first talk about the negative feedback mechanism, which works similarly to your thermostat. If your heater is turned on in your home and your temperature is set at 75, your heater will run until that temperature gets to 75. Then it will turn off. As the temperature lowers when it goes below 75, it will turn back on, and it turns off and on to keep the level right there at 75 degrees. Well the hormones within the endocrine system, it kind of works the same way. If an endocrine gland senses that there is too much of a circulating hormone in the body, it will initiate changes to decrease production of that hormone, and if an endocrine organ or gland senses there's not enough of a circulating hormone, it will initiate changes to increase production of that hormone, to try to keep homeostasis, just the right amount of hormones circulating in the body. Let's now look at a a specific example of that negative feedback mechanism or negative feedback loop. We're going to look at the release of thyroid hormones, which are T3 and T4. Starting off, the hypothalamus produces thyroid-releasing hormone which causes the anterior pituitary gland to produce thyroid-stimulating hormone, and then this causes the thyroid gland to produce T3 and T4. And it releases T3 and T4 into the body, where it goes and does its job. So if the hypothalamus senses that there is too much T3 and T4 out there, it will decrease production of TRH, which will, in turn, cause the anterior pituitary gland to decrease production of TSH, and this will cause the thyroid gland to decrease production of T3, T4. And that is what we mean by a negative feedback mechanism. The anterior pituitary gland also can sense if there's too much T3 and T4 circulating in the body, and if it does sense that, it will, by itself, decrease TSH, which will, in turn, decrease production of T3 and T4 by the thyroid gland. This works kind of the opposite way as well. So if there's not enough T3, T4 circulating in the body, the hypothalamus will increase production of TRH, which will cause the anterior pituitary gland to increase production of TSH, and that will cause an increase in production of T3 and T4 by the thyroid gland. This how we maintain homeostasis for these thyroid hormones. However, if we end up having an issue in the hypothalamus or in the anterior pituitary gland or in the thyroid gland, then that really throws a wrench in everything. So when we are talking about hypothyroidism and hyperthyroidism, we will get into more detail about that. Okay. So that negative feedback loop example that I just explained, that controls the release of most endocrine hormones. However, there are a few hormones that are controlled by a positive feedback mechanism instead. So with a negative feedback mechanism, like we just talked about, if we release a bunch of hormones, the body will sense that, right? The organs and glands will sense that, and they will decrease production of that hormone. That's a negative feedback loop. With a positive feedback mechanism, when we release a bunch of hormone, that causes additional release of that same hormone. So oxytocin is a hormone that is regulated by a positive feedback mechanism. And I'll give you a couple of examples where oxytocin is released and that the release of oxytocin causes additional release of oxytocin. One is during childbirth. So release of oxytocin allows for uterine contractions, and uterine contractions cause additional oxytocin to be released. Also, we see it with breastfeeding. So breastfeeding causes the release of oxytocin, which allows for milk ejection. And this in turn causes an additional release of oxytocin, so it just compounds that. So oxytocin will stop being produced after childbirth or after a mom is done breastfeeding. And that's how production of oxytocin does end up decreasing. Med-Surg Endocrine System, part 7: Thyroid Panel and Blood Glucose Labs Let's start with T3. So T3 should be between 70 and 204, and the way I remember this range is T3 reminds me of times 3. So if you take 70 times 3, that gives you 210, which is kind of the upper end of that range. So if I can remember 70, and if I look at T3, then I know to multiply that times 3 to get 210 as the upper range. So this trick, along with others, is in my Lab Values deck, if you're interested. T4. T4 should be between 4 and 12, and the way I remember this is that my husband is obsessed with Terminator, or at least used to be, and I've probably been forced to watch T4, or Terminator 4, between 4 and 12 times, and that's probably not an exaggeration at all. At least I've watched part of it 4 to 12 times, because I'm usually asleep for a good bit of it, so but yeah, 4 to 12 times, not kidding. So that's how I remember T4. TSH. TSH reminds me of tush, right? So kind of missing the U but it looks like tush. The normal range for TSH is between 0.5 and 5, so it's roughly up to 5. So the way I remember this is if you touch my tush, again, right, my booty, I am going to slap you with all 5 fingers. So that helps me remember that when we're talking about TSH, the normal range is up to 5, 5 fingers. Okay. I hope you're enjoying my silly, little ways to remember these things. Let's talk about blood glucose. If your patient has a fasting blood glucose, we would expect them to have a value under 100. If they have a value over 100 for a fasting blood glucose, then we would be concerned for prediabetes or diabetes. If a patient has a two-hour oral glucose tolerance test, then we would expect a value under 140. And then if they get their HGB A1c level drawn, we would expect that percentage to be under 6, okay? When we talk about diabetes in an upcoming video, if a patient has diabetes, we're going to manage their progress at controlling their blood glucose levels with that HGB A1c value. And if they keep it under 7, then that's usually good enough if the patient is diabetic. But if we're talking about the general population and someone who does not have diabetes or at least not diagnosed diabetes, we would expect that A1c to be under 6. Med-Surg Endocrine System, part 8: Hypo- vs. Hyperpituitarism & Hypophysectomy So let's first talk about hypopituitarism. This is where we have a deficiency of one or more of the pituitary gland hormones that are released. And if you recall, there's a lot of different hormones that are released by the pituitary gland. This includes TSH, prolactin, FSH, LH, ACTH, GH, and then also ADH and oxytocin. So there's a lot of hormones. So when we have a deficiency of one or more of these hormones, that can cause a lot of different problems in the body. In terms of the pathophysiology behind hypopituitarism, in most cases, it's an issue with the pituitary gland. So we have a pituitary tumor, there's some kind of congenital defect, or due to trauma, so trauma causes some damage to the pituitary gland. In some cases, it may be an issue with the hypothalamus. If you remember, the hypothalamus releases hormones that cause the pituitary gland to release hormones, so if the hypothalamus isn't doing its job, then the pituitary gland can't do its job. But in most cases, it's actually an issue with that pituitary gland. So in terms of signs and symptoms of this condition, we're going to get a variety of signs and symptoms depending on which of the hormones is affected. In most cases, the growth hormone is affected. So when a patient has hypopituitarism, we'll often see delayed growth. Also, FSH and LH release is also affected often with this condition. So when we have decreased FSH and LH, we may see signs and symptoms such as amenorrhea in females and impotence in males. And then because we're not doing-- or not releasing as much TSH as we need to, which is thyroid-stimulating hormone, your patient may exhibit signs and symptoms of hypothyroidism, which we'll talk more about in another video. And then, lastly, we may see signs and symptoms of adrenal insufficiency because the pituitary gland is not producing enough ACTH. So signs and symptoms of adrenal insufficiency include fatigue, weakness, weight loss, hypoglycemia, as well as hyponatremia and orthostatic hypotension. So in terms of the labs and how we diagnose this condition, we would obviously take a look at levels of those pituitary hormones, but we also want to take a look at target hormone levels as well. And then, we're going to do something called an ACTH stimulation test. Like we talked about, ACTH is one of the hormones released by the pituitary gland that causes the adrenal gland to release cortisol. Okay? So if we give a patient ACTH, we give then an injection of ACTH, if there's an issue with the pituitary gland and it hasn't been producing that ACTH, it will cause the adrenal glands to be happy. They're finally getting some ACTH and they will produce their cortisol like they're supposed to. However, if we give the patient this ACTH injection and it doesn't cause the adrenal gland to produce any cortisol, then that means there's probably an issue with the adrenal gland as opposed to the pituitary gland. So that's another test we do. And then, we would also do a CT or MRI of the pituitary gland to try to identify any kind of tumor or abnormality in the pituitary gland. In terms of treatment, the patient is going to require hormone replacement therapy. So they may get medications such as corticosteroids as well as thyroid replacement hormones and sex hormones and growth hormones depending on where they have those deficiencies. Alright, now let's talk about hyperpituitarism, which is where we have oversecretion of the pituitary gland hormones. The pathophysiology behind this disorder, it typically starts with a pituitary adenoma, which is a benign tumor in the pituitary gland, or tissue hyperplasia, which is overgrowth of tissue, and either this adenoma or this tissue hyperplasia typically takes place in the anterior pituitary gland, and it compresses the brain tissue and causes increased secretion of growth hormone, prolactin, and ACTH. So in terms of signs and symptoms of this disorder, because we have this compression of brain tissue, this can cause an increase in intercranial pressure, and this can result in symptoms such as a headache and nausea and vomiting. Also, because we have increased secretion of growth hormone, this can result in acromegaly, as well as arthralgia. So arthralgia is just a fancy name for joint pain. And with increased ACTH, this causes increased levels of cortisol, so your patient may have signs and symptoms of Cushing's disease. And we'll definitely be talking about Cushing's disease in more detail in another video. And then those increased levels of prolactin can result in sexual dysfunction as well. So in terms of diagnosis of hyperpituitarism, we're going to do a CT or MRI of the pituitary gland, which will show this adenoma or tissue hyperplasia. And then in terms of treatment options, surgically, we can do a hypophysectomy, which is removal of part or all of the pituitary gland. We typically go through the nasal cavity. So that is a transsphenoidal approach to the hypophysectomy. But sometimes we need to go through the oral cavity, like under the top lip or kind of there at the upper-gum level. Medications that can be used alternatively include a dopamine agonist, which helps to inhibit growth hormone or prolactin secretion. Or we can use somatostatin for acromegaly. Let's now talk about the nursing care and patient teaching following a hypophysectomy. One of the main things we need to monitor for as a nurse following this procedure are for signs and symptoms of a CSF leak, or cerebrospinal fluid leak, in the drainage. So some of the signs and symptoms that may indicate there is a CSF leak include a halo sign in the drainage. So when I say halo sign. I mean that there is clear or bloody drainage in the center of the drainage, but then there is this yellow ring outside of that drainage. If you see that halo sign, that may mean that there is a CSF leak. Other signs that may indicate a CSF leak include if the patient is complaining of a headache or is also indicating that the drainage tastes sweet. And then, if you test the drainage, and it is positive for glucose, that is also a possible sign that there is a CSF leak, and that needs to be further investigated. In terms of patient teaching, we want to definitely teach them to avoid activities that may increase intercranial pressure. So this includes coughing, sneezing, blowing their nose, bending at the waist, and straining during bowel movements. So we are definitely going to be giving them stool softeners and things to help prevent straining during bowel movements. In addition, you need to let your patient know that a decreased sense of smell is expected for about the first month after the procedure. And then it is also recommended, particularly if we did the hypophysectomy through the oral cavity, that they do not brush their teeth for 2 weeks. It is okay for them to floss and rinse their mouth. And then finally, the patient really needs to understand that lifelong hormone replacement therapy is needed because we have removed part or all of the pituitary gland. So that portion or the whole gland is not going to be producing those hormones anymore. So the patient will need to take those replacement hormones for the rest of their life. HYPOPITUITAR ISM What is hypopituitarism? Hypopituitarism is a disorder where there is a deficiency in one or more of the pituitary gland hormones. If you remember from our pituitary gland overview, this master gland releases six hormones from the ANTERIOR: Thyroid-stimulating hormone (TSH) Prolactin Follicle-stimulating hormone (FSH) Luteinizing hormone (LH) Adrenocorticotropic hormone (ACTH) Growth hormone (GH) And two hormones from the POSTERIOR pituitary gland: Antidiuretic hormone (ADH) Oxytocin When the body has a deficiency in one or more of these eight, this can cause a lot of problems. The most common hormone deficiencies resulting in hypopituitarism are GH, FSH, and LH. Pathophysiology of hypopituitarism It’s most common for hypopituitarism to be caused by an issue with the pituitary gland itself. This is easy to remember. Pituitarism — pituitary gland. The patient may have a pituitary tumor, a congenital defect, or a traumatic injury to the pituitary gland. More rarely, hypopituitarism is caused by an issue with the hypothalamus. In Endocrine Video 3 on GH, oxytocin and prolactin, Cathy teaches these endocrine hormone pathways: The hypothalamus releases corticotropin-releasing hormone (CRH), which causes the anterior pituitary gland to release ACTH. The hypothalamus produces thyrotropin-releasing hormone (TRH), which causes the anterior pituitary gland to release TSH. The hypothalamus releases growth hormone-releasing hormone (GHRH), which causes the anterior pituitary gland to release GH. The hypothalamus secretes gonadotropin-releasing hormone (GnRH), which causes the anterior pituitary gland to produce LH and FSH. The hypothalamus creates ADH and then it is stored in the pituitary gland to be released. Notice that 5 out of the 8 hormones released by the pituitary gland start in the hypothalamus. It makes sense that a problem with the hypothalamus could lead to a deficiency of one of those pituitary hormones. But usually, it’s a problem with the pituitary gland. Signs and symptoms of hypopituitarism Hypopituitarism can result from a deficiency in one or more of eight hormones. Therefore, there are a wide variety of signs and symptoms that are possible with hypopituitarism, depending on which of the hormones’ production is affected. The most common hormone deficiency behind hypopituitarism is GH, so delayed growth and development is a common sign. With hypopituitarism, another common deficiency is FSH and LH. Remember that FSH and LH are responsible for the production of sex hormones estrogen, progesterone and testosterone. So, deficiencies in FSH and LH can lead to decreased sexual function, and symptoms like amenorrhea (lack of menstrual period) in women and impotence in men. TSH is responsible for stimulating the thyroid to prompt it to produce thyroid hormones T3 and T4. So with a deficiency of TSH, the patient can then have a deficiency of T3 and T4, and may show the signs and symptoms of hypothyroidism. Thus, hypopituitarism with deficient TSH can cause secondary or tertiary hypothyroidism. Signs of hypothyroidism include weight gain, hypotension, bradycardia, lethargy, cold and intolerance. ACTH triggers the adrenal cortex to release cortisol, aldosterone and other androgens. So when there is a deficiency in ACTH, this can lead to a deficiency of those hormones, which is known as adrenocortical insufficiency or adrenal insufficiency. Signs of adrenocortical insufficiency include fatigue, weakness, weight loss, hypoglycemia, and hyponatremia. Lab values associated with hypopituitarism Pituitary hormone levels will be measured, but also the target hormones. Cathy covered the expected lab values for T3, T4, and TSH in the previous video in this series. Diagnosis of hypopituitarism ACTH stimulation test Remember, ACTH is one of the hormones released by the pituitary gland that causes the adrenal gland to release cortisol. If we give a patient an injection of ACTH, and their adrenal glands successfully produce cortisol in response (determined via a blood test), we know it was a problem with the pituitary gland. The adrenal glands were just waiting for enough ACTH to function properly. So, if we know it’s a problem with the pituitary gland, that’s how we diagnose hypopituitarism.However, if the patient gets the injection of ACTH, and they do not produce cortisol, we know it’s a problem with the adrenal glands themselves. The adrenal glands got what they needed, and were not able to complete their mission. CT/MRI A CT scan or MRI can also be used to diagnose hyperpituitarism. These tests will help identify any kind of tumor or abnormality (e.g., trauma, defect) in the pituitary gland. Treatment of hypopituitarism Treating hyperpituitarism requires hormone replacement therapy. Sometimes this therapy may be done with the pituitary hormones, and sometimes with the target hormones. Thyroid replacement hormones Levothyroxine (T4) is a synthetic thyroid hormone medication for hypothyroidism. Levothyroxine can be used to treat hyperpituitarism when there is a deficiency in TSH. Since TSH is required for the thyroid to produce T3/T4, if TSH is deficient, synthetic thyroid hormones may be needed. Growth hormone When a patient has hypopituitarism with GH deficiency, they may need a growth hormone replacement medication in the form of somatropin. Corticosteroids When a patient has hypopituitarism with ACTH deficiency, they may have a resulting deficiency in cortisol; so they may need a replacement medication for this. These are called corticosteroids or glucocorticoids and include prednisone, hydrocortisone, methylprednisolone, and dexamethasone. Later in this series you will learn that one of the key medications given to a patient with adrenocortical insufficiency is hydrocortisone. Dexamethasone, basically synthetic cortisol, is also used in the dexamethasone suppression test to diagnose Cushing’s syndrome. Sex hormones If a patient has hypopituitarism with FSH or LH deficiency, they may also be deficient in sex hormones. Thus, they may need to take replacement sex hormone medications like estradiol or testosterone. These medications and more are covered in our Pharmacology flashcards for nursing students. HYPERPITUITAR ISM Pathophysiology of hyperpituitarism Hyperpituitarism usually starts with a pituitary adenoma, which is a benign tumor in the pituitary gland, or tissue hyperplasia, which is an overgrowth of tissue. Either the adenoma or the tissue usually resides in the anterior pituitary gland, compressing the brain tissue and causing increased secretion of GH, prolactin and ACTH. Signs and symptoms of hyperpituitarism Hyperpituitarism symptoms can include intracranial pressure due to the compressed brain tissue. This pressure can lead to headaches, nausea and vomiting. Hyperpituitarism with growth hormone excess can result in symptoms like the hormone disorder acromegaly as well as arthralgia, which is joint pain. Hyperpituitarism with ACTH excess results in excess cortisol, so patients may have signs and symptoms of Cushing’s disease. Hyperpituitarism with excess prolactin can lead to symptoms of sexual dysfunction, like loss of sex drive. Because prolactin is the hormone that promotes lactation, excess prolactin can also lead to abnormal lactation. Diagnosis of hyperpituitarism To diagnose hyperpituitarism, the patient may need a CT scan or MRI, which will show the adenoma or tissue hyperplasia on the pituitary gland. Treatment of hyperpituitarism The surgery for hyperpituitarism is a hypophysectomy, which is removal of part or all of the pituitary gland. A medication that can be used for hyperpituitarism with growth hormone or prolactin excess, is the dopamine agonist levodopa/carbidopa. Levodopa and carbidopa help to inhibit growth hormone and prolactin secretion. Need to remember levodopa/carbidopa? Check out our Pharmacology flashcards for nursing students! Another medication for hyperpituitarism with GH excess is somatostatin, which is a medication for acromegaly. Somatostatin is actually a naturally-occurring hormone in the body that’s also known as growth hormone-inhibiting hormone. HYPOPHYSECTOMY What is a hypophysectomy? A hypophysectomy is a brain surgery to remove all or part of the pituitary gland. A transsphenoidal hypophysectomy is when the gland is removed through the nasal cavity, which is the more common approach. Sometimes, the hypophysectomy needs to go through the oral cavity, so an incision is made under the top lip. Nursing care following a hypophysectomy After a hypophysectomy procedure, the patient’s nose will drain. It’s important to monitor that drainage for signs and symptoms of a cerebrospinal fluid (CSF) leak. One sign of CSF leak is a halo sign in the drainage. This means there is clear or bloody fluid in the center of the drainage, but a yellow ring outside that drainage. If you see this halo sign, it can mean the patient has a CSF leak. Another sign of CSF leak is if the patient complains of a headache and also indicates that their drainage tastes sweet. If you test the drainage and it’s positive for glucose, that is another sign of CSF leak and will need to be further investigated. Patient teaching following a hypophysectomy After a patient has a hypophysectomy, it’s important as a med-surg nurse to teach them a few things they will need to know for their recovery. While a patient is healing from their hypophysectomy, they need to avoid activities that increase intracranial pressure. Activities that increase intracranial pressure include coughing, sneezing, blowing their nose, bending at the waist, and straining during bowel movements. With these patients, you will definitely be administering stool softeners and other options to help prevent straining during bowel movements. Following a hypophysectomy, it will be important to let your patient know that a decreased sense of smell is expected for about the first month after the procedure. It’s also recommended the patient not brush their teeth for two weeks, especially if the procedure was performed through the oral cavity. It is okay for the patient to floss and rinse their mouth. Finally, the patient must understand that they will need lifelong hormone replacement therapy after a hypophysectomy. The pituitary gland, or part of it, is gone and it will not be producing those hormones. Hormones that may need to be replaced include cortisol in the form of a glucocorticoid, and thyroid hormones. Med-Surg Endocrine System, part 9: Growth Hormone Deficiency and Excess GROWTH HORMONE DEFIC IENCY What is growth hormone deficiency? Growth hormone deficiency occurs when the anterior pituitary gland secretes an inadequate amount of growth hormone. It may be caused by a congenital disorder. It may also be due to trauma to the pituitary gland. Growth hormone deficiency can also be caused by a problem with the hypothalamus. If you recall from our overview on growth hormone (GH), the hypothalamus releases growth hormone-releasing hormone (GHRH), which causes GH to be produced in the anterior pituitary gland. So if the hypothalamus has a problem, it will not produce enough GHRH to instruct the pituitary gland to release GH, resulting in a GH deficiency. Signs and symptoms of growth hormone deficiency The primary symptom with growth hormone deficiency is a patient with short stature but proportional height and weight. Other signs and symptoms include reduced muscle mass and increased body fat. Because growth hormone plays such an important part in the puberty process, the onset of puberty may also be delayed. Diagnosis of growth hormone deficiency To diagnose growth hormone deficiency, there are several options available, including a growth hormone stimulation test, a bone age scan, or a CT scan of the patient’s head to look for abnormalities in the hypothalamus or pituitary gland. A growth hormone stimulation test triggers the pituitary gland to produce GH and then evaluates the amount that is produced. A bone age scan is an X-ray that assesses the maturity of the patients’ skeleton to see if it is appropriate for the patient’s age. Treatment for growth hormone deficiency with Somatropin A patient with growth hormone deficiency will need growth hormone replacement therapy. The drug for this is called somatropin, which can be used on children and adults, and is administered subcutaneously. Somatropin is used for growth hormone deficiency because it is similar to naturally occurring GH; it stimulates growth and anabolism. Some side effects that somatropin can cause are hyperglycemia and pancreatitis. Somatropin is just one of the hundreds of medications covered in our Pharmacology Flashcards. When to stop administering somatropin Throughout the growth hormone replacement therapy, the patient will have X-rays done so that growth rate and bone age can be monitored. The epiphyseal plate, also known as the growth plate, is a section on the end of long bones that allows the bones to grow. Epiphyseal closure, when these plates close, is when bones stop lengthening. When the patient is taking somatropin, it is important these X-rays be monitored for the epiphyseal closure. Stop treatment with somatropin prior to epiphyseal closure. GROWTH HORMONE EXCESS What is growth hormone excess? Growth hormone excess is excess secretion of GH from the anterior pituitary gland. Growth hormone excess causes increased growth of bone and cartilage, as well as increased protein synthesis. What causes growth hormone excess? Growth hormone excess is usually due to a tumor or lesion in the pituitary gland that causes it to pump out extra growth hormone. More rarely, growth hormone excess can be caused by hypothalamus dysfunction. If the hypothalamus produces too much growth hormone-releasing hormone, that causes excess growth hormone to be produced in the pituitary gland. Signs and symptoms of growth hormone excess Signs and symptoms of growth hormone excess depend on the onset of this disorder. Gigantism Growth hormone excess that occurs prior to the epiphyseal growth plate closure results in gigantism. Remember, epiphyseal closure is when the bones stop growing. So growth hormone excess that occurs before the bones stop lengthening can result in gigantism. The important signs and symptoms to know for this are excessive height (because skeletal growth velocity increases and the bones are still able to lengthen) and arthritis. Acromegaly Growth hormone excess that occurs after growth plate closure results in acromegaly. The signs and symptoms to know for acromegaly are enlarged hands and feet, a protruding jaw, kyphosis (abnormal curvature of the thoracic spine), arthritis, and an enlarged larynx. The enlarged larynx causes a deep, hollow voice. Famous person with acromegaly In the movie Princess Bride (one of Cathy’s favorites!) the giant Fezzik is played by Andre the Giant. Andre the Giant has acromegaly, with the deep and hollow voice, enlarged hands and feet, and kyphosis. Check it out, and that will help you remember the signs and symptoms of acromegaly. Diagnosis of growth hormone excess To diagnose growth hormone excess, the patient can get a CT/MRI of the pituitary gland to see if there is an abnormality like a lesion or tumor. Treatment for growth hormone excess The treatment for growth hormone excess is a hypophysectomy to remove all or part of the pituitary gland, if necessary. Learn more about hypophysectomy surgery. Growth hormone deficiency is where we have inadequate secretion of growth hormone from the anterior pituitary gland. This may be due to a congenital disorder. It may also be due to injury or damage to the pituitary gland, or it could be due to an issue with the hypothalamus. If you recall, the hypothalamus produces growth hormone-releasing hormone, or GHRH, and this allows for secretion of growth hormone. If we are not producing GHRH due to some issue with the hypothalamus, then the pituitary gland is not getting the signal it needs to produce growth hormone. So in terms of signs and symptoms of growth hormone deficiency, the primary thing we'll see is short stature in our patient but proportional height and weight. Other signs and symptoms may include reduced muscle mass, increased fat, and delayed puberty. So in terms of diagnosing this condition, we could do a growth hormone stimulation test as well as a bone age scan, and we could do a CT scan of the patient's head to take a look for abnormalities in the hypothalamus or the pituitary gland. In terms of treatment, we need to provide growth hormone replacement therapy. This is done with a drug called somatropin. We administer this through a subcutaneous route. If you want more details about somatropin, you'll notice here, on the back of card 21 if you're following along with cards [in our Medical-Surgical flashcards], there's a reference to Pharm card 109 [in our Pharmacology flashcards], and that card has information about somatropin. But some of the key points about administering somatropin, besides the fact that it's administered subcutaneously, is that we typically stop treatment with somatropin once X-rays show epiphyseal closure. So we would be doing X-rays throughout the therapy with the growth hormone replacement, and when we see that epiphyseal closure, that's typically when we terminate treatment with somatropin. Now let's talk about growth hormone excess. This is where we have excess secretion of GH from the anterior pituitary gland, and this may be due to some kind of tumor or lesion in the pituitary gland. That is most likely. But it could also be due to some kind of dysfunction in the hypothalamus. So if the hypothalamus produces too much growth hormone-releasing hormone, that causes excess growth hormone to be produced in the pituitary gland. So when we have excess growth hormone, this causes increased growth of bone and cartilage as well as increased protein synthesis. Signs and symptoms will depend on when we had the onset of this disorder. So if we have growth hormone excess prior to epiphyseal growth plate closure, this results in gigantism. And key signs and symptoms of gigantism include excessive height and arthritis. However, if we have onset of growth hormone excess after growth plate closure, this results in acromegaly. And signs and symptoms of acromegaly include enlarged hands and feet, a protruding jaw, kyphosis, which is an abnormal curvature of the thoracic spine, arthritis, as well as an enlarged larynx. So this enlarged larynx can cause a deep and hollow voice. So one of my favorite movies of all time is Princess Bride. If you haven't seen it, I totally recommend it. But Andre the Giant is a key actor in this movie, and he has acromegaly. So he has that deep and hollow voice. He definitely has enlarged hands and feet and that kyphosis. So check it out, and that will help you to remember the signs and symptoms of acromegaly. So to diagnose this condition, we would do a CT or MRI of the pituitary gland to basically see if we have got some kind of lesion or tumor there. And then, for treatment, we would do a hypophysectomy to remove part of the pituitary gland or all of the pituitary gland, if necessary. Med-Surg Endocrine System, part 10: Diabetes Insipidus and SIADH WHAT IS THE DIFFERENCE BETWEEN SIADH AND DI? With diabetes insipidus, the body has too little antidiuretic hormone (ADH), and with SIADH, the body has too much ADH. If you would like more in-depth information about ADH, we gave an overview of ADH in the pathophysiology section of this playlist. ANTIDIURETIC HORMONE REVIEW As a quick overview, ADH is released by the posterior pituitary gland in response to: Low blood volume Low blood pressure Hypernatremia (increased blood osmolarity) If the body senses any of these three things, it will release ADH from the posterior pituitary gland, which will cause the kidneys to reabsorb more water, which helps to: Increase blood volume Increase blood pressure Dilute the blood so the blood osmolarity drops to a normal level DIABETES INSIP IDUS Diabetes insipidus is sometimes jokingly called “the other diabetes,” meaning it’s not related to the much more common diabetes mellitus. The word diabetes comes from Latin and Greek meaning “siphon” or “to pass through,” referring to excessive urination common with the disease. The word insipidus comes from Latin meaning “tasteless,” referring to the diluteness of the urine. Pathophysiology Neurogenic diabetes insipidus Neurogenic diabetes insipidus happens when there is some kind of trauma or tumor in the hypothalamus or pituitary gland which is causing insufficient ADH to be released. Without enough ADH being released from the posterior pituitary gland, the kidneys are not getting the signal to reabsorb water. The prefix neuro- in neurogenic means nervous system, or more specifically, brain. The hypothalamus and pituitary gland are in the brain, so that’s how you can remember neurogenic diabetes insipidus. Nephrogenic diabetes insipidus With nephrogenic diabetes insipidus, the posterior pituitary gland is actually releasing the correct amount of ADH. But there’s a problem with the kidneys. They are not responding appropriately to the ADH signal. They are getting the ADH, but they don’t respond and don’t reabsorb more water. Why don’t the kidneys respond to the ADH? It may be due to some kind of kidney infection or damage. Sometimes kidney damage occurs from use of nephrotoxic medications. The prefix nephro- in nephrogenic means kidneys, so that’s how you can remember nephrogenic diabetes insipidus is a problem with the kidneys. Pretty easy! If you’d like to learn more about prefixes and suffixes that can help you easily decode disease names, check out our Medical Terminology Flashcards. Signs and symptoms of diabetes insipidus One of the telltale symptoms of diabetes insipidus is large amounts of dilute urine. Dilute urine is urine that has a higher concentration of water than is expected -- in this case, because the kidneys are not reabsorbing the water. Dilution or concentration of urine is measured by the urine specific gravity test, which we will cover shortly. Another key symptom of diabetes insipidus is polydipsia, which is excessive thirst. If you think about it, these two symptoms will exacerbate one another. If you are very thirsty, you will increase your water intake, but drinking tons of water will cause you to excrete large quantities of diluted urine, which can cause even more thirst in response to fluid loss! Easy way to remember polydipsia Diabetes inSIPidus will make you want to SIP more water because you're super thirsty! Other signs and symptoms of diabetes insipidus include dehydration, hypotension, and loss of appetite. Lab values associated with diabetes insipidus Urine specific gravity A urine specific gravity test measures the relative densities of a patient’s urine to the density of water. More specifically, it’s a ratio of the mass of urine to the mass of an equal volume of water, so it measures how dense or heavy the urine is compared to water. The closer the urine specific gravity ratio is to 1, the closer the urine’s density is to water. The expected range for urine specific gravity is 1.010 - 1.025. Lower than that is dilute urine, and higher than that is concentrated urine. Very low urine specific gravity, under 1.005, can indicate diabetes insipidus. Urine osmolality A urine osmolality test measures urine concentration, or the amount of dissolved substances in the urine. The expected range for urine osmolality is 300 - 900 mOsm/kg. Lower than that is dilute urine, and higher than that is concentrated urine. Very low urine osmolality, under 200, can indicate diabetes insipidus. Serum osmolality (blood osmolality) Blood (serum) osmolality is the amount of dissolved substances in the liquid part (plasma) of the blood. A large portion of these substances is sodium. Remember that one of the tasks that ADH gives the kidneys is to dilute the blood so its osmolality drops to a normal level. Without the kidneys doing that job, the blood becomes more concentrated and its osmolality rises. The expected range for serum osmolality is 275-295 mOsm/L. Lower than that is dilute blood, and higher than that is concentrated blood. Very high serum osmolality, over 300, can indicate diabetes insipidus. This is opposite of the urine osmolality, because the fluid shifting into the urine results in excessively dilute urine, but significant fluid loss from the blood. Sodium Sodium is an electrolyte that’s important for nerve and muscle function and maintaining fluid balance. Remember that a large portion of the substances in the blood is sodium — so as blood fluid levels drop and serum osmolality increases, sodium (Na) levels will also be high in a patient with diabetes insipidus. The expected range for sodium (na) is 136 - 145 mEq/L. Lower than that can indicate hyponatremia, and higher than that can indicate hypernatremia. In diabetes insipidus, the expected sodium level would be above 145 mEq/L. Having trouble remembering all these lab values? Urine specific gravity, urine osmolality, serum osmolality, and sodium are all covered in our Lab Values Flashcards. You can use these to practice for your nursing exams and as a reference guide if you’re a practicing nurse. Diagnosis of diabetes insipidus Water deprivation test Remember that one of the symptoms of diabetes insipidus is producing large volumes of dilute urine. Well, large volumes of dilute urine can also be a result of drinking large volumes of water. A water deprivation test basically checks to see what happens when you take the water away. Does the body behave normally when the water is taken away, or abnormally? Is the dilute urine due to too much water, or is the body actually unable to concentrate urine? Normally, water deprivation would cause increased production of ADH, which would trigger the kidneys to preserve fluid, resulting in smaller volumes of more concentrated urine. But if the patient is deprived of water in this test, and still produces dilute urine, this is abnormal and can indicate diabetes insipidus Vasopressin test The vasopressin test helps differentiate between neurogenic and nephrogenic diabetes insipidus. Remember that neuro means brain (pituitary gland) and nephro means kidneys. Vasopressin is a drug used as a hormone replacement for ADH. We expect it to do the same thing as ADH: trigger the kidneys to reabsorb water. If we give a patient vasopressin and their kidneys do not reabsorb water, we know it’s a kidney problem and we have nephrogenic diabetes insipidus. If we give the patient vasopressin and their kidneys successfully reabsorb water, then we know it was a problem with the pituitary gland not producing enough ADH, and we have neurogenic diabetes insipidus. Treatment (medications) for diabetes insipidus In the case of neurogenic diabetes insipidus, we can provide the patient medications like vasopressin or desmopressin (DDAVP) as an ADH replacement. Check out Cathy’s easy way to remember the side effects of antidiuretic hormones. Nursing care for diabetes insipidus When a patient has diabetes insipidus, you will want to montior their intake and output (I&Os), urine specific gravity, and daily weight. Weight is important because weight loss can occur with excessive fluid loss. Also, monitor for signs of fluid volume deficit: tachycardia, hypotension, poor skin turgor, dry/sticky mucus membranes. SYNDROME OF INAPPROPRIATE ADH (SIADH) Pathophysiology of SIADH You can think of SIADH as basically the opposite of diabetes insipidus. With SIADH, there is excess secretion of ADH from the posterior pituitary gland. Why does excess ADH get released? It can be due to a brain tumor, head injury, meningitis, or because of a medication. This excess ADH will be released even when serum osmolality is low (when the blood is diluted). This results in the kidneys reabsorbing more water — meaning the body retains too much water. Signs and symptoms of SIADH The key symptom of SIADH is a very small amount of concentrated urine. The body is holding onto the water so it’s not being released in the urine. There will also be signs and symptoms of fluid volume excess. This includes tachycardia (fast heart rate), hypertension (high blood pressure), crackles, jugular vein distention, and weight gain. Some other symptoms the patient may have are headache, weakness, and muscle cramping. With the blood diluted, this can lead to hyponatremia (abnormally low sodium), and one symptom of hyponatremia is confusion, especially in elderly patients. Check out Cathy’s nursing tip for the easy way to remember SIADH symptoms! Labs values associated with SIADH Remember that SIADH is the opposite of diabetes insipidus. With DI, the patient has dilute urine and concentrated blood — with SIADH, the patient has concentrated urine and dilute blood Urine specific gravity With SIADH a patient has concentrated urine, so that means a high urine specific gravity — the urine is a lot denser than water. Urine specific gravity will be over 1.03. Urine osmolality This concentrated urine will also result in a high urine osmolality, over 900 mOsm/kg. Serum osmolality (blood osmolality) The blood will be very dilute, which means a decreased serum osmolality, under 270 mOsm/L. Sodium Remember that a large portion of the substances in the blood is sodium — so when serum osmolality is low, sodium (Na) levels will also be low in a patient with SIADH. Sodium levels will be under 136 mEq/L, indicating hyponatremia. Treatment (medications) for SIADH One of the important medications for SIADH is a diuretic to try to eliminate the excess fluid. Within diuretics, you have loop diuretics (furosemide), thiazide diuretics (hydrochlorothiazide), osmotic diuretics (mannitol), and potassium sparing diuretics (spironolactone). Want to learn about diuretics in more detail? These medications are covered in our Pharmacology Flashcards. We can also give the patient a vasopressin antagonist. Remember that vasopressin is ADH and an antagonist blocks — blocking production of ADH makes sense for a patient with excess or uncontrolled ADH production. A patient with SIADH and hyponatremia can also be given hypertonic saline, an IV sodium solution, to slowly raise the sodium levels in their body and allow their electrolytes to balance. Nursing care for SIADH For a patient with SIADH, you will monitor their intake & output and weigh daily, just like the patient with diabetes insipidus. You will restrict fluids and replace sodium as ordered by the provider. Monitor for fluid volume excess. If the patient has too much fluid volume overload, that can lead to pulmonary edema which is life threatening, so it’s important to monitor for that. In the case of pulmonary edema, along with calling the healthcare provider, the nurse's priority action is to sit the patient up in tripod position over the bedside table. Remember that hyponatremia can lead to confusion. So you will want to monitor the patient’s neurological status for that. Also, you may need to implement seizure precautions, because hyponatremia can lead to seizures if it becomes severe. Diabetes insipidus vs. SIADH labs Lab Value Diabetes insipidus SIADH Urine output High Low Urine specific gravity Low (urine is dilute) High (urine is concentrated) Lab Value Diabetes insipidus SIADH Urine osmolality Low (urine is dilute) High (urine is concentrated) Serum osmolality High (blood is concentrated) Low (blood is dilute) Sodium High (hypernatremia) Low (hyponatremia) So both of these disorders have to do with ADH, either too much ADH, not enough ADH, or the organs in your body aren't responding appropriately to ADH. So let's do a quick review of ADH, and if you want more details about ADH, I did make a whole other video about it. But if you recall, ADH is released by the posterior pituitary gland in response to low blood volume in the body, low blood pressure, or to hypernatremia, or increased blood osmolarity. So if the body senses any of these three things, it will release ADH from the posterior pituitary gland, which will cause the kidneys to reabsorb more water, which helps to bring up that blood pressure, bring up that blood volume, and dilute the blood so that the blood osmolarity is back to a normal level. So with diabetes insipidus, we have one of two things going on. We may have neurogenic diabetes insipidus, which means that there is some kind of injury or tumor in the hypothalamus or the pituitary gland such that insufficient ADH is being released from the posterior pituitary gland. So if the posterior pituitary gland is not releasing enough ADH, the kidneys aren't getting the signal to reabsorb that water. So that is neurogenic diabetes insipidus. The other thing we may have going on is something called nephrogenic diabetes insipidus. So in this situation, the posterior pituitary gland is doing its job fine. It's releasing ADH. But there's some problem in the kidneys and they are not responding appropriately to that signal. Right? They're getting the ADH but they're kind of like, "Ehh." They're not reabsorbing more water. This may be due to some kind of kidney infection, or maybe the kidneys have been damaged due to nephrotoxic medications. But this is called nephrogenic diabetes insipidus. So in terms of signs and symptoms of diabetes insipidus, the key symptom is that the patient will have large amounts of dilute urine. So we're just dumping water. We're just peeing out tons of dilute urine. We're not reabsorbing that water as we should be. The patient will exhibit polydipsia, so this is where they have excessive thirst. And one way that I remember this symptom, if you look at the word diabetes insipidus, diabetes inSIPidus will make you want to SIP more water, because you're super thirsty. Other signs and symptoms include dehydration, hypotension, and anorexia. So in terms of labs, labs are definitely going to be important to know. The urine, like we talked about, is going to be very dilute. So the specific gravity of the urine will be very low, or under 1.005. Also the osmolarity of the urine will also be very low, because it's very dilute. So it will be under 200, and then we would expect kind of decreased sodium levels in the urine as well. In the blood though, that's a totally different story. Because we're getting rid of all those fluids, the blood's going to be really concentrated, so the serum, or blood osmolarity is going to be over 300, and the sodium levels are also going to be really high, so we're going to see hypernatremia. In terms of diagnosis of diabetes insipidus, we can do a water deprivation test to test the ability of the kidneys to concentrate urine. We can also do a vasopressin test. So vasopressin is essentially the same as ADH. And if we give the patient vasopressin, we would expect their kidneys to reabsorb water. If their kidneys don't do that, then we know it's a problem with the kidneys and we have nephrogenic diabetes insipidus. If we give the patient vasopressin and their kidneys do do their job and reabsorb water, then we know it was an issue with the pituitary gland not producing enough ADH. And if that is the case, then we can provide medications such as vasopressin or desmopressin, which you can find on Pharm card 110 [in our Pharmacology Flashcards] in terms of getting more information about those medications. So in terms of nursing care, when a patient has diabetes insipidus, we're definitely going to want to monitor the patient's I&Os, as well as their urine specific gravity and their daily weight. Let's move on to syndrome of inappropriate ADH, or SIADH. With SIADH, we have excess release of ADH from the posterior pituitary gland due to a brain tumor, head injury, meningitis, or because of a medication. So even though the blood is very dilute, the posterior pituitary gland still releases ADH, even though it should not. So because it's releasing all this extra ADH inappropriately, it's causing the kidneys to reabsorb more water. So signs and symptoms of SIADH will include a very small amount of very concentrated urine. And then we'll have signs and symptoms of fluid volume excess because we have all this extra fluid being reabsorbed. So the patient may exhibit signs and symptoms such as tachycardia, hypertension, crackles, jugular vein distention, as well as weight gain. They may also complain of a headache, weakness, and muscle cramping. And then they may also exhibit confusion because we have hyponatremia due to all this dilution, and that can cause the patient to be confused. So one way to remember what SIADH does, if you look at the first two letters of that, S-I, you can think of super inflated, and that's basically what happens. When you have SIADH, you reabsorb all this extra fluid, and you are super inflated. In terms of labs, we're going to have, basically, the exact opposite as we saw with diabetes insipidus. So the urine with SIADH will be super concentrated. So the urine specific gravity will be elevated. It will be over 1.03, and the urine osmolality or osmolarity will also be increased because it's so concentrated. The blood or the serum will be a completely different story. It will be very dilute, so the serum osmolality will be decreased. It will be under 270 and we'll see hyponatremia because the sodium is diluted with all this extra fluid volume. In terms of treatment, we're definitely going to give the patient diuretics to try to get rid of some of this excess fluid. We can also give them a vasopressin antagonist, and then we can also give them hypertonic saline to help bring up the sodium levels and allow for those electrolyte levels to be more in balance. In terms of nursing care, again, we're going to want to monitor the patient's I&Os, we're going to weigh our patients daily, and we're going to restrict fluids and replace sodium as ordered by the provider. We're going to monitor for fluid volume excess. So if we have too much fluid volume overload, we can end up with pulmonary edema, which is life threatening. So we're definitely going to want to monitor for that. And then we're going to want to continually monitor the patient's neurologic status because of the confusion that can result from hypernatremia, and we're also going to need to implement seizure precautions, because hypernatremia can result in seizures if it gets too bad. Med-Surg Endocrine System, part 11: Adrenocortical Insufficiency & Addisonian Crisis ADRENOCORTICAL INSUFFIC IENCY Adrenocortical insufficiency is inadequate secretion of hormones by the adrenal cortex. These hormones include aldosterone, cortisol, and androgens (sex hormones — the precursors for testosterone and estrogen). If you recall from our lesson on cortisol, the hypothalamus produces corticotropin-releasing hormone (CRH), which causes the pituitary gland to produce adrenocorticotropic hormone (ACTH), and this allows the adrenal gland to secrete cortisol. Primary causes of adrenocortical insufficiency With primary adrenocortical insufficiency, there is some kind of trauma or infection to the adrenal gland that causes partial or total destruction of the gland and prevents it from producing cortisol. Addison's disease One of the key causes of primary adrenocortical insufficiency is Addison's disease, which is an autoimmune disorder. In patients with Addison’s disease, the immune system is attacking, and therefore damaging, its own adrenal cortex. Secondary causes of adrenocortical insufficiency When there is a problem outside the adrenal gland, this is known as a secondary cause of adrenocortical insufficiency. If there is an insufficient amount of CRH from the hypothalamus or ACTH from the pituitary gland, this hypopituitarism can suppress the whole HPA system (hypothalamus-pituitary gland-adrenal cortex) and result in secondary adrenocortical insufficiency. Another cause of secondary adrenocortical insufficiency can be abrupt cessation of corticosteroids. Chronic use of corticosteroids can lead to inadequate function of the HPA system and thus, when the corticosteroids are stopped, the patient may find themselves with adrenocortical insufficiency. Signs and symptoms of adrenocortical insufficiency Signs and symptoms of adrenocortical insufficiency include weakness, fatigue, weight loss, hypotension (low blood pressure), dehydration, hypoglycemia, and a bronzed skin appearance. It has been reported that President John F. Kennedy had Addison’s disease, and if you look at pictures of him, you can see that he looks very tan. Apparently, this was not from sunbathing on the white house lawn. It’s because he had adrenocortical insufficiency due to Addison’s disease, and bronzed skin was definitely one of the side effects. Lab values associated with adrenocortical insufficiency The labs that you would see on a patient with adrenocortical insufficiency include elevated potassium, calcium, and blood urea nitrogen (BUN); and decreased cortisol, sodium and glucose. That’s a lot of lab values to remember for one disease. Cathy recommends you take the time to think critically about the hormones involved, which hormones are missing, you can deduce what the lab values and symptoms are. With adrenocortical insufficiency, the patient does not have enough cortisol. Cortisol is the stress hormone and over time can cause elevated levels of glucose. So low cortisol, low glucose (which is why hypoglycemia is a symptom). With adrenocortical insufficiency, the patient does not have enough aldosterone. If you recall from our lesson, aldosterone allows for reabsorption of water and sodium, and excretion of potassium. Low aldosterone, low sodium and water (which is why hyponatremia, hypotension, and dehydration are symptoms). And low aldosterone, potassium is not being excreted, so high potassium (which is why hyperkalemia is a symptom). Hormone Causes Without then…(lab) Cortisol Increasing glucose Low glucose Reabsorption of water High BUN, calcium Reabsorption sodium of Low sodium Hyponatremia Excretion potassium of High potassium Hyperkalemia Aldosterone this, Without (symptom) this, then… Hypoglycemia high Dehydration These lab values and many more are covered in our Lab Values flashcards for your convenience! This includes their normal ranges, and causes and symptoms of above/below range. Diagnosing adrenocortical insufficiency (ACTH stimulation test) We use the ACTH stimulation test to determine whether the patient has primary or secondary adrenocortical insufficiency. Remember, the hypothalamus produces CRH, which triggers the pituitary gland to product ACTH, so the adrenal gland can produce cortisol. Primary adrenocortical insufficiency In primary adrenocortical insufficiency, the adrenal gland itself has the problem. It’s actually getting sufficient ACTH, but it’s not doing its job in response to that. So if you give a patient the ACTH and nothing happens, you know it’s a problem with the adrenal gland and that patient has primary adrenocortical insufficiency. Secondary adrenocortical insufficiency In secondary adrenocortical insufficiency, the problem is further back along the chain. The body is not getting the ACTH it needs from its pituitary gland in order to stimulate the adrenal cortex to release cortisol. So if you give a patient ACTH and their adrenal gland suddenly starts producing cortisol like it’s supposed to, then you know it was not an issue with the adrenal gland, and was actually an issue with the pituitary gland or hypothalamus. Therefore, you know it’s secondary adrenocortical insufficiency. Treatment of adrenocortical insufficiency One of the key medications for a patient with adrenocortical insufficiency is hydrocortisone. This corticosteroid (glucocorticoid) is a hormone replacement drug for cortisol. This patient’s hyperkalemia also needs to be treated — hyperkalemia is dangerous and can cause cardiac dysrhythmias. Kayexalate (sodium polystyrene sulfonate) is one hypokalemic agent that can be used for this. You can also give the patient insulin to lower potassium levels. Insulin helps move potassium into the cells and out of the bloodstream. The problem is, insulin does the same with glucose, and this patient already has hypoglycemia. They shouldn’t be losing more glucose. So this patient would need insulin with glucose. The patient may also need calcium gluconate, like Kalcinate, to help protect their heart from the detrimental effects of hyperkalemia. Nursing care for adrenocortical insufficiency When it comes to giving nursing care to a patient with adrenocortical insufficiency, administer fluids and electrolytes as ordered. Provide food and supplemental glucose to help treat the hypoglycemia. Ensure continuous cardiac telemetry is in place due to the changes in potassium levels. Monitor for fluid volume deficit if kayexalate is administered, as this can lead to diarrhea. Patient teaching A patient with adrenocortical insufficiency might need additional corticosteroid doses during times of illness or stress in the future, so they don’t get too low on their cortisol levels. ADDISONIAN CRISIS An Addisonian crisis is a life-threatening disorder caused by adrenal insufficiency. It’s a critical care topic important for Med-Surg exams like the NCLEX. Causes of an Addisonian crisis Causes of an Addisonian crisis can include stress and trauma. Normally, the body greatly increases cortisol production to handle stress, but in a patient with adrenal insufficiency, those cortisol stores can become quickly depleted, leading to acute onset of all the symptoms of adrenal insufficiency. Other causes can include infection or abrupt discontinuation of corticosteroids. Signs and symptoms of an Addisonian crisis Signs and symptoms of an addisonian crisis are very similar to the signs and symptoms of general adrenal insufficiency. This means weakness, fatigue, dehydration, etc. But in an Addisonian crisis, the patient will have severe hypotension, and this can cause the patient to go into shock. You may also see dysrhythmias because of the very elevated levels of potassium (hyperkalemia). Treatment of an Addisonian crisis To treat an addisonian crisis, the patient will need IV glucocorticoids as well as fluids with dextrose (glucose). It’s also important to find and treat the underlying cause of the Addisonian crisis. For example, if the patient has an infection or some kind of trauma, that needs to be addressed and treated. Nursing care for an Addisonian crisis When providing care to a patient undergoing an Addisonian crisis, make sure to closely monitor their vital signs, their I&Os, and their weight. You should also monitor the patient for signs of shock. Some of the key signs of shock include decreased levels of consciousness and decreased urine output, below 30 ml/hour. Monitor the patient for dysrhythmias because of the hyperkalemia, and provide them with bed rest and a quiet environment to reduce stress. Reducing stress reduces the cortisol their body needs to use. So what is adrenocortical insufficiency? This is where we have insufficient secretion of hormones from the adrenal cortex. These hormones include aldosterone, cortisol, and androgens. So in terms of the pathophysiology behind this disease, we have either primary causes or secondary causes of this disease. With primary causes, we have some kind of injury or infection to the adrenal gland that causes partial or total destruction of the gland. One of the key causes of primary adrenocortical insufficiency is Addison's disease, which is an autoimmune disorder. In terms of secondary causes of adrenocortical insufficiency, this is where we have problem outside of the adrenal gland. One secondary cause is abrupt discontinuation of corticosteroid therapy. Another secondary cause could be an issue with the pituitary gland or the hypothalamus. So if you recall, the hypothalamus produces CRH which causes the pituitary gland to produce ACTH and this prompts the adrenal gland to secrete cortisol. So if we have issues with either the hypothalamus or the pituitary gland, then the adrenal gland isn't getting the right message to produce cortisol. So those are secondary causes of adrenocortical insufficiency. In terms of signs and symptoms, signs and symptoms include weakness, fatigue, weight loss, hypotension, dehydration, hypoglycemia, and a bronzed skin appearance. So it's been reported that JFK, President Kennedy, had Addison's disease, and if you look at pictures of him, he always has this very tan or bronzed appearance, which, apparently, was not from laying out in the sun. It's because he had Addison's disease and this is definitely one of the side effects. In terms of labs that you will see when someone has adrenocortical insufficiency, you would expect elevated potassium, calcium, and BUN, but you would expect decreased cortisol, sodium, and glucose. Instead of just remembering all these up or down labs, if you think about the hormones involved and which hormones we don't have enough of, you can kind of better understand or think critically about what values will be up and which values will be down. So with this disease, we don't have enough cortisol. And if you recall, cortisol is our stress hormone and it causes elevated levels of glucose. Well, if we don't have enough cortisol, then our glucose levels go down and that's why we have hypoglycemia. Also, with this disorder, we don't have enough aldosterone. And if you recall, aldosterone allows for reabsorption of water and sodium and excretion of potassium. So when we don't have enough aldosterone, we are not reabsorbing all that water and sodium. We're excreting it instead, which is why we end up with hyponatremia as well as hypotension and dehydration, just getting rid of all that water. But we're also retaining all that potassium instead of excreting it. So that's why we end up with hyperkalemia. So it all comes down to really understanding what those hormones are supposed to do, and then you can really understand what to expect when those hormones are not on board. Right. Now let's now talk about diagnosis of adrenocortical insufficiency. We would use an ACTH stimulation test to help differentiate whether we have primary adrenocortical insufficiency or secondary causes of this disorder. So if a patient has a primary cause of this disorder that means there's a problem with the adrenal gland itself and it's getting sufficient ACTH from the pituitary gland and it doesn't care, like, "You can give me all the ACTH you want. I'm just not going to produce cortisol." So if we give them external ACTH, it doesn't care. He's like, "You can give it to me from the pituitary gland or externally. Either way, I'm kind of injured or damaged and I'm not going to produce cortisol." So we give them the ACTH. If that doesn't make any difference, then we know it is a primary cause of adrenocortical insufficiency. There's a problem with the adrenal gland. However, if we give the patient who has a secondary cause of this disorder ACTH-- so with the secondary cause, remember they're not getting enough ACTH from the pituitary gland. If we give them the ACTH and the adrenal gland's pumped and excited, like, "Finally. I've been waiting for this ACTH and it hasn't been coming. And now I can produce cortisol." So if the adrenal gland suddenly starts producing cortisol like it's supposed to, then we know it was an issue with the pituitary gland or the hypothalamus. It's a secondary cause of this disorder. That's an explanation of how this ACTH stimulation test works. In terms of treatment, one of the key medications we'll give somebody who has adrenocortical insufficiency is hydrocortisone. We also need to treat that hyperkalemia because if you recall, hyperkalemia is really dangerous and can cause cardiac dysrhythmias. So you really want to bring those potassium levels down. And ways we can do this is-one medication is called Kayexelate. That helps to bring potassium levels down. You can also give the patient insulin. So insulin helps move potassium into the cells and out of the bloodstream. The only problem is, it also moves glucose into the cells and out of the bloodstream and we have hypogyclemia with this disease. So if we're giving the patient insulin to help bring those potassium levels down in the bloodstream, we also need to give them glucose in order to bring up those glucose levels in the bloodstream. So we're going to give insulin with glucose. We're also going to need to give the patient calcium gluconate to help protect their heart from the detrimental effects of hyperkalemia. In terms of nursing care, we're definitely going to administer our fluids and electrolytes as ordered. We're going to provide food and supplemental glucose to help treat that hypoglycemia. And we're going to teach the patient that in the future, additional corticosteroid doses may be needed during times of illness or stress so that they don't get too low on their cortisol levels. Now let's talk about an Addisonian crisis. So if you're following along with cards, I'm on Card 29 in the endocrine system [in the Medical-Surgical Flashcard deck]. An Addisonian crisis is where we have a lifethreatening disorder caused by adrenal insufficiency. And causes of this crisis can include infection, stress, trauma, or abrupt discontinuation of corticosteroids. In terms of the signs and symptoms, a lot of them are going to be fairly similar to what we just talked about. So weakness, fatigue, that type of thing. But we're also going to have severe hypotension that can cause shock. And then, we also may have dysrhythmias because we have very elevated levels of potassium. In terms of treatment, we're definitely going to give this patient IV glucocorticoids as well as fluids with dextrose. And we need to really identify and treat the underlying cause of this crisis. So if the patient has infection or some kind of trauma, we need to try to address that. In terms of nursing care, we're going to want to closely monitor this patient's vital signs, their I&Os, and their weight. And monitor for signs of shock. Some of the key signs of shock include decreased level of consciousness and decreased urine output. So urine output that drops below 30 ml per hour. We're also going to want to closely monitor for dysrhythmias because of that hyperkalemia and provide the patient with bed rest and a quiet environment. Med-Surg Endocrine System, part 12: Glucocorticoid Hormone Excess (Cushing's Syndrome) WHAT IS CUSHING’S SYNDROME? Cushing’s syndrome (glucocorticoid hormone excess) happens when there is an overproduction of cortisol by the adrenal cortex. If you remember from our review on endocrine hormones, the hypothalamus produces CRH, which causes the anterior pituitary to release ACTH, which prompts the adrenal cortex to release cortisol. Cushing’s syndrome can be caused by an adenoma (benign tumor) in the adrenal gland or pituitary gland. This syndrome is also often caused by prolonged steroid use. If the problem is with the pituitary gland, this is called hyperpituitarism, which we covered in video 8 of this series. The elevated cortisol levels caused by this syndrome also cause increased glucose levels, protein catabolism, altered fat metabolism, and a decreased immune response in the body. This decreased immune response makes the patient more susceptible to infection. SIGNS AND SYMPTOMS OF CUSHING’S SYNDROME Many of the signs and symptoms of glucocorticoid hormone excess are the same as the side effects of prednisone, which is a glucocorticoid. This includes: A “buffalo hump,” which is a fat deposit between the shoulders on the back. “Moon face,” which is a puffy rounded face Truncal (torso) obesity Weight gain Fluid retention Peptic ulcer disease Diabetes Bone loss Weakness Emotional instability Increased infection When Cathy was pregnant, she had severe hyperemesis (extreme, persistent nausea), and was given prednisone. So she had the resultant moon face. She remembers telling her family about her debilitating illness, with constant vomiting and inability to eat. They looked at her moon face and thought, “Looks like she’s eating alright to me!” But really she wasn’t. And she and her husband can both recall the emotional instability side effect as well! If you also remember that cortisol is responsible for regulating the metabolism and immune response, you can piece together that the side effects are weight gain (poorly regulated metabolism) and a poor immune response. When you have Cushing’s, it will make you look like a cushion. (Because of all the fluid retention, moon face and weight gain.) LAB VALUES ASSOCIATED WITH CUSHING’S SYNDROME Increased glucose and sodium are expected with Cushing’s syndrome, as well as decreased potassium and calcium. In addition, the patient will have elevated levels of cortisol in their saliva. These lab value ranges are covered in detail in our Lab Values flashcards, including normal ranges and causes/symptoms/treatment for abnormal values. DIAGNOSIS OF CUSHING’S SYNDROME Cushing’s syndrome can be diagnosed with a dexamethasone suppression test, and then a CT, MRI, or ultrasound to check the pituitary and adrenal glands for a tumor. Dexamethasone suppression test Dexamethasone is a glucocorticoid, basically synthetic cortisol. Remember, these hormones act in a negative feedback loop. If a healthy patient is given dexamethasone, the pituitary gland should sense that there is extra cortisol, so it should scale back production of ACTH, which should cause the adrenal gland to reduce production of cortisol. If the pituitary gland does not scale back ACTH despite the extra cortisol, the negative feedback loop has failed and there must be interference in the pituitary gland—likely, an adenoma. However, if the pituitary gland performs the expected response effectively and scales back production of ACTH, but the adrenal gland just keeps secreting cortisol, we know it’s an issue with the adrenal gland. TREATMENT FOR CUSHING’S SYNDROME If there is a tumor on the pituitary gland, the surgery required for that is a hypophysectomy. If there is a tumor on the adrenal gland, the surgery for that is an adrenalectomy, which is certainly an easier name to remember! Ketoconazole is an antifungal medication that works for Cushing’s syndrome because it inhibits cortisol synthesis. There are some severe side effects to look out for with ketoconazole, including hepatotoxicity, which means it’s basically toxic to the liver. Another side effect is GI bleeding. Ketoconazole is one of the many medications covered in our Pharmacology flashcards. NURSING CARE FOR CUSHING’S SYNDROME Diet Because a patient with Cushing’s syndrome is retaining fluid and sodium, you will need to make sure to restrict their fluid and sodium. Also, encourage increased intake of potassium, calcium, and protein. What to monitor A patient with Cushing’s syndrome needs to be monitored for fluid-volume overload and pulmonary edema. Because this patient is retaining so much fluid, it will start affecting the lungs and the patient’s ability to breathe properly. Protection/prevention A patient with Cushing’s syndrome has fragile skin. With so much fluid retention, their skin becomes paper thin, which makes it fragile and easy to break down. So handle this patient with care! This patient should also be protected from bone fractures because of the side effect of bone loss that comes with Cushing’s syndrome. So, implement fall procedures according to your facility policy This patient needs to be protected from GI bleeding since they are at increased risk for this to happen. So, for example, do NOT give this patient a medication like an NSAID or aspirin, as these medications reduce blood clotting and could exacerbate the issue and increase the risk of GI bleeding. Finally, we want to prevent infection in a patient with Cushing’s syndrome because their immune response is decreased. Med-Surg Endocrine System, part 13: Pheochromocytoma & Hyperaldosteronism PHEOCHROMOCYTOMA Pathophysiology of pheochromocytoma Pheochromocytoma is a rare tumor on the adrenal gland, which causes excess secretion of norepinephrine and epinephrine. If you remember from our overview of norepinephrine and epinephrine, these hormones are catecholamines from the adrenal medulla. Another way to think about pheochromocytoma is to break down the word. Pheo- comes from the Greek phios, which means dark or dusky, -chromo- means color, -cyt- which means cell, and -oma, which means tumor. When cells from the adrenal medulla are treated with chromium salts (preserved), they turn a signature dark brown color. So, “pheochromocyt-” means “dark brown cells” but it’s really referring to cells of the adrenal medulla. Unfortunately, this root is a bit weird, but at least with -oma, you can remember that it’s a tumor. To learn more root words that will help you translate medical words you might not recognize (for instance, in crunch time on an exam!) check out our Medical Terminology flashcards. Signs and symptoms of pheochromocytoma Signs and symptoms of pheochromocytoma include tachycardia (heartbeat above 100 BPM), hypertension, headache, diaphoresis (excessive sweating), and shortness of breath. If you want to think critically to remember the synonyms for pheochromocytoma, remember that this disorder is caused by an excess secretion of norepinephrine and epinephrine (adrenaline), which are the fight or flight hormones released in response to acute stress. If you are acutely stressed, your heart is beating faster, blood pressure is going up, and you’re sweating. Diagnosis of pheochromocytoma There are multiple methods to diagnose pheochromocytoma: a 24-hour urine test, a clonidine suppression test, or a CT/MRI to locate an adrenal tumor. 24 hour urine test To diagnose a patient with pheochromocytoma, we can perform a 24-hour urine test. A 24-hour urine test tests for vanillylmandelic acid and metanephrine, which are byproducts from the breakdown of epinephrine and norepinephrine. Elevated levels of vanillylmandelic acid and metanephrine in the urine over a 24-hour period can indicate pheochromocytoma. Clonidine suppression test Another way to diagnose pheochromocytoma is with a clonidine suppression test. Clonidine is a medication for high blood pressure that acts on the central nervous system to decrease sympathetic outflow. With decreased sympathetic nervous system outflow, you should see decreased secretion of epinephrine and norepinephrine. However, if this patient shows continued high levels of epinephrine and norepinephrine regardless of central nervous system function, this strongly indicates there is a problem with the adrenal medulla and the pheochromocytoma tumor may be present. Treatment for pheochromocytoma Adrenalectomy The patient with pheochromocytoma will need surgery to remove the tumor. This surgery is known as an adrenalectomy, which is a removal of one or both of the adrenal glands. This one is easy to remember since adrenal is obviously adrenal, and the suffix -ectomy means removal. Ectomy is one of the suffixes you will encounter very often. Thyroidectomy, hypophysectomy, and adrenalectomy are all surgery options you will need to be familiar with for your Med-Surg exams. We created our Medical Terminology flashcards to help you know which suffixes, prefixes, roots and abbreviations are the most important ones for nursing school and healthcare practice in general. Antihypertensive medications Before a patient with pheochromocytoma undergoes adrenalectomy surgery, they will still have symptoms that include potentially dangerous hypertension, and will require specific antihypertensive medications. Some of the commonly prescribed antihypertensives before an adrenalectomy are the beta blockers metoprolol, atenolol and propranolol. If you’re studying for a pharmacology exam, there are a lot of different antihypertensive medications to know. In our Pharmacology series, we cover the antihypertensives you will most need to know for ATI, NCLEX, HESI, or a Pharm exam. This video series corresponds with our Pharmacology flashcards, which makes memorizing these medications easy. Nursing care for pheochromocytoma Here’s something important to remember about the nursing care for a patient with pheochromocytoma: do not palpate the abdomen. Although abdomen palpation is a step in physical assessment, it should not be done on this patient because it can cause a sudden release of catecholamines, which can trigger severe hypertension which is very dangerous for this patient. HYPERALDOSTERONISM Pathophysiology of hyperaldosteronism Hyperaldosteronism is an excess amount of aldosterone secreted by the adrenal gland, caused by an adenoma or tissue overgrowth in that adrenal gland. If you have been following along in our Endocrine series, you might have noticed that glandular tumors often result in excess secretion of the hormone that gland is supposed to secrete, which can lead to a disease or disorder. As above, in the adrenal medulla can result in an excess secretion of norepinephrine/epinephrine and cause pheochromocytoma. Video 8: A tumor (or tissue overgrowth) in the anterior pituitary can cause increased secretion of GH, prolactin, and ACTH, resulting in hyperpituitarism. Video 9: A tumor on the pituitary gland or hypothalamus can result in an excess section of growth hormone — growth hormone excess. Video 12: A tumor on the pituitary or adrenal gland can result in an excess secretion of cortisol and result in Cushing’s syndrome. Video 15: A nodule (small tumor) on the thyroid gland OR a pituitary tumor can cause increased secretion of T3 and T4 and lead to hyperthyroidism. Signs and symptoms of hyperaldosteronism Signs and symptoms of hyperaldosteronism include hypertension, headache, weakness, paresthesias (pins and needles), and tetany (muscle spasms or cramps). In order to think critically about the symptoms of hyperaldosteronism, remember what aldosterone does. If you recall from our overview of aldosterone, aldosterone causes reabsorption of sodium and water and excretion of potassium. So if we have too much aldosterone, this causes too much sodium and water to be reabsorbed and too much potassium to be excreted. When excess water is reabsorbed, this increases the blood volume, which increases blood pressure. Lab values associated with hyperaldosteronism The lab values that are often associated with hyperaldosteronism are high sodium and low potassium, and...drumroll please...increased aldosterone! The expected range of sodium is 136 - 145 mEq/L, and sodium amounts greater than 145 mEq/L can indicate hypernatremia. Hypernatremia is seen in patients with hyperaldosteronism because their excess aldosterone causes that excess reabsorption of sodium and water. The expected range of potassium is 3.5 - 5.0 mEq/L, and potassium amounts less than 3.5 can indicate hypokalemia. Hypokalemia is seen in patients with hyperaldosteronism because their excess aldosterone causes that excess excretion of potassium. Hypokalemia can be dangerous for the patient because it can put them at risk for life-threatening dysrhythmias. (Check out our EKG series to learn more about the different dysrhythmias!) We created our Lab Values flashcards to help you remember the ranges of sodium, potassium, and 64 other lab values you need to know for most nursing exams. Diagnosis of hyperaldosteronism There is no special test The main way that hyperaldosteronism is diagnosed is through a CT scan of the adrenal gland. This CT scan allows us to see if there is a tumor on the adrenal gland. Treatment for hyperaldosteronism An adrenalectomy, which we described above for pheochromocytoma, may be what’s needed for hyperaldosteronism. We can also give a patient with hyperaldosteronism a potassium-sparing diuretic, which will help them get rid of the excess fluid, but also help them keep their potassium, which is important since they are low. The potassium-sparing diuretic you’ll likely need to know for exams is spironolactone,which is covered in the Renal system section of our Pharmacology flashcards. In rare cases, glucocorticoid therapy can be used for hyperaldosteronism. When this is the case, the disorder is known as glucocorticoid-remediable aldosteronism. Nursing care for hyperaldosteronism When you are caring for a patient with hyperaldosteronism, it’s important to monitor their blood pressure, their input & outputs, and their potassium levels (since potassium dropping too low can be very dangerous). A patient with hyperaldosteronism should make sure their diet is low in sodium (since they have too much sodium already) and high in potassium (since they don’t have enough). Let's first talk about pheochromocytoma, which is where we have a tumor on the adrenal gland, which causes excess secretion of norepinephrine and epinephrine, which are catecholamines from the adrenal medulla, which is like the inside part of the adrenal gland. So with this excess secretion of epinephrine and norepinephrine, that activates the body's sympathetic response, and basically, throws the body into fight or flight mode. So signs and symptoms of this condition include tachycardia, hypertension, headache, diaphoresis, and shortness of breath. In terms of diagnosis, we can do a 24-hour urine test where we test for byproducts from the breakdown of epinephrine and norepinephrine. So some of these byproducts include vanillylmandelic acid as well as metanephrine. So if we find that we have elevated levels of these substances over a 24-hour period in the urine then that would be indicative of pheochromocytoma. The other test we can do is a clonidine suppression test. So clonidine is a medication we give for high blood pressure. It acts on the central nervous system and should decrease the sympathetic outflow and with decreased sympathetic nervous system outflow, we should have decreased secretion of epinephrine and norepinephrine. However, if we have continued high levels of epinephrine and norepinephrine being released from the adrenal gland regardless of central nervous system function, then that is also strongly indicative that we may have a tumor and pheochromocytoma present. And then lastly, we can, of course, do a CT/MRI of the adrenal gland to help identify that tumor. So in terms of treatment, the patient's going to need surgery. We need to remove that tumor and they may need an adrenalectomy. And then prior to surgery, we definitely want to be giving the patient antihypertensive medications because of that extreme hypertension that's related to this disorder. One important thing for you to remember as a nurse is you never want to palpate the abdomen of a patient who is suspected of having pheochromocytoma because that can trigger the sudden release of catecholamines, which, in turn, can trigger severe hypertension in the patient, which can be very dangerous. Now let's talk about hyperaldosteronism. This is where we have an adenoma or hyperplasia in the adrenal gland such that excess amounts of aldosterone are being secreted. And if you recall, aldosterone is a hormone that causes reabsorption of sodium and water and excretion of potassium. So if we have too much aldosterone, that's going to cause excess reabsorption of sodium and water and excess excretion of potassium. So in terms of signs and symptoms, hypertension is going to be a key symptom, and it makes sense, right? If we are reabsorbing all this water, that's going to bring our blood volume up, which is going to increase blood pressure. Other signs and symptoms include headache and weakness. In terms of the labs we'll see with this condition, because we're reabsorbing all of this sodium and water, we're going to have hypernatremia. And because we're getting rid of all this potassium, we're going to have hypokalemia, which can be dangerous to the patient. Anytime we have abnormally high or low levels of potassium, that places the patient at risk for life-threatening dysrhythmias. Aldosterone will be elevated in these patients, which makes sense because we're talking about hyperaldosteronism. And then in terms of diagnosis, we can do a CT scan of the adrenal gland. And then treatment may include an adrenalectomy. Also, we can give the patient a potassium-sparing diuretic, which is spironolactone. So that will help get rid of that excess fluid, but retention of potassium, which is important for this patient. And then in terms of nursing care, we're definitely going to want to monitor the patient's blood pressure, their I's and O's, and their potassium levels. And then we want to encourage that patient to consume a low-sodium and high-potassium diet in order to help balance those electrolyte levels. Med-Surg Endocrine System, part 14: Hypothyroidism & Myxedema Coma HYPOTHYROIDIS M Hypothyroidism is a disease marked by inadequate production of T3 and T4, which are thyroid hormones from the thyroid gland. TRH, TSH, T3/T4 hormone review If you remember from our overview on thyroid hormones, the hypothalamus produces thyroid-releasing hormone (TRH), which causes the pituitary gland to produce thyroid-stimulating hormone (TSH), which prompts the thyroid gland to produce the thyroid hormones T3 and T4. You can think of the chain like this Hypothalamus produces TRH Pituitary gland produces TSH Thyroid produces T3/T4 Pathophysiology of hypothyroidism To understand the differences between primary, secondary and tertiary hypothyroidism, you can flip the chain backwards (so that you are starting from the thyroid). Thyroid produces T3/T4 Pituitary gland produces TSH Hypothalamus produces TRH Primary hypothyroidism In primary hypothyroidism, there is a problem with the thyroid gland itself. If the thyroid gland is damaged, it cannot produce the T3 and T4 that it should. The leading cause of primary hypothyroidism is Hashimoto’s disease. Hashimoto’s disease, also called chronic lymphocytic thyroiditis, is an autoimmune disorder that causes antibodies to attack and destroy the thyroid tissue. It occurs most commonly in middle-age women, but can occur in others. Secondary hypothyroidism Secondary causes of hypothyroidism occur when there is an issue with the pituitary gland, like a pituitary tumor. In this case, the pituitary gland is not functioning properly and therefore not producing enough TSH. Remember TSH is thyroid-stimulating hormone, so without the right stimulation, the thyroid gland is not prompted to make the correct amount of T3/T4. Tertiary hypothyroidism Tertiary hypothyroidism occurs when there is a dysfunction of the hypothalamus. It creates a domino effect along the hormone pathway. If there is a problem with the hypothalamus, then it’s not producing enough TRH, so the pituitary gland is not being prompted to make enough TSH, so the thyroid gland doesn’t get the message to produce adequate T3/T4. How to remember primary vs. secondary diseases You can always remember that with a “primary” version of a disease, it means there’s an issue closest to the source, rather than several steps away along the chain. For example, in adrenocortical insufficiency, when the adrenal glands aren’t producing enough cortisol, the primary type is when there is a problem with the adrenal gland itself. In hyperparathyroidism, when the parathyroid gland is secreting too much PTH, the primary type is when there is a problem with the parathyroid glands themselves. If you know which gland produces which hormone in which order, you’ll easily be able to understand whether a disorder is the primary, secondary or tertiary type. That’s why it’s so important to have a good understanding of the hormone pathways that lead to endocrine diseases and disorders. If you need a refresher, check out these A&P reviews we put together for the endocrine system in med-surg: Med-Surg Endocrine System, part 2: Organs, glands & hormone overview Med-Surg Endocrine System, part 3: Cortisol, T3/T4, GH, Estrogen, Progesterone, Testosterone, Oxytocin & Prolactin Med-Surg Endocrine System, part 4: ADH, Aldosterone & RAAS Med-Surg Endocrine System, part 5: Epinephrine, Norepinephrine, Calcitonin, PTH, Insulin & Glucagon Med-Surg Endocrine System, part 6: Negative Feedback Mechanism vs. Positive Feedback Mechanism Signs and symptoms of hypothyroidism The signs and symptoms of hypothyroidism include hypotension, bradycardia, lethargy, cold intolerance, constipation, weight gain, thin hair, brittle fingernails and depression. If you want to think critically to deduce the signs and symptoms of hypothyroidism, remember from our hormone overview what T3/T4 controls: Metabolism. So when those hormones are low, the metabolism becomes sluggish and you see weight gain, cold intolerance (body temperature regulation), and lethargy. Heart function. So when those hormones are low, you see that slower heart function with bradycardia and hypotension. Digestion.So when those hormones are low, you see reduced digestive capabilities like constipation. Bone maintenance.So when those hormones are low, you see brittle fingernails. Lab values When it comes to the lab values you might see with hypothyroidism, you will be looking at T3/T4 and TSH. The measurement of these hormones is known as a thyroid panel, which we explained in video 7 of this series. These are the most important endocrine lab values to know for your Med-Surg exams, whether a course final, your ATI or NCLEX. Lab values can be dispersed throughout your textbooks, which is why we created our Lab Values flashcards, to keep the most important lab values you need to know for your exams all in one place that’s easy to study! Primary hypothyroidism: Low T3/T4, high TSH Secondary hypothyroidism: Low T3/T4, low TSH Tertiary hypothyroidism: Low T3/T4, low TSH T3/T4 values with hypothyroidism In all types of hypothyroidism, you will see decreased T3/T4. That’s an easy one, because that’s what this disease is marked by! The expected range for T3 in a thyroid panel is 70 - 204 ng/dL. T3 levels under 70 ng/dL can indicate hypothyroidism. The expected range for T4 in a thyroid panel is 4 - 12 mcg/dL. T4 levels under 4 mcg/dL can indicate hypothyroidism. TSH values with hypothyroidism The TSH value you will get back in a thyroid panel for hypothyroidism really depends on if you are looking at primary, secondary, or tertiary hypothyroidism With primary hypothyroidism, remember there is an issue in the thyroid gland itself causing inadequate production of T3/T4. However, the pituitary gland is functioning fine in this scenario, and its job is to make TSH to prompt the thyroid gland. It’s prompting desperately, but the thyroid is not responding. So with primary hypothyroidism, you will see elevated levels of TSH. The expected range for TSH in a thyroid panel is 0.5 - 5.0 mU/L. TSH levels greater than 5 mU/L can indicate primary hypothyroidism when accompanied by low T3/T4. With secondary or tertiary hypothyroidism, the pituitary gland is not functioning properly (by itself, or because of a dysfunctional hypothalamus) and therefore not producing enough TSH. So with secondary or tertiary hypothyroidism, you will see decreased levels of TSH. TSH levels under 0.5 mU/L can indicate secondary or tertiary hypothyroidism when accompanied by low T3/T4. Over the years, there have been periods of time when Cathy thought she had hypothyroidism. She noticed she was tired, cold, and had gained some weight. So she gets a thyroid panel, and every time, her T3, T4, and TSH levels were all normal. She always realizes sheepishly that she should cut back on her junk food and exercise more. Relatable! Treatment The treatment for hypothyroidism is synthetic thyroid hormones, including levothyroxine (Synthroid, T4) and liothyroxine (Cytomel). These medications replace the thyroid hormones that the body is not producing enough of. The patient will need to take this medication as a lifelong treatment. It’s important that this medication is taken on an empty stomach, so give this medication in the morning with a full glass of water, 30-60 minutes before a meal. Levothyroxine is one of the essential medications you need to know for your Pharm exams and it’s covered in our Pharmacology flashcards. Coordinating these early medications In Cathy’s experience at the hospital, thyroid medications are usually scheduled for 6 AM. Cathy needs to wake these patients up at 6 AM with this medication and a full glass of water. Sometimes patients are not happy about this! So she came up with a strategy. If the patient with hypothyroidism needs labs drawn in the morning, Cathy coordinates it so they get labs drawn, their vitals taken, and their thyroid medication administered all at once. Then she can leave them alone! Nursing care & patient teaching For patients with hypothyroidism there are some nursing care and patient teaching tactics you can employ. Encourage frequent rest periods (to help with their lethargy). Encourage a low-calorie, high-fiber diet to promote weight loss and prevent constipation. Increase the patient's room temperature and provide blankets (to help with their cold intolerance). This patient will need routine TSH/T3/T4 monitoring to ensure their medications remain therapeutic. The patient will also need to recognize signs of HYPERthyroidism (insomnia, tachycardia, heat intolerance, weight loss), as this can indicate their medication is working too well and needs to be adjusted. MYXEDEMA COMA Hypothyroidism is a disorder you need to know for your Med-Surg classes and exams, and a myxedema coma is a critical care topic that builds on your knowledge of this disorder. Myxedema coma is a life-threatening complication of hypothyroidism known as decompensated hypothyroidism. Though this complication contains the word coma, patients may or may not be actually comatose. Either way, this is a medical emergency. Causes Myxedema coma can be caused by long-term untreated hypothyroidism, abrupt discontinuation of thyroid medication, or infection or illness. It can also be a combination of these. For example, in untreated hypothyroidism, the body comes up with adaptive mechanisms to maintain homeostasis, and if a bad infection occurs, these mechanisms can fail, and the body can fall into myxedema coma. Signs and symptoms The signs and symptoms of myxedema coma are very serious and include hypoxia (not enough oxygen), decreased cardiac output, decreased levels of consciousness (hence coma), bradycardia, hypotension and hypothermia. Nursing care priorities The most important nursing care priority when responding to a myxedema coma is maintaining a patent airway. That’s always the most important priority, which you know from the ABCs of nursing. There’s a chance that this patient will need to be intubated and receive mechanical ventilation, so you will need to assist with that. Monitor the patient’s cardiac rhythm. Administer large doses of thyroid medications, like the aforementioned levothyroxine, as ordered. And you will need to warm this patient, since they have hypothermia with this condition. So with hypothyroidism, we have inadequate production of T3 and T4 which are thyroid hormones in the thyroid gland. In terms of the pathophysiology behind hypothyroidism, causes could include primary, secondary, or tertiary causes. So, just to do a little review here, the hypothalamus produces thyroid-releasing hormone TRH, which causes the pituitary gland to produce TSH or thyroid-stimulating hormone, and that allows the thyroid gland to produce T3 and T4. So with primary hypothyroidism, that's where we have an issue with the thyroid gland itself. So the leading cause of primary hypothyroidism is Hashimoto's disease which is an autoimmune disorder that causes antibodies to attack and destroy the thyroid tissue. So if the thyroid gland is damaged, it can't produce its T3 and T4 like it should. Secondary causes of hypothyroidism is where we have an issue with the pituitary gland, like if there was a pituitary tumor. This decreases production of TSH so the thyroid gland is not getting the message it needs to produce T3 or T4. And then we have tertiary causes of hypothyroidism. So if there is some kind of dysfunction in the hypothalamus then the hypothalamus is not releasing TRH and therefore, the pituitary gland is not releasing TSH, and that is causing inadequate production of T3 and T4. Hopefully that's helpful for you to be able to differentiate the three different causes of hypothyroidism. Now, let's talk about the signs and symptoms of hypothyroidism. This includes hypotension, bradycardia, lethargy, cold intolerance, constipation, weight gain, thin hair, brittle fingernails, as well as depression. In terms of what labs we may see, it really depends on whether we're dealing with primary hypothyroidism or secondary or tertiary hypothyroidism. So with primary hypothyroidism, we have an issue in the thyroid gland itself. So it's been injured, and it's just not able to produce that T3 and T4. However, the pituitary gland is working just fine. So the pituitary gland is desperate to try to get this thyroid gland to produce its T3 and T4. So it's increasing levels of TSH. Be like, "Come on thyroid gland. Here's more TSH. Can you please get going on making your T3 and T4?" And the thyroid gland like, "Sorry, dude. I'm injured. I'm going to chill out. I can't produce any T3 or T4." So labs that you would see with primary hypothyroidism include low levels of T3 and T4 but elevated levels of TSH. On the other hand, if you're dealing with secondary or tertiary hypothyroidism, this means that the thyroid gland itself is working fine but it's not getting the right signal from the pituitary gland. So the pituitary gland is not producing enough TSH and that makes the thyroid gland not produce T3 and T4. So if you look at the labs for secondary hypothyroidism, you're going to have low levels of T3 and T4 but you're also going to have low levels of TSH because there's some kind of pituitary tumor or the pituitary gland is not getting the proper signal from the hypothalamus. If there's a problem with the hypothalamus, that causes decreased TRH, which causes decreased TSH, which causes decreased T3 and T4. Okay? So those are the labs you can expect. Over the years, I've had periods of time where I was feeling like, "Oh, I'm really tired and I'm cold all the time and I've kind of gained some weight. And maybe I have hypothyroidism." And I go and I get that checked out and all the time, my T3, T4, and TSH levels are all normal. So that has never been the problem. It's like, well, maybe I just need to stop eating so much and exercise more. That might work too. So I've never actually had any issues with my thyroid, but I've always suspected that I may have had those issues in the past. Okay. In terms of treatment, we would give them a synthetic form of the thyroid hormones. So this would include levothyroxine or liothyroxine. So you would give this medication not with meals - so like an hour before meals - in the morning with a full glass of water. At the hospital, they always schedule thyroid medications, levothyroxine or liothyroxine, at 6:00 AM. So you get to wake your patient up at 6:00 AM and give them their thyroid medication with a full glass of water. And, boy, are they happy to see you at 6:00 AM. Not. So a lot of times, if they have to have labs in the morning, I try to coordinate it all so they get their labs drawn, we could do their vital signs, and they get their thyroid medication all at once, so then I can leave them alone after that. Okay. In terms of nursing care for a patient who has hypothyroidism, you want to encourage frequent rest periods because they have this lethargy, you want to encourage a low-calorie, high-fiber diet to help promote weight loss and to prevent constipation, and then you want to increase the patient's room temperature and provide blankets because they have this cold intolerance. Okay, finally let's talk about myxedema coma, which is one of our critical care topics here in the MedicalSurgical Deck, Card 36 [Endocrine system]. This is where we have a patient with severe, life-threatening hypothyroidism, and it could be due to the fact that they have untreated hypothyroidism, or they may have abruptly discontinued their thyroid medication, or it could be due to infection or illness. So signs and symptoms are very serious and include hypoxia as well as decreased cardiac output, decreased level of consciousness, bradycardia, hypotension and hypothermia. So in terms of the nursing care priorities, we're going to want to maintain a patent airway, right? So our ABC priorities, airway is most important. There's a chance that this patient will need to be intubated and receive mechanical ventilation, so you're going to want to assist with that. You're definitely going to want to monitor the patient's cardiac rhythm and administer large doses of thyroid medications such as levothyroxine as ordered. And then warm the patient as they will have hypothermia with this condition. Med-Surg Endocrine System, part 15: Hyperthyroidism & Thyroid Storm (Thyrotoxicosis) HYPERTHYROIDISM Hyperthyroidism is a disorder of the thyroid causing excess secretion of thyroid hormones T3 and T4 that causes the body to go into a hypermetabolic state. Similar to hypothyroidism, there are primary, secondary and tertiary causes of hyperthyroidism. TRH, TSH, T3/T4 hormone review If you remember from our overview on thyroid hormones, the hypothalamus produces thyroid-releasing hormone (TRH), which causes the pituitary gland to produce thyroid-stimulating hormone, which prompts the thyroid gland to produce the thyroid hormones T3 and T4. You can think of the chain like this Hypothalamus produces TRH Pituitary gland produces TSH Thyroid produces T3/T4 Pathophysiology of hyperthyroidism To understand the differences between primary, secondary and tertiary hyperthyroidism, you can flip the chain backwards (so that you are starting from the thyroid). Thyroid produces T3/T4 Pituitary gland produces TSH Hypothalamus produces TRH Primary hyperthyroidism In primary hyperthyroidism, there is a problem with the thyroid gland itself that’s causing it to secrete too much T3 and T4. The most common cause is Grave’s disease, an autoimmune disorder. In Grave’s disease, your body creates antibodies that basically trick your thyroid into growing and producing too much T3 and T4. A thyroid nodule (small tumor) can also be an issue that causes excess secretion of T3 and T4 and thus, primary hyperthyroidism. Secondary hyperthyroidism Secondary causes of hyperthyroidism occur when there is an issue with the pituitary gland, like a tumor. This causes excess secretion of TSH. With excess TSH, the thyroid gland thinks it needs to make lots of T3 and T4, even though it doesn’t need to. But the thyroid gland is just taking orders. Throughout the Endocrine system section of this Med-Surg playlist, you’ve learned about multiple diseases where glandular tumors result in excess hormone secretion. Tumors that do this are known as “functioning” tumors, because they are actually taking on a job: making hormones. Sometimes the tumor actually harms the gland in a way where it can’t make enough hormone (e.g., secondary HYPOthyroidism), in that case, it is not a functioning tumor. Tertiary hyperthyroidism Tertiary causes of hyperthyroidism happen when there is a problem in the hypothalamus. Due to some dysfunction, the hypothalamus is producing too much TRH, which is causing the production of too much TSH, which causes the thyroid gland to go into overdrive and produce too much T3 and T4. Again, the thyroid gland is just taking orders! Signs and symptoms The thyroid is responsible for the body’s metabolism, so hyperthyroidism leads to a hypermetabolic state. Signs and symptoms of hyperthyroidism include tachycardia, hypertension, heat intolerance, exophthalmos (bulging eyeballs), weight loss, insomnia, diarrhea, and warm, sweaty skin. If you want to think critically to deduce the signs and symptoms of hyperthyroidism, remember from our hormone overview what T3/T4 controls: T3/T4 controls metabolism. So when those hormones are high, the metabolism goes into overdrive and you see weight loss, warm skin, heat intolerance (feeling too hot) and insomnia (if you are hyper you can’t get to sleep). T3/T4 controls heart function. So when those hormones are high, you see that faster heart function with tachycardia and hypertension. T3/T4 controls digestion. So when those hormones are high, your digestion system is in overdrive too which results in diarrhea. Lab values When it comes to the lab values you might see with hyperthyroidism, you will be looking at T3/T4 and TSH. The measurement of these hormones is known as a thyroid panel, which we explained in video 7 of this series. The thyroid panel and blood glucose labs are the most important endocrine lab values to know for your MedSurg exams, whether a course final, your ATI or NCLEX. Lab values can be dispersed throughout your textbooks, which is why we created our Lab Values flashcards, to keep the most important lab values you need to know for your exams all in one place that’s easy to study! Primary hyperthyroidism: High T3/T4, low TSH Secondary hyperthyroidism: High T3/T4, high TSH Tertiary hyperthyroidism: High T3/T4, high TSH T3/T4 values with hyperthyroidism In all types of hyperthyroidism, you will see increased T3/T4. That’s an easy one, because that’s what this disease is marked by! The expected range for T3 in a thyroid panel is 70 - 204 ng/dL. T3 levels over 204 ng/dL can indicate hyperthyroidism. The expected range for T4 in a thyroid panel is 4 - 12 mcg/dL. T4 levels over 12 mcg/dL can indicate hyperthyroidism. TSH values with hyperthyroidism The TSH value you will get back in a thyroid panel for hyperthyroidism really depends on if you are looking at primary, secondary, or tertiary hyperthyroidism With primary hyperthyroidism, remember there is an issue in the thyroid gland itself causing excess production of T3/T4. However, the pituitary gland is functioning fine in this scenario, and its job is to scale back TSH production to prompt the thyroid to scale back T3/T4. The pituitary gland is scaling back, but the thyroid is not responding. So with primary hyperthyroidism, you will see decreased levels of TSH. The expected range for TSH in a thyroid panel is 0.5 - 5.0 mU/L. TSH levels less than 0.5 mU/L can indicate primary hyperthyroidism. With secondary or tertiary hyperthyroidism, the pituitary gland is in overdrive (by itself, or because of a dysfunctional hypothalamus) and therefore producing too much TSH — and that's what's prompting the thyroid to make too much T3/T4. So with secondary or tertiary hyperthyroidism, you will see increased levels of TSH. TSH levels over 5 mU/L can indicate secondary or tertiary hyperthyroidism. Treatment of hyperthyroidism If a patient has primary hyperthyroidism, they may need a thyroidectomy, which is a removal of the thyroid gland. We go into more detail about a thyroidectomy in Video 16 of this series. After the thyroid is removed, the patient will be sent into HYPOthyroidism, and will require lifelong hormone replacement therapy with levothyroxine. Some medication options for hyperthyroidism are propylthiouracil (PTU), a strong iodine solution, and beta blockers. PTU blocks synthesis of thyroid hormones, and an iodine solution is absorbed by the thyroid gland to inhibit thyroid hormone production and release. Beta blockers like metoprolol and propranolol can be used to bring down the high blood pressure and heart rate side effects that are seen with this disease. If you need help remembering these medications for Med-Surg or Pharmacology, they are covered in our Pharmacology Flashcards! Nursing care If you have a patient with hyperthyroidism, you will want to increase their calorie and protein intake to offset the weight loss they are experiencing. The protein is important since that hypermetabolic state can reduce muscle mass. Make sure to monitor this patient’s input and output, their weight, and their vital signs. For a hyperthyroidism patient with exophthalmos, you will tape their eyelids closed for sleep so their eyes don’t dry out. You definitely want to explain this to the patient carefully because it can be scary when you wake up and your eyes don’t open! You will also provide eye lubricant to help protect the eyes. THYROTOXICOSIS (THYROID STORM) Hyperthyroidism is a disorder you need to know for your Med-Surg classes and exams, and a thyroid storm is a critical care topic that builds on your knowledge of this disorder. Thyrotoxicosis is an acute, life-threatening complication of hyperthyroidism known as a thyroid storm, with extremely high levels of thyroid hormones. This is usually brought on by infection, stress, diabetic ketoacidosis (DKA), or even after a thyroidectomy. Signs and symptoms Signs and symptoms of thyrotoxicosis include severe hypertension, chest pain, dysrhythmias, and dyspnea (difficulty breathing) due to respiratory exhaustion. Treatment A patient undergoing thyroid storm can be given beta blockers to get the vital signs under control, antithyroid medications to stop the problem at the source, and antipyretics (anti-fever medication) like acetaminophen to bring the fever down. Nursing care Because a patient in thyrotoxicosis is having trouble breathing, your most important nursing priority becomes maintaining a patent airway. Then, monitor this patient for dysrhythmias. With hyperthyroidism, we have excess secretion of T3 and T4 from the thyroid gland, and just like we saw with hypothyroidism, we have primary, secondary, and tertiary causes of this disorder. And if you recall, the hypothalamus produces TRH, thyroid-releasing hormone which causes the pituitary gland to produce TSH, thyroid-stimulating hormone and that allows for secretion of T3 and T4 from the thyroid gland. If we have an issue with the thyroid gland itself - so that would be primary hyperthyroidism - the most common cause is Grave's Disease which is an autoimmune issue, but we can also have some kind of thyroid nodule. Due to one of these causes, we have hypersecretion of T3 and T4. So that's primary hyperthyroidism. With secondary hyperthyroidism, this is where we have some kind of pituitary disorder such as a tumor, which is causing excess secretion of TSH. So with all this extra TSH, the thyroid gland is getting the message to produce more and more thyroid gland hormones even though it doesn't really need to, but that's the order it's getting from the pituitary gland. And then with tertiary hyperthyroidism, that means we have an issue in the hypothalamus. So due to some kind of hypothalamus dysfunction, the hypothalamus is producing too much TRH, which is causing the production of too much TSH, which is causing the thyroid gland to go into overdrive, producing all that T3 and T4 even though it really isn't supposed to just because it's getting that order from above. So those are the three causes of hyperthyroidism. So with all that T3 and T4 being produced by the thyroid gland, it really puts the body into a hypermetabolic state. So signs and symptoms of hyperthyroidism include tachycardia, hypertension, heat intolerance, bulging eyeballs, which is something called exophthalmos, weight loss without trying, insomnia, diarrhea, and warm, sweaty skin. In terms of the labs we'll see with hyperthyroidism, T3 and T4 levels will be elevated. TSH levels will depend on whether we're talking about primary or secondary hyperthyroidism. So with primary hyperthyroidism, that's where we have Graves' disease or a thyroid nodule, that thyroid gland is just cranking out the T3 and T4 regardless of how much TSH it's getting. The pituitary gland's over here really concerned, like, "Wow, you're putting out a lot of T3 and T4. Can you please chill out?" And the thyroid gland's like, "I can't chill out. I got to keep making my T3 and T4." So the pituitary gland is scaling back how much TSH it gives the thyroid gland, but the thyroid gland doesn't care. Doesn't care and is going to keep cranking that stuff out as fast as it can. So with primary hyperthyroidism, elevated T3 and T4 but decreased TSH because that pituitary gland is trying to rein that thyroid gland in. When we have secondary or tertiary hyperthyroidism, then our levels of TSH will be increased, right, because there's some kind of tumor or malfunction which is causing increased TSH, which is causing the thyroid gland to produce more T3 and T4. So the thyroid gland is functioning fine. He's like, "I think I'm making enough T3, T4 here." But the pituitary gland's going crazy and is like, "No. Here's some more TSH. Make more. Make more." And the thyroid gland's like, "Okay, I'll do that." And that's secondary hyperthyroidism. So with that, we'll have elevated TSH and elevated T3 and T4. Let's move to treatment. If a patient has primary hyperthyroidism, they may need a thyroidectomy, which is removal of the thyroid gland. And in my next video, we will talk about nursing care of patients who have to undergo a thyroidectomy. Medications that could be used include PTU, iodine solutions, as well as beta-blockers to help bring those vital signs down. In terms of nursing care, we're going to want to increase our patient's calorie and protein intake because of that weight loss and the fact that they're in this hypermetabolic state. We're going to want to monitor their I's and O's as well as their weight and their vital signs. And then for exophthalmos, which is the bulging eyes, we're going to want to tape their eyelids closed for sleep and provide eye lubricant to really protect those eyes. Let's briefly talk about a life-threatening complication of hyperthyroidism which is thyrotoxicosis, or a thyroid storm. This is where we have excessively high levels of thyroid hormones. And this could be brought on due to infection, stress, diabetic ketoacidosis, which is DKA, or possibly due to a thyroidectomy. In terms of signs and symptoms of this disorder, we're going to have severe hypertension as well as chest pain, dysrhythmias, dyspnea, which is difficulty breathing, delirium, fever, and nausea and vomiting. In terms of treatment, we can give this patient beta-blockers to try to get those vital signs in control, antithyroid medications, as well as antipyretics for treating the fever. And in terms of nursing care, we're definitely going to want to maintain a patent airway, which is always your number-one priority, and then also monitor the patient for dysrhythmias. Med-Surg Endocrine System, part 16: Thyroidectomy: Nursing Care NURSING CARE Any time you have a patient who has had a surgery on their neck (like a thyroidectomy), consider it a serious threat to their airway! Assess for any laryngeal edema (which could manifest with stridor), and intervene rapidly if you identify that. Make sure to have easy access to a crash cart, oxygen delivery devices, and an emergency tracheostomy kit. Patient positioning When a patient comes back from having their thyroidectomy surgery, place them in a semi-fowler’s position. Sitting totally upright would put the patient at a 90 degree angle, but in a semi-Fowler’s position they are angled between 15 and 45 degrees. Support their head and neck using either sandbags or pillows to keep everything in a neutral position. You don’t want the patient to hyperextend their neck by bending it too far backwards, or have their head droop down in front. Keep the patient’s head at the midline to avoid disrupting the suture line across their throat. Bleeding Lots of blood flows through the thyroid gland, and bleeding is a potentially life-threatening complication after a thyroidectomy. You will want to be monitoring your patient carefully for bleeding following this surgery. Check their wound dressing for blood, and check behind their neck to make sure blood is not pooling behind them Parathyroid damage Remember from our anatomy overview of the Endocrine system that the parathyroid glands are 4 glands that basically bedazzle the thyroid gland. The parathyroid glands’ job is to secrete parathyroid hormone (PTH), which causes increased calcium levels. These glands are tiny, the size of a grain of rice, and are somewhat in-the-way during a thyroidectomy and sometimes they get accidentally nicked or damaged during the surgery. So if the parathyroid glands, whose job it is to indirectly increase blood calcium, get damaged and are unable to do their job, calcium will not be increased to the level it should, and this will result in hypocalcemia. Hypocalcemia Calcium is an important electrolyte in the body, and the normal level of calcium (Ca) in the blood is 9-10.5 mg/dL. Calcium levels under 9 mg/dL can indicate hypocalcemia. Besides hypoparathyroidism resulting from parathyroid gland damage, other causes of hypocalcemia can be diarrhea (causes electrolyte loss) and vitamin D deficiency (because vitamin D helps the body absorb calcium). Signs and symptoms of parathyroid damage are signs and symptoms of hypocalcemia, which includes numbness, tingling around the mouth, muscle twitching, GI upset, and positive Chvostek’s and Trousseau’s signs. Chvostek’s sign A Chvostek’s sign is an abnormal reaction to the stimulation of the facial nerve. If you tap the patient’s cheek and their face twitches, this is a positive Chvostek’s sign and can indicate the patient has hypocalcemia. Cathy’s easy way for remembering this is that both Chvostek and cheek start with CH! Trousseau’s sign Trousseau’s sign is an abnormal reaction by the hand, to pressure on the arm. If you inflate a blood pressure cuff on a patient’s upper arm and it causes spasms in their hands and fingers due to ischemia, that can indicate hypocalcemia. Treatment If a patient does have hypocalcemia that is confirmed with a blood test, we can provide them with calcium gluconate to bring the calcium level up. PATIENT TEACHING After a patient undergoes a thyroidectomy, it’s important to teach them to avoid extreme neck extension or flexing, and to keep their head in a midline position. Otherwise, they risk damage to that suture line. As part of patient teaching post-thyroidectomy, you will also need to reinforce that the patient will need to take thyroid replacement for the rest of their lives. Their thyroid gland is now gone, so it will not be producing thyroid hormones T3 and T4 anymore. The thyroid hormone replacement medication is levothyroxine, which is given on an empty stomach with a full glass of water. So after your patient comes back from the OR, from having their thyroidectomy, you want to place your patient in a semi-Fowler's position. And then you want to support their head and neck using either sandbags or pillows to keep it in a neutral position. So we don't want them to hyper-extend their neck or have their neck go down like this. We really want to support it and keep it midline to avoid disruption of the suture line. We're going to want to monitor for bleeding, so we're going to want to check their dressing and also check behind their neck to make sure there's no blood pooling behind their neck. And then we also want to monitor for signs and symptoms of parathyroid damage. During a thyroidectomy, the parathyroid gland can be damaged as well which can cause hypocalcemia. So signs and symptoms of parathyroid damage are going to be signs and symptoms of hypocalcemia. This includes numbness and tingling around the mouth as well as muscle twitching. You also may have a positive Chvostek sign. So the Chvostek sign is where you tap the cheek and that's how I remember this sign because Chvostek starts with C-H, and cheek also starts with C-H. So you tap their cheek and if you get twitching of the facial muscles, then that is a positive Chvostek sign and they indicate that the patient has hypocalcemia. Also if they have a positive Trousseau's sign that is also indicative of hypocalcemia. So that's where you inflate a blood pressure cuff on their upper arm, and it causes spasms in their hand and fingers. It causes their hands and fingers to kind of go like this due to the ischemia. So if your patient is exhibiting that, then that is definitely a strong indicator that they may have sustained parathyroid gland damage. And then if your patient does have hypocalcemia that's confirmed with a blood test, then we can provide them with calcium gluconate to help address that. In terms of patient teaching, we want to reinforce that they need to avoid extreme neck extension or flexing, right? They want to keep their head in a midline position. You also need to reinforce that the patient will need to take thyroid replacement for the rest of their lives, right? The thyroid gland is gone, so it is not going to be producing T3 and T4. So the patient will need to take a medication such as levothyroxine every day for the rest of their lives. And just as a reminder about that medication, we do give that on an empty stomach, about an hour before breakfast with a full glass of water. Med-Surg Endocrine System part 17: Hypoparathyroidism and Hyperparathryoidism REVIEW OF PARATHYROID HORMONE & PTH In video 2 of our Med-Surg Endocrine system playlist, we taught you about the parathyroid glands.You have four parathyroid glands, and they are right next to/on top of the thyroid gland. You can think of the parathyroid glands as bedazzling the thyroid gland. The parathyroid glands’ main function is to release parathyroid hormone (PTH). Remember that the endocrine system and its negative feedback loops seek homeostasis with different hormone levels, wanting to get levels not too high, not too low, but just right (think of the baby bear in Goldilocks and the Three Bears). PTH’s goal is to keep calcium at the appropriate level by increasing it, and it does this in three ways: PTH pulls calcium from the bones into the bloodstream. PTH causes increased reabsorption of calcium at the kidneys. Increasing reabsorption at the kidneys means you don’t lose as much calcium via urination. PTH causes increased absorption of calcium from food in the intestines. HYPOPARATHYROIDISM Hypoparathyroidism is decreased or insufficient secretion of PTH. Since PTH’s main function is to increase calcium levels in the body, when the parathyroid glands are functioning normally, calcium will be at the correct level. When PTH is too low, blood calcium levels will also be low. Causes Hypoparathyroidism most often occurs after damage to the parathyroid glands during a thyroidectomy. A thyroidectomy is that complete or partial removal of the thyroid gland that we discussed in our last article. If you remember how the parathyroid glands are bedazzling the thyroid, and know that they are about as small as grains of rice, and they can be really hard to avoid during that thyroidectomy surgery, so sometimes they get accidentally damaged, or even removed. Signs and symptoms The signs and symptoms of hypoparathyroidism are the signs and symptoms of hypocalcemia (low calcium levels), which include numbness, tingling around the mouth, muscle twitching, GI upset, and positive Chvostek’s and Trousseau’s signs. Hypocalcemia can result in more severe side effects too, like seizures, dysrhythmias, and tetany. Tetany is a symptom marked by involuntary contraction and spasming of the muscles. Tetany is not related to tetanus, which is an infectious disease that we get vaccinated against. The two do share the same root, “tet,” which means tension (as in a muscle). Lab values The lab values that you need to know about for hypoparathyroidism are: Decreased PTH Decreased calcium (hypocalcemia) Increased phosphorus (hyperphosphatemia) The normal level of calcium (Ca) in the blood is 9 - 10.5 mg/dL. Calcium levels under 9 mg/dL can indicate hypocalcemia. Phosphorus (P) Phosphorus (P) is a lab value you should be familiar with for your nursing exams. The normal level of phosphorus (P) in the blood is 3.0 - 4.5 mg/dL. Hyperphosphatemia Phosphorus levels above 4.5 mg/dL can indicate hyperphosphatemia. Hyperphosphatemia can also be caused by kidney disease, and its symptoms are the same as hypocalcemia: muscle spasms, numbness, tingling. Calcium and phosphorus have an inverse relationship in the body. When we have high levels of calcium, we have low levels of phosphorus, and when we have low levels of calcium, we have high levels of phosphorus. That’s why the symptoms of hyperphosphatemia and hypocalcemia are the same. Treatment (medications) There are several medications that can be used to treat hypoparathyroidism, including vitamin supplements. A patient with hypoparathyroidism can be given calcium gluconate, which is usually administered with a vitamin D supplement because vitamin D is essential for allowing absorption of calcium. Phosphate binders can also be given, to help bring the phosphorus levels down. Nursing care When you have a patient with hypoparathyroidism, you may need to implement seizure precautions because of the risk of seizures associated with hypocalcemia. You will follow your facility’s procedure, but that usually includes padding the side-rails of the bed and making sure oxygen equipment is available. A patient with hypoparathyroidism will need a high-calcium, low-phosphorus diet, and can be given their phosphate binders with their meals. HYPERPARATHYROIDISM Hyperparathyroidism is a disorder of the parathyroid glands resulting in hypersecretion, or excess secretion, of parathyroid hormone (PTH) resulting in excess blood calcium levels. Causes The primary cause of hyperparathyroidism is an adenoma (benign tumor) on the parathyroid gland that causes excess secretion of PTH. Remember that a primary cause is when the problem is local to the organ in question and not caused by something somewhere else in the body. A secondary cause of hyperparathyroidism is kidney disease. With kidney disease, calcium levels are low. This is because healthy kidneys help activate vitamin D (which helps calcium absorption) and remove extra phosphorous (which allows more calcium in the blood). When kidneys are diseased, they can’t perform that function as well, and the body is not able to get calcium levels up where they should be, resulting in hypocalcemia. But remember, PTH’s job is to get calcium to a normal level. So in response to calcium being low, the parathyroid glands go into overdrive producing excess PTH. Signs and symptoms The signs and symptoms of hyperparathyroidism are the signs and symptoms of hypercalcemia, which includes fatigue, muscle weakness, bone pain and deformities (because calcium is being pulled out of bones), nausea and vomiting, weight loss, constipation, hypertension, kidney stones, depression or other behavioral changes and dysrhythmias. Lab values The lab values that you need to know about for hyperparathyroidism are: High PTH High calcium (hypercalcemia) Low levels of phosphorus (hypophosphatemia) The normal level of calcium (Ca) in the blood is 9 - 10.5 mg/dL. Calcium levels over 10.5 mg/dL can indicate hypercalcemia. The normal level of phosphorus (P) in the blood is 3.0 - 4.5 mg/dL. Phosphorus levels below 3 mg/dL can indicate hypophosphatemia. These labs are covered in our Lab Values flashcards, which help you keep the most important labs for your exams all in one place. Treatment For patients with hyperparathyroidism, there are several types of treatments available, including medications to control symptoms, as well as surgical interventions. One medication option is the loop diuretic Lasix (furosemide), which helps increase the excretion of calcium through urine, and bring blood calcium levels down. Another medication for hyperparathyroidism is calcitonin, which prevents calcium extraction from bones by inhibiting osteoclast activity, and increases kidney excretion of calcium. Calcitonin helps tone down calcium in the blood! And finally, patients can be given phosphates to bring their phosphorus levels up. Need help remembering these medications for Med-Surg or Pharm? They’re covered in our Pharmacology flashcards for nursing students so you can memorize them easily. Surgery might be needed if the patient has an adenoma on their parathyroid gland (that primary cause of the disorder). The surgery to remove the parathyroid glands is called a parathyroidectomy, which is thankfully a pretty easy one to remember! Nursing care for hyperparathyroidism Fragile; handle with care! If you have a patient with hyperparathyroidism, you will want to implement safety precautions. This patient is literally fragile— their excess levels of PTH causes calcium to be pulled out of the bones. Remember how we need calcium to build strong bones? Well, without the needed calcium, this patient’s bones are weak and brittle. If they were to fall, there could be some tragic consequences. You will want to provide for patient safety, assist the patient with ambulation, and make sure they don’t fall! A patient with hyperparathyroidism should eat a low-calcium, high-phosphorus diet, and increase their fluid intake to prevent constipation and the risk of kidney stones. These parathyroid glands release PTH. PTH causes increased calcium levels in the bloodstream, and it does this three ways. One is it pulls calcium out of the bones into the bloodstream. It also causes increased reabsorption of calcium at the kidneys, and it causes increased absorption of calcium in the intestines, and that's how it brings those calcium levels up in the bloodstream. With hypoparathyroidism, we have decreased or insufficient secretion of PTH, and this causes those calcium levels to go down, because those parathyroid glands are not working correctly. And the main cause of this issue is that during a thyroidectomy, which is removal of the thyroid gland, we have nicked and damaged those parathyroid glands, and when we damage them, they don't produce their PTH, and causes those calcium levels to come down. In terms of signs and symptoms of this disorder, if we have hypoparathyroidism, we're basically going to see the same signs and symptoms we would see for someone who has hypocalcemia, so low levels of calcium. So this includes muscle cramps, numbness and tingling, a positive Chvostek's sign, as well as a positive Trousseau's sign. We may also see tetany or seizures and possibly dysrhythmias as well. In terms of labs, when we have hypoparathyroidism we will have decreased PTH. So decreased parathyroid hormone. In addition, we will have hypocalcemia, so levels of calcium will be under 9. And then we will have hyperphosphatemia. So you may recall, when we have high levels of calcium, we'll have low levels of phosphorous, and the opposite is true too. If we have high levels of phosphorous, we have low levels of calcium. They have this inverse relationship. So with this disorder, we'll have hypocalcemia, but hyperphosphatemia. In terms of treatment, we would provide a patient with this disorder with calcium gluconate, so we want to try to get those calcium levels up. We would give them calcium as well as Vitamin D supplements because Vitamin D is essential to allow for the absorption of calcium. And then we can also give them phosphate binders to help bring those phosphorous levels down. In terms of nursing care, we're going to want to implement seizure precautions because of the risk of seizures. So we're going to pad those side-rails of the bed and make sure we have oxygen equipment available at the bedside, etc. We're going to provide the patient with a high-calcium, low-phosphorous diet. And then also give the patient phosphate binders with their meals. Now let's talk about hyperparathyroidism. This is where we have hypersecretion, excess secretion, of PTH from the parathyroid glands. And this may be due to primary or secondary causes. The primary cause would be an adenoma which is a benign tumor on the parathyroid gland that causes excess secretion of PTH. One of the secondary causes of hyperparathyroidism would be kidney disease. So with kidney failure or kidney disease, we have hypocalcemia. So our calcium levels are very low. And the parathyroid glands, they sense that and they're trying to compensate. So they pump out all this extra PTH to bring up those calcium levels. And in the process, when we have all that PTH, that pulls calcium out of the bones, into the bloodstream. And those levels just keep coming up. In terms of labs, we would see high levels of PTH, high levels of calcium, and low levels of phosphorus. For signs and symptoms, the signs and symptoms of hyperparathyroidism are going to be consistent with the signs and symptoms of hypercalcemia. So this includes fatigue, muscle weakness. We also may see bone pain and deformities, because we're pulling all that calcium out of the bones. Nausea and vomiting, weight loss, constipation, hypertension as well as kidney stones and dysrhythmias are also possible side effects. In terms of treatment, medications we can use include furosemide, which is Lasix. That helps to increase excretion of calcium, and bring those blood levels down. We can also give a patient calcitonin. So if you recall, calcitonin helps to tone down calcium levels in the bloodstream. And then we can also give the patient phosphates to help bring those phosphorus levels up. Surgery may also be needed if the patient has an adenoma. If they have the primary cause of hyperparathyroidism. So they may need a parathryoidectomy, so removal of the parathyroid gland. And then in terms of nursing care, we're going to want to implement safety precautions for this patient, because the excess levels of PTH is causing calcium to be pulled out of the bones, those bones are going to be really weak and fragile. And so if that patient were to fall, then it could be really tragic. So we're definitely going to want to provide for patient safety, assist the patient with ambulation, make sure they do not fall. We also want to provide the patient with a low-calcium, high-phosphorus diet, and increase their fluid intake as well, to help prevent that constipation as well as the risk for kidney stones. Med-Surg Endocrine System part 18: Diabetes Mellitus DEFINIT ION OF DIABETES Diabetes causes chronic hyperglycemia (increased blood sugar levels) due to EITHER: insufficient insulin production by the pancreas, or insulin resistance of the cells in the body. If you remember from our insulin overview earlier in this series, insulin’s job is to transport glucose from the bloodstream into the body’s cells where it can be used for energy. This is another classic example of the endocrine system’s attempt to reach homeostasis in the body via a negative feedback loop: when the body senses that blood glucose levels are rising, the beta cells in the pancreas (islets of Langerhans) release insulin to help bring that glucose down. You can think of insulin as an escort, helping to bring glucose from the bloodstream into the cells. Some students also find it useful to think of insulin as a key. Insulin acts like a key by opening the doors of the cells so glucose can enter. If you don’t have an escort, you can’t find your seat, and if you don’t have your keys, you can’t get in the door. If there’s not enough insulin, then glucose can’t get into the cells to be used for energy, and it builds up in the bloodstream TYPES OF DIABETES Type 1 diabetes In type 1 diabetes, an autoimmune dysfunction destroys beta cells in the pancreas, and this leads to a lack of insulin secretion by the pancreas. Patients with type 1 diabetes are insulin dependent and will require insulin for the rest of their lives in order for the glucose to get from their bloodstream into the cells. Type 1 diabetes used to be known as juvenile diabetes because it is most often discovered in children, but it was renamed because it can strike adults too. Type 2 diabetes In type 2 diabetes, we see progressive insulin resistance and decreased insulin production from the pancreas. Progressive insulin resistance means that insulin’s effectiveness at transporting glucose decreases over time — insulin becomes less effective. This usually occurs in adults, but there have been increasing cases of children with type 2 diabetes. Note: Cathy uses the phrase “juvenile diabetes” in this video when she refers to childhood-onset type 2 diabetes, not the former name for type 1 diabetes. Risk factors The risk factors that are associated with type 2 diabetes are: obesity, inactivity, hypertension, hyperlipidemia (high cholesterol), smoking, genetics, and race and ethnicity. Patients who are Black, Latino, or Native American are statistically at a higher risk for diabetes. It is important to note the word statistically. Race does not play a biologically predetermined role in this disease, but the risks are higher statistically for communities of color for a variety of reasons, including the social and environmental determinants of health — financial resources; access to adequate and nondiscriminatory health care; access to education; and more. Gestational diabetes Gestational diabetes occurs when the placental hormones during a pregnancy counteract insulin, and this results in glucose intolerance during pregnancy. SIGNS AND SYMPTOMS OF DIABETES The most notable and memorable signs and symptoms of diabetes are known as The Three Ps: polydipsia, polyphagia, and polyuria. Poly means multiple or many, dipsia is thirst, phagia is hunger, and uria means urine. This prefix and these root words are covered in our Medical Terminology flashcards, which we designed to equip you with the ability to translate any unfamiliar medical term you encounter! Other symptoms of diabetes include: Weight loss. Although patients experience excessive hunger, they still lose weight because without insulin, the food they’re eating doesn’t enter the cells and they are basically starving even though they are eating. Warm skin Dehydration, which also causes: Dry skin Weak pulses Decreased skin turgor (skin is not elastic, when you pinch the skin and release it stays pinched and does not snap back in place) Fruity-smelling breath (that’s the glucose!) Kussmaul respirations (increased rate and depth of respirations) are seen in Diabetic Ketoacidosis (DKA) as a compensatory mechanism to attempt to correct metabolic acidosis by blowing off excess carbon dioxide. Nausea and vomiting Weakness Lethargy DIABETES DIAGNOSIS Remember from our prior video that blood glucose lab values, especially as they pertain to diabetes, are VERY important to know for your Med-Surg exams and in nursing practice. If a patient has two or more of the following labs on separate days, then that can indicate diabetes: Casual blood glucose over 200.This test measures blood sugar regardless of when the patient last ate, and it’s also sometimes known as a random blood sugar test. This test can be useful because blood glucose levels in non-diabetic don’t vary that wildly throughout the day, so amounts that vary wildly can indicate a problem. Fasting blood glucose over 126.This test is useful to get a baseline of what a patient’s glucose is when their body is not digesting anything, and is usually done first thing in the morning. Glucose over 200 with an oral glucose tolerance test (OGTT).The OGTT measures the patient’s blood sugar level initially, they are given a glucose solution to drink, and then the blood sugar is measured again (sometimes multiple times). The point of this test is to see how the body processes sugar in real time. HgB A1c over 6.5%.This test gives a longer term picture, kind of like the drug tests that are done on hair follicles! This test measures the patient’s average blood sugar level for the past two to three months. It’s actually measuring what percentage of your hemoglobin is coated with sugar TREATMENT The treatment for Type 1 diabetes is insulin. If your patient has type 1 diabetes, they will need that insulin for the rest of their life since their pancreas does not make enough. If your patient has type 2 diabetes, they may require insulin, but they will likely begin treatment with oral antidiabetic medications. These oral antidiabetics aren’t insulin replacements; they are more like insulin encouragers. This means that these medications don’t work for type 1 diabetics, because their insulin cannot be encouraged. They simply can’t make it, and require outside insulin. When you treat diabetes, the goal is to get the Hgb A1c under 7%. FOOT CARE Foot care is very important for diabetic patients. Cathy, as a wound nurse herself, has seen many diabetic foot ulcers that have unfortunately led to amputations. The feet of a diabetic patient can be injured easily for several reasons. Diabetes can cause neuropathy that prevents the patient from feeling sensation in their feet. Because we walk around all day, feet are more at risk than other body parts of being injured, and without sensation, you don’t feel pain when injured, so you may be carrying on with an injured foot and not know it! Think about it: if you were to step on a nail, you’d want to know about it immediately! The second reason is that diabetes can cause reduced blood flow to the feet, which makes it harder for injuries or infections to heal. So if this patient does injure their feet, it takes a lot longer to heal. Here is some foot care teaching you want to provide your diabetic patient: Patients should inspect their feet daily using a mirror, Check their shoes for objects before putting their feet in, Apply moisturizer to combat dry skin, but not between the toes because it can result in Athlete’s foot (a fungal infection), Wear cotton socks as opposed to synthetic socks, Wear closed-toe shoes to protect against injuries (think of it as a helmet for your feet!), Avoid hangnails and the resulting infections by cutting toenails straight across rather than rounding, Don't use over-the-counter products for corn or callus removal, Avoid using heating pads on their feet, as they might not be able to feel it if it was burning them. ILLNESS CARE When patients with diabetes get sick, they are much more likely to have life-threatening complications, like diabetic ketoacidosis (DKA). Here are some special instructions to provide your patient about caring for themselves when they are sick: Monitor their blood glucose levels more frequently Don’t skip insulin Test their urine for ketones, which are an indicator of DKA Drink 3L water per day to avoid dehydration Notify their provider if: Illness lasts for more than 1 day Temperature over 101.5℉ or 38.6℃ Blood glucose over 250 Urine positive for ketones Diabetes causes chronic hyperglycemia, so increased blood glucose levels, due to insufficient insulin production by the pancreas and/or insulin resistance of the cells in the body. So insulin is kind of like an escort, and it helps to bring glucose from the bloodstream into the cells. So if there's not enough insulin, then glucose can't get it to the cells and it builds up in the bloodstream. So there are three types of diabetes, type 1, type 2, and gestational diabetes. With type 1, we have destruction of the beta cells in the pancreas due to an autoimmune dysfunction, and this leads to a lack of insulin secretion by the pancreas. So patients with type 1 diabetes, they are insulin dependent. They will require insulin for the rest of their lives in order for that glucose to get from the bloodstream into the cells. Then we have type 2 diabetes. This is where we have progressive insulin resistance and decreased insulin production from the pancreas. And this typically occurs later in life, but not always. So we definitely are seeing increased incidences of juvenile diabetes. Risk factors associated with type 2 diabetes includes obesity, inactivity, hypertension, hyperlipidemia, smoking, genetics, and race. So patients that are African American, Hispanic, or American Indian, they are definitely at higher risk for diabetes. The third type of diabetes is gestational diabetes. So this is where the placental hormones counteract insulin, and this results in glucose intolerance during pregnancy. Alright. Now, let's talk about the signs and symptoms of diabetes, which are basically the signs and symptoms of hyperglycemia. There's a lot to remember but they're all here on the back of card 44 [of the Endocrine system section in the Medical-Surgical Flashcard deck]. Let's first talk about the three P's, polydipsia, polyphagia, and polyuria. Poly means a lot or many. So with diabetes, we're going to have a lot of thirst, a lot of hunger, and a lot of urine. Other symptoms include weight loss, warm and dry skin. So the way I remember the skin symptom is, "Warm and dry, sugar's high. Cold and clammy, needs some candy." So we'll talk about that cold and clammy skin when we cover hypoglycemia, but for hyperglycemia, the skin will be warm and dry. Other symptoms include dehydration - which you may see weak pulses and decreased skin turgor in a patient with dehydration - fruity breath, Kussmaul respirations. So with Kussmaul respirations, we have increased rate and depth of respirations. Other signs and symptoms include nausea and vomiting, weakness, and lethargy. So in terms of diagnosis of diabetes, if the patient has two or more of the following labs on separate days, then that is indicative of diabetes. So these labs include a casual blood glucose over 200, a fasting blood glucose over 126, glucose over 200 with an oral glucose tolerance test or an Hgb A1c over 6.5%. So again, if they have two or more of those over separate days, then they would be diagnosed with diabetes. In terms of treatment, insulin is definitely an important one to remember. If your patient is type 1, that is all they're going to be getting, right? They're insulin dependent. Type 1 diabetic patients cannot take oral diabetic medications. They require insulin. If your patient is type 2, they can take insulin, but they can also receive oral antidiabetic medications. So when we are treating diabetes, our goal is to try to get the Hgb A1c under 7%. So that Hgb A1c result really tells us a lot about the patient's blood glucose levels over the past two, three months, as opposed to just doing a spot check on the blood glucose. It just tells you how that glucose is doing right then and there. That Hgb A1c is a more indicative result on how the patient has been managing their diabetes over the last several months. So that's going to be an important one to watch for, and our goal is to get that under 7%. Alright. So finally, let's talk about foot care and illness care, which are some important teaching you'll need to provide your diabetic patient. With foot care, as a wound nurse, I see lots and lots of diabetic foot ulcers that often lead to amputations. It's a huge complication of diabetes, so we need our diabetic patients to take care of their feet. So some of the education you should provide your diabetic patients include that they need to inspect their feet daily. Using a mirror, they should always check their shoes for objects before putting their feet in there because that can cause damage. They should apply moisturizer to their feet but not between the toes because putting it between the toes can result in athlete's foot, which is basically a fungal infection. They should wear cotton socks, as opposed to synthetic socks, and they definitely need to wear closed-toe shoes. So they should not go barefoot or wear open-toed shoes, and their shoes need to be fitted properly. Ideally, they would go see their podiatrist and get some special properly-fitted shoes to help protect their feet. They should cut their toe nails straight across. They shouldn't round them on the sides because that can cause hangnails, which can lead to really complicated infections. They should also not use over-the-counter products for corn or callus removal. And then finally, they should not use heating pads on their feet because diabetic patients have decreased sensation in their extremities. So if that heating pad is too hot, it can burn them and cause damage. And they won't even know because they can't really feel it. In terms of illness care, this is definitely important. So I share an office with the diabetic educators at my hospital. And when patients get sick, they are much more likely to have life-threatening complications such as diabetic ketoacidosis, or DKA. When your patient is sick, they need to monitor their blood glucose levels more frequently. They should not skip insulin when they're sick. And they also need to test their urine for ketones because if there is ketones in the urine, that could indicate that they have DKA. Also, when the patient is sick, it's important to prevent dehydration. So they should drink about 3 liters of water per day to prevent that dehydration. And then they should notify their provider if their illness lasts for more than one day, if they have a temperature over 38.6 degrees Celsius, if their blood glucose levels are over 250 or if their urine is positive for ketones. Med-Surg Endocrine System, part 19: Diabetes Complications - Hypoglycemia, DKA, HHS HYPOGLYCEMIA Hypoglycemia is a common complication seen in patients with diabetes wherein blood glucose levels drop below 70 mg/dL. You might remember from our endocrine lab values overview that the normal blood glucose levels are between 70 and 140 mg/dL, depending on the type of test. Values lower than 70 mg/dL indicate hypoglycemia. Causes of hypoglycemia There are a variety of reasons that a patient with diabetes can enter into hypoglycemia. A patient might become hypoglycemic because of excess insulin, not enough food intake, too much exercise, or alcohol consumption. Excess insulin medication can lead to low blood sugar because if you remember, insulin is the escort that takes glucose to the cells to be used as energy, so when the body has excess insulin, it’s removing too much glucose and the glucose levels will drop, causing that hypoglycemic state. Check out our overview of insulin medications, including rapid-acting, short-acting, intermediate-acting, and long-acting. These medications are covered in our Pharmacology Flashcards for Nursing Students. If a patient skips a meal or is not eating enough food, they are not putting enough glucose into their body to begin with, so the levels don’t get a chance to rise to where they need to be. If a patient gets too much exercise, their body is burning all of their glucose as energy (thanks to that escort insulin!) and they can exhaust their stores of glucose, which means the levels will be too low. Alcohol consumption and hypoglycemia Alcohol consumption can cause hypoglycemia in people with diabetes for an interesting reason that has to do with how our liver functions. If you remember from our overview of glucagon: Glucose is the sugar in our bloodstream that we can use for energy, and when it’s stored for later it’s converted to glycogen Glucagon is a hormone that controls these two processes in the liver: Glycogenolysis is when the liver converts glycogen back to glucose (for energy) GlucoNEOgenesis is when the liver forms NEW glucose (for energy) You can think of these processes as a safety net that makes sure you have enough glucose. But as you may already know, alcohol consumption is taxing on the liver. Alcohol is toxic, so the liver works hard to break it down so it doesn’t poison you. In fact, the liver is so busy when it’s breaking down alcohol that it can’t make you any new glucose at the same time. Your body no longer has the safety net to rely on. With alcohol in your system, and the insulin medications at work whisking the glucose away, blood glucose levels can quickly drop in a patient with diabetes. Signs and symptoms of hypoglycemia The signs and symptoms of hypoglycemia include hunger, irritability, confusion, diaphoresis, headache, shakiness, blurred vision, pale, cool skin, and decreased level of consciousness that can progress into a coma. Cold and clammy… need some candy! Nursing care of a patient with hypoglycemia When you have a patient in a hypoglycemic state, your objective is to bring their blood glucose levels back up. The method by which you will do this depends upon if the patient is conscious or unconscious. Hypoglycemia in conscious patients For a patient that is conscious, you will need to quickly provide 15g of a readily-absorbed carbohydrate, like in juice or milk. Re-check their blood glucose 15 minutes later. If the level is still under 70 mg/dL, you will administer another dose of carbohydrates. Once their blood glucose level is over 70 mg/dL, you want to provide the patient with a snack that contains both a protein and carbohydrate. In this scenario, you are prioritizing getting the blood glucose to a safer level, then the snack with protein will provide longer-term energy. Hypoglycemia in unconscious patients If a patient is unconscious, they aren’t going to be swallowing any juice, so you will need to inject glucagon through the intramuscular or subcutaneous route. Remember that glucagon is a hormone that prompts the liver to make some glucose. Glucagon and all the other essential diabetes meds you need to know about are covered in our Pharmacology Flashcards. After you give the glucagon, if your patient has not regained consciousness within 10 minutes, then you will administer another dose. Once your patient has regained consciousness and can safely swallow, then you can provide them a snack as explained above. Glucagon does cause nausea and vomiting, so monitor your patient to make sure they don’t just vomit up the snack you give them. DIABETIC KETOACIDOSIS (DKA) Diabetic ketoacidosis (DKA) is a life-threatening, rapid-onset complication of diabetes that causes increased blood glucose levels and ketones in the blood and urine. It happens primarily in people with Type 1 diabetes, but it’s not unheard of in Type 2. This is hyperglycemia, so it’s the opposite of the hypoglycemia we just learned about above. Risk factors Risk factors associated with DKA include an infection or illness, stress, or untreated/undiagnosed Type 1 diabetes. In Cathy’s experience, it’s common at the hospital for patients to show up with DKA at the emergency room and that is the first time that patient finds out they have Type 1 diabetes. Signs and symptoms Signs and symptoms of DKA are the same signs and symptoms as those of hyperglycemia which we just covered in our diabetes overview. Symptoms of DKA include the 3 Ps: polydipsia, polyphagia, and polyurea; weight loss, fruity breath odor, Kussmaul respirations, and dehydration. Lab values associated with DKA The lab values you need to know for DKA include blood glucose, ketones, metabolic acidosis, and hyperkalemia. Blood glucose Remember that the expected ranges for blood glucose are usually between 75-140 mg/dL depending on the type of test. In DKA, the blood glucose levels will be greater than 300 mg/dL — but under 600 mg/dL, because when blood sugar levels reach 600 mg/dL, we enter into hyperglycemic-hyperosmolar state (HHS) which we’ll cover next. Ketones Ketones are chemicals created by your body when it breaks down fat to use for energy. The body does this when it can’t use glucose, either because the glucose is depleted or because, in the case of DKA and HHS, there is not enough insulin to use all of the glucose that’s there. With DKA, the patient will have ketones in their urine and blood. What about the keto diet? Doesn’t that have something to do with ketones? You don’t need to know this for Med-Surg or Critical care, but we should explain so you are aware of it. Ketones are also the basis of a ketogenic diet or “keto,” which you have probably heard of by now. The idea behind a ketogenic diet is to keep carbohydrate intake extremely low, so that the body burns all of its glucose and switches to using stored fat for energy. When the body is burning fat for energy, it’s known as being in a state of ketosis. If you are in a state of ketosis due to the ketogenic diet, you have more ketones than someone eating a balanced diet, but not enough ketones to cause acidosis. Diabetic ketoacidosis is a life-threatening complication of diabetes where the body can’t use glucose for energy despite having a lot of glucose, and nutritional ketosis is a state achieved through diet where glucose intake is kept low on purpose. Metabolic acidosis DKA can put the patient’s body into metabolic acidosis, which means the blood is too acidic. When ketones build up in the bloodstream, they make the blood more acidic, which is where the -acidosis suffix of this disease comes from. Hyperkalemia Another lab value associated with DKA is hyperkalemia — when potassium levels are too high. The normal range for potassium is between 3.5 and 5.0 mEq/L. Potassium (K) levels over 5 mEq/L can indicate hyperkalemia, which can put the patient at risk for life-threatening dysrhythmias. The symptoms of hyperkalemia include dysrhythmias, muscle weakness, numbness/tingling, diarrhea, confusion. The K in DKA will remind you to monitor K! Hyperglycemic hyperosmolar state (HHS) Hyperglycemic-hyperosmolar state (HHS) is a serious complication of diabetes, also marked by very high glucose levels. HHS has a more gradual onset and is more common in type 2 diabetes. Two Hs in HHS, HHS is more common in Type 2 Risk factors Risk factors for HHS are older age, inadequate fluid intake, decreased kidney function, infection, and stress. Signs and symptoms The signs and symptoms of HHS are the signs and symptoms of hyperglycemia as described above, in addition to the signs and symptoms of dehydration, which includes hypotension, weak pulses, headache and weakness. Lab values associated with HHS Blood glucose Remember that the expected ranges for blood glucose are usually between 75-140 mg/dL depending on the type of test. In HHS, the blood glucose levels will be greater than 600 mg/dL, which is extremely high. Ketones Unlike DKA, there are no ketones present in the urine or blood with HHS, and thus no resultant metabolic acidosis. The reason why there are no ketones even though HHS blood sugar is doubly high, is because in patients with Type 2 diabetes, their body actually does produce some insulin, and so the body does not have to switch entirely to fat burning. It may be helpful to think of the two this way: In DKA, the body is unable to access its high level of glucose and thinks it’s starving, so switches to fat to save itself. In HHS, the body gradually got really high glucose and can access some of it for energy, so it doesn’t respond with that same emergency mechanism, even though it is still in grave danger. HHS is more fatal than DKA. TREATMENT OF DKA AND HHS The first step in treating DKA or HHS is to address any underlying causes, like an infection, illness, or acute stress. The body can’t respond to other treatments if it thinks it’s under attack. Administer IV fluids and insulin to the patient to help them become hydrated and process their blood glucose. Monitor blood glucose levels hourly, aiming to bring them under 200 mg/dL. If a patient has metabolic acidosis with DKA, administer sodium bicarbonate, an alkalinizing agent, to counter balance the acid in their blood (acid + alkaline = neutral). Potassium Closely monitor the patient’s potassium levels. When a patient first presents to the ER with DKA, their potassium will be very high. You will likely administer calcium gluconate to protect the heart from dysrhythmia. However, as you treat the patient with insulin, their blood potassium levels will naturally decrease. Remember that in addition to glucose, insulin also brings potassium from the bloodstream into the cells. Over the course of their treatment, the patient may end up with hypokalemia as their potassium is brought down. If that occurs, you may need to supplement their potassium to bring it back to a normal level. CHRONIC DIABETES COMPLICATIONS Diabetes can cause other serious complications over time, and there are a lot of associated risks. These are important to know as you will encounter them often throughout your nursing career. Cardiovascular disease Adults with diabetes are more likely to die of heart disease than adults without diabetes. Diabetes and cardiovascular disease have a correlated relationship because cardiovascular risk factors are common in people with diabetes, including obesity, high cholesterol and hypertension. Hyperglycemia can cause damage to the heart, making it more prone to heart failure. Neuropathy Diabetes can cause neuropathy, which is nerve damage that leads to numbness or shooting pains. Diabetes can cause neuropathy because hyperglycemia can damage nerves, as well as the blood vessels that serve oxygen to your nerves. In diabetic patients, neuropathy often happens to the feet, which makes the feet more prone to injury as we discussed in our previous video. Nephropathy Diabetes can cause nephropathy, which is kidney disease. Hyperglycemia can damage the kidneys through interruption of their filtering mechanism, as well as scarring. Kidney failure is a life-threatening condition that will require dialysis or a kidney transplant. Retinopathy Diabetes can cause retinopathy, which is damage to the blood vessels in the back of the eye caused by hypergylcemia. Mild cases that are caught early can be treated with carefully managed diabetes, but advanced cases may require laser treatment, surgery, or regular shots in the eye. Gastroparesis Diabetes can cause gastroparesis, which is a condition where your stomach doesn’t work properly to move food down. As we have mentioned, hyperglycemia can cause nerve damage, and one of the nerves that it can damage is the vagus nerve near the stomach, which can affect stomach function. With gastroparesis patients have nausea, vomiting, heartburn, and feel uncomfortable whenever eating, which can greatly reduce quality of life. Other complications Diabetes can also cause tooth decay, gum disease, and sexual dysfunction, among other things. There are many reasons to take diabetes seriously and manage it very closely to avoid complications. Let's first talk about hypoglycemia. That is defined as a blood glucose level under 70 mg/dL. What are some causes of hypoglycemia in diabetes patients? Well, if they have excess insulin, that can definitely cause hypoglycemia. If they skip a meal or just decrease their food intake, that can also cause hypoglycemia. Other causes include exercise, as well as excess alcohol. The signs and symptoms of hypoglycemia are important to remember. And those are all here on the back of card 46 [of the Medical-Surgical Flashcard deck]. So those include hunger, irritability, confusion, diaphoresis, headache, shakiness, blurred vision, pale, cool skin, and decreased level of consciousness that could progress into a coma. Regarding the skin, you remember when we were talking about hyperglycemia, I was like, "If the skin is warm and dry, sugar's high." With hypoglycemia, if the skin is cold and clammy you need some candy. So cold and clammy skin is definitely a sign of hypoglycemia. In terms of nursing care of a patient with hypoglycemia, if that patient is conscious and their blood sugar levels are under 70, you can give them 15 grams of a readily absorbed carbohydrate. So this can be a half a cup of juice or soda or like eight ounces of milk. Then you're going to want to recheck their blood glucose in about 15 minutes. If their blood glucose level is still under 70, then you'll want to give them another dose of carbohydrates, so some more juice or soda or milk. And then, again, recheck. Once their blood glucose level is over 70, then you want to provide the patient with a snack that contains both a protein and a carbohydrate. For your unconscious patient, you're going to want to provide glucagon through the IM or subcutaneous route. So my little saying to remember glucagon is, "When the glucose is gone, your patient needs glucagon." So if, after you give the glucagon, your patient has not regained consciousness within 10 minutes, then you're going to give them another dose of glucagon. Once your patient has regained consciousness and can safely swallow, then you can provide them a snack at that point. I will warn you that glucagon does cause nausea and vomiting so once your patient is conscious, you want to not only make sure they can safely swallow, you're going to also want to make sure that they're not going to just vomit up whatever snack you give them. So just something to keep an eye on. Now let's talk about DKA, which is diabetic ketoacidosis. This is a life-threatening complication of diabetes that causes increased blood glucose levels as well as ketones in the blood and urine. It is definitely more common with Type 1 diabetics, and it has a rapid onset. So some of the risk factors associated with DKA include an infection or illness, as well as stress and untreated or undiagnosed Type 1 diabetes. So often at the hospital, patients will show up with DKA at the emergency room and that is the first time that they find out that they have Type 1 diabetes. In terms of the signs and symptoms, because the patient will have hyperglycemia, we're going to see the same signs and symptoms that I talked about in my previous video associated with hyperglycemia. So this includes the three Ps-- so polydipsia, polyphagia, polyurea, as well as weight loss, fruity breath odor, Kussmaul respirations, and dehydration. Labs are going to be important to know how to differentiate DKA from HHS. So with DKA, blood glucose will be elevated over 300. And you will have ketones in the urine as well as the blood. That is different than HHS. HHS will actually have higher levels of blood glucose, often over 600. And there will be no ketones in the urine or blood. Also with DKA, we're going to see metabolic acidosis present in the patient, as well as hyperkalemia. And anytime we have an abnormality in potassium levels, either too high or too low, the patient is at risk for lifethreatening dysrhythmias. So when you see the word DKA, K is in the middle and that will help you to recall that you need to closely monitor the patient's potassium levels because they're going to be really high and that can definitely cause some life-threatening dysrhythmias, like I said. Now moving on to HHS. HHS stands for hyperglycemic hyperosmolar state. With HHS, we have very high glucose levels as well as severe dehydration. HHS has a more gradual onset and it is definitely more common with Type 2 diabetic patients. So if you look at the initials HHS, there are two Hs, which will hopefully remind you that HHS is more common with Type 2 diabetes. Some of the causes and risk factors associated with this condition include older age, inadequate fluid intake, decreased kidney function, as well as infection and stress. Signs and symptoms of HHS will include the signs and symptoms of hyperglycemia, which we've talked about a lot, in addition to the signs and symptoms of dehydration, which may include hypotension, weak pulses, headache, and weakness. In terms of the labs, blood glucose levels will be over 600, and there will be no ketones in the urine or blood and no metabolic acidosis present like we saw with DKA. Now, let's talk about the treatment of DKA and HHS. First of all, we're going to want to identify and treat any underlying cause of these complications. So if the patient has an infection, we're going to want to treat that infection. We're going to be administering IV fluids and insulin to the patient. We're going to want to check their blood glucose levels hourly. And our goal is to bring those levels under 200. If the patient has metabolic acidosis with DKA, we're going to administer bicarbonate. We're also going to closely monitor the patient's potassium [K] levels. So when the patient first presents to the emergency room with DKA, their potassium levels are going to be very high. And we're going to want to give them calcium gluconate to help protect the heart from dysrhythmia. However, as we treat the patient with insulin, insulin helps to bring glucose from the bloodstream into the cells. But it also brings potassium from the bloodstream into the cells. So over the course of treatment, the patient may end up with hypokalemia. And if that is the case, then we're going to want to replace their potassium as needed. The last thing I want to touch on in this video are some of the chronic complications of diabetes. There's a lot of them. And left untreated and not managed, diabetes can really ravage the body and cause so many problems. So as a nurse, you need to really provide education to your patient on these risks. So some of the complications associated with diabetes include cardiovascular disease, which can lead to a myocardial infarction as well as a stroke. Diabetic neuropathy, which can lead to neuropathic pain as well as foot injury and infection. It can cause nephropathy, so kidney damage, as well as retinopathy. So damage to the eyes which can lead to blindness. It can cause gastroparesis which can lead to impaired digestion, as well as tooth decay, gum disease, and sexual dysfunction. So there are so many reasons to really take diabetes seriously and manage it very closely to avoid these complications.